This web page is an edited version of a paper we published with colleagues Frank DiLiberto, Darío Yacovino and Sunit Das (Cherchi, DiLiberto et al. 2021).
For patients
The phrase “cervicogenic vertigo” (CV) refers to the idea that neck problems can disturb a person’s equilibrium. This idea is controversial, in part because there is not yet any definitive diagnostic test for it. Nevertheless, your doctor may suspect a diagnosis of CV if you have neck pain and disequilibrium, and there is no evidence for a more convincing diagnosis on tests of inner ear function. The best studied treatment modality is manual physical therapy for the neck.
For clinicians
Practical summary
Vestibular clinicians often encounter patients with neck symptoms and vertigo in whom it may seem logical to postulate a causal relationship between the two symptoms. The possible relationship between these has been given various labels in the literature; here we shall use the term cervicogenic vertigo (CV), but other terms include various permutations of “cervical”/”cervicogenic” and “vertigo”/”dizziness.”
The most popular theory is that cervicogenic vertigo is due to an abnormality in cervical proprioception. Etiologies such as vascular compromise, even if sometimes correct, probably account for only a modest proportion of cases.
There have been numerous attempts at developing a test for cervicogenic vertigo; none appears sufficiently sensitive or specific, and none has gained wide acceptance. It seems likely that this failure is at least in part due to the fact that the system in question involves multimodal sensory integration, and in practice it is difficult to manipulate selectively a single sensory modality while leaving the other modalities unchanged.
In the absence of a confirmatory test for CV, it remains a diagnosis of exclusion. Depending on the clinical scenario and findings on physical examination, additional workup may include otovestibular testing and imaging.
Physical therapy for the neck has been studied more than other treatment modalities, and is usually described as having favorable outcomes. Given our ignorance of the underlying mechanism of disease, it is difficult to understand why physical therapy should be helpful, but one possibility is that such therapy normalizes cervical mechanics and thereby interrupts the maladaptive positive feedback loop in which each symptom (vertigo, neck pain) exacerbates the other.
Cervicogenic vertigo more commonly provokes symptoms during positional changes and other movements. Such movements can also provoke other forms of vertigo, so when formulating a differential diagnosis for CV, it is prudent to keep in mind common causes as well, such as benign paroxysmal positional vertigo.
1. Introduction
Investigations of cervicogenic vertigo (CV) often appear motivated by the frequently encountered clinical scenario of a patient with neck symptoms and dizziness, in whom no other cause for the dizziness has been identified. Since mere co-occurrence does not prove causality, a skeptical audience would understandably eschew regarding CV as a “diagnosis,” and prefer the more neutral term, “syndrome.”
Discussions of cervicogenic vertigo (CV) usually characterize the idea as “controversial” (Brandt 1996, Kristjansson and Treleaven 2009, Li and Peng 2015), and acknowledge that the lack of a diagnostic test contributes to the controversy (Kristjansson and Treleaven 2009, Yacovino and Hain 2013, Hain 2015, Peng 2018).
Most medical phenomena that eventually come to be accepted as diagnoses began as unproven ideas; as hypotheses that required testing. Since the absence of proof is not proof of absence, we should remain receptive to the possibility of progress on this topic, and that the controversy surrounding CV may ultimately be resolved.
With these points in mind, we shall review why CV is controversial, beginning with an appraisal of candidate mechanisms for its pathophysiology, how these mechanisms could be tested, why tests have failed, and a more general discussion of why it has proven so difficult to devise a sensitive and specific test. We conclude with a brief review of treatments.
The literature regarding CV spans nearly a century, and in reviewing this, we have been struck by the degree to which paraphrasing the text of a previous author appears often to result in changing the earlier article’s intent. In the interest of accurately conveying the thought of previous authors, we have elected generous use of direct quotations in the present review.
2. Assumptions, definitions, and conditions
For purposes of this discussion, we shall make the initial simplifying assumption that cervicogenic vertigo (to be defined presently) is the only source of symptoms—though later we shall also mention why this assumption is faulty.
We take the term “vertigo” in its technical sense as referring to a kinetic illusion; a discrepancy between perceived versus actual motion/stasis. While we would prefer a more neutral term such as “disequilibrium” or “dizziness,” the word “vertigo” has become quite entrenched in the literature since Ryan and Cope’s 1955 paper on the subject (Ryan and Cope 1955). Some readers may take the term “vertigo” to refer more narrowly to a sensation of rotation, but many authors note that such a sensation is actually uncommon in CV (Wrisley, Sparto et al. 2000, Yacovino and Hain 2013). The term “cervicogenic” designates that the underlying mechanism of vertigo arises from (is “generated” by) a problem in the cervical region—in other words, the definition requires a causal relationship, whereby a cervical problem provokes vertigo.
