By Marcello Cherchi, MD PhD
For patients
Some patients who have suffered head trauma (with or without fracture of the temporal bone) develop fluctuating hearing loss and episodes of disequilibrium. These symptoms resemble Ménière’s disease, but despite the similarity, it is unclear whether this should be treated in the same way as Ménière’s disease (as some physicians suggest).
For clinicians
Around the mid-20th century case reports began to emerge of head trauma followed by fluctuating hearing loss and vertigo. Since the audiologic and vestibular characteristics resembled Ménière’s disease, these were sometimes referred to as “post-traumatic Ménière’s” (Gundrum 1959, Paparella and Mancini 1983, Lehrer and Poole 1984), but we prefer to reserve the term “Ménière’s” for the idiopathic syndrome.
Nevertheless, the idea that endolymphatic hydrops could be caused by a traumatic insult was popularized by Dr. Harold Frederick Schuknecht (Gulya and Schuknecht 1982, Schuknecht and Gulya 1983), and given his stature in the field (Nadol 1997), eventually the phrase post-traumatic endolymphatic hydrops entered the literature (DiBiase and Arriaga 1997).
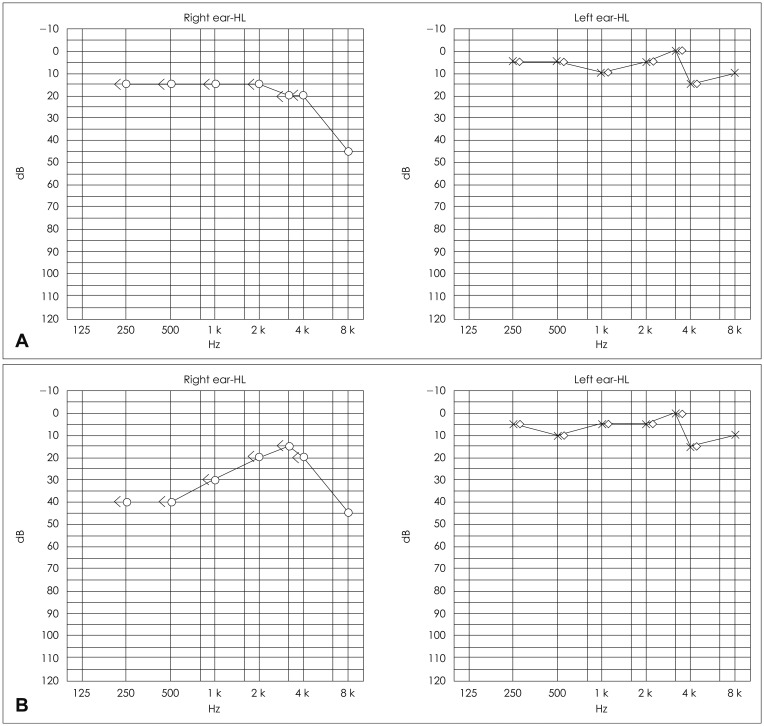
The Figure below, from Chung and colleagues (Chung, Jung et al. 2014), shows audiograms from a case of post-traumatic endolymphatic hydrops. The audiogram in Panel A is from the time of admission; the right side showed moderate hearing loss at 8 kHz. The audiogram in Panel B shows new right-sided moderate low frequency sensorineural hearing loss.
The mechanism of post-traumatic endolymphatic hydrops is unknown. Logically one would think that trauma causes disordered endolymphatic fluid flow, either from increased production, or decreased resorption, or both; this could in turn be due to alteration in the function of cells that produce/absorb these fluids, or abnormalities in the hydraulic system through which they pass (cochlear duct, endolymphatic duct, and vestibular aqueduct).
Head trauma can result in temporal bone fractures. Similar to cases of head trauma without temporal bone fractures, some of these patients develop hearing loss and disequilibrium. Consequently, hypothesized mechanisms for this similarly include post-traumatic endolymphatic hydrops (Lyos, Marsh et al. 1995, Johnson, Semaan et al. 2008), for which there is some histopathological evidence from temporal bone studies (Knoll, Ishai et al. 2020).
Audiometry from published cases is compatible with endolymphatic hydrops. We are not aware of systematic vestibular studies in such patients (such as electrocochleography, or tests for vestibular weakness), so in our view the degree to which post-traumatic endolymphatic hydrops matches idiopathic endolymphatic hydrops remains unclear.
Absent better guidance for treatment, it is probably medically reasonable to manage such cases according to their phenotype — meaning, these cases may be treated with strategies similar to Ménière’s disease — to a point. Applying relatively low-risk interventions (dietary sodium restriction, oral medications) seems reasonable. In contrast, we would approach ablative therapies (e.g., transtympanic gentamicin injection, vestibular neurectomy) with great caution.
References
Chung J, Jung HJ, Kim CS, Kim YH (2014) A Case of Post-Traumatic Meniere’s Disease. Korean J Audiol 18: 41-4. doi: 10.7874/kja.2014.18.1.41
DiBiase P, Arriaga MA (1997) Post-traumatic hydrops. Otolaryngol Clin North Am 30: 1117-22.
Gulya AJ, Schuknecht HF (1982) Classification of endolymphatic hydrops. Am J Otolaryngol 3: 319-22. doi: 10.1016/s0196-0709(82)80003-3
Gundrum LK (1959) Post-traumatic Meniere’s symptom-complex. Eye Ear Nose Throat Mon 38: 385-8.
Johnson F, Semaan MT, Megerian CA (2008) Temporal bone fracture: evaluation and management in the modern era. Otolaryngol Clin North Am 41: 597-618, x. doi: 10.1016/j.otc.2008.01.006
Knoll RM, Ishai R, Lubner RJ, Trakimas DR, Brodsky JR, Jung DH, Rauch SD, Nadol JB, Jr., Remenschneider AK, Kozin ED (2020) Peripheral Vestibular Organ Degeneration After Temporal Bone Fracture: A Human Otopathology Study. Laryngoscope 130: 752-760. doi: 10.1002/lary.28010
Lehrer JF, Poole DC (1984) Post-traumatic Meniere’s syndrome. Laryngoscope 94: 129. doi: 10.1288/00005537-198401000-00025
Lyos AT, Marsh MA, Jenkins HA, Coker NJ (1995) Progressive hearing loss after transverse temporal bone fracture. Arch Otolaryngol Head Neck Surg 121: 795-9. doi: 10.1001/archotol.1995.01890070081017
Nadol JB, Jr. (1997) Harold Frederick Schuknecht. 1917-1996. Audiol Neurootol 2: 168-70. doi: 10.1159/000259239
Paparella MM, Mancini F (1983) Trauma and Meniere’s syndrome. Laryngoscope 93: 1004-12. doi: 10.1288/00005537-198308000-00006
Schuknecht HF, Gulya AJ (1983) Endolymphatic hydrops. An overview and classification. Ann Otol Rhinol Laryngol Suppl 106: 1-20. doi: 10.1177/00034894830920s501
![]()