Most research on CV requires that (explicitly or implicitly) in order to entertain a diagnosis of CV, either (1) neck symptoms must be present (pain; head-on-neck and/or neck-on-trunk movement that is limited, excessive, uncontrolled, unintended, irregular, etc.), and these neck symptoms must temporally overlap with the symptom of vertigo; or (2) there is a history of neck injury that precedes the development of the symptom of vertigo; or (3) both (Wrisley, Sparto et al. 2000, Li and Peng 2015, Thompson-Harvey and Hain 2019).
3. Immediate problems
When one attempts to apply these assumptions, definitions, and conditions to clinical cases, several problems become immediately apparent.
The first problem pertains to the relationship between cervical disease and vertigo; while the definition of CV requires that cervical disease be the cause of vertigo, there are, of course, other possible relationships.
One possibility is that the temporal overlap of symptoms may hold, but the causal relationship does not—in other words, the relationship is one of coincidence rather than causality (van Leeuwen and van der Zaag-Loonen 2017). This possibility merits consideration because neck pain and vertigo are each very common human experiences, and even when each symptom results from an independently occurring etiology, the likelihood of temporal overlap (coincidence) by random distribution is not small. Neck pain is common and appears to be increasing; the prevalence among adults aged 25–84 in the US was 14.8% in 2002 and 17.2% in 2018 (Zajacova, Grol-Prokopczyk et al. 2021); similar demographics are reported in other countries (Rydevik, Szpalski et al. 2008). In the US, dizziness and vertigo accounted for 20.6 million ambulatory care visits per year in 2013–2015 (Dunlap, Khoja et al. 2019), and for approximately 4 million emergency department visits in 2011 (Saber Tehrani, Coughlan et al. 2013). Thompson-Harvey and Hain capture this idea by noting that “The main clinical problem in diagnosing cervical vertigo is that symptoms of subjects who have both neck disorders and dizziness may overlap… In other words it is difficult to differentiate between the chance coincidence of arthritis of the neck and dizziness, from the situation where arthritis of the neck causes dizziness” (Thompson-Harvey and Hain 2019).
Another possibility is that the temporal overlap of symptoms may hold, but the relationship is reversed; instead of neck pathology causing vertigo, the vertigo causes the neck symptoms. Patients with vertigo of any cause often unconsciously make compensatory postural adjustments, and neck symptoms may ensue(Brandt and Bronstein 2001, Yacovino and Hain 2013); in other words, the neck symptoms may be an effect of the vertigo, rather than its cause.
The second problem pertains to the relationship between CV and neck injury. Hain states that, “inner ear disorders are rare after neck trauma” (Hain 2015), citing Mallinson and Longridge (Mallinson and Longridge 1998). However, most injuries are not so focal as to affect the neck in isolation; in fact, whiplash—the most common neck injury, in whose context cervicogenic vertigo is suspected—is usually not a “pure neck injury.” Yacovino and Hain note that “Postwhiplash vertigo can combine several mechanisms. At the ear level, the otolith system is prone to suffer inertial damage” (Yacovino and Hain 2013), and several authors have noted that benign paroxysmal positional vertigo can result from acceleration-deceleration injuries (Vibert and Hausler 2003, Rydevik, Szpalski et al. 2008, Lee, Park et al. 2011). More broadly, “Dizziness following neck injury may be due to vestibular system pathologies, brain injury, or cervicogenic dizziness” (Wrisley, Sparto et al. 2000), including “the ear (labyrinth contusion), the brainstem, the cortical and subcortical structures, and the vertebral arteries (traumatic artery dissection)” (Yacovino and Hain 2013). The analytically desirable simplifying assumption we mentioned earlier (CV is the only source of symptoms) often does not hold in the real-world laboratory of clinical medicine; neck injuries are a good example where this assumption often fails. Finally, a significant proportion of neck-injury-related CV cases is composed of whiplash injuries, and patients in many such cases are in (or are contemplating) litigation. The medico-legal dimension of whiplash injuries (Pearce 1989) introduces considerations beyond anatomy and physiology whose influence on symptoms (which are subjective reports) is difficult to assess, and which have the potential to complicate analysis by introducing psychological components (Walton and Elliott 2017), and the possibility of secondary gain.
4. Underlying physiology
Discussions of CV usually assume a physiologic framework in which there is integration of multiple sensory inputs with planned output, and then there are multimodal outputs. An example of this view is evident in the following: “The results of several studies suggest that the control of posture, perception of the orientation of the body, and the location of objects in extrapersonal space requires an integration of proprioceptive, visual, and vestibular signals as well as internally generated signals related to intended head and body movements” (Gdowski and McCrea 1999), sometimes referred to as “efference copies” or “corollary discharges.” Efference copies refer to cortical constructs that serve to anticipate head-body position under a range of conditions and predict the appropriate motor response. These constructs are modified throughout life based on experienced sensory feedback.
The Figure below, from Kristjansson and Treleaven (Kristjansson and Treleaven 2009), is a schematic of the multisensory integration and output relevant for CV.
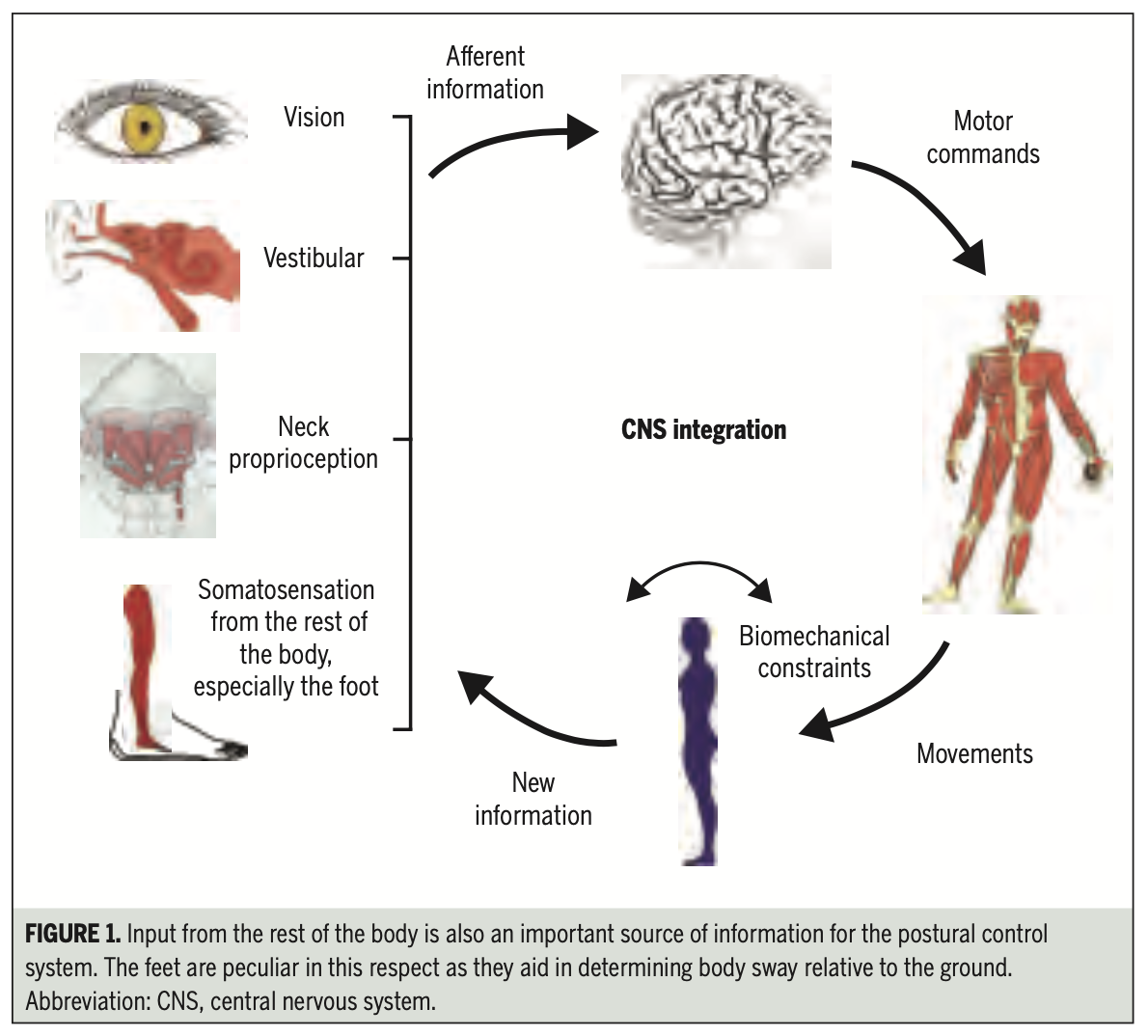
For an individual to perceive correctly her orientation in, and movement through, space, the brain must, at some level, solve the problem of a coordinate transformation (mapping from the coordinate system of one frame of reference to that of another frame of reference) (Mergner, Siebold et al. 1991, Mergner, Huber et al. 1997). Brandt described this well:
“It is necessary for the sensorimotor control system to know the attitude of the head relative to the body, since the vestibular system signals only head motion relative to space and head position relative to the gravity vector. The head-mounted sensory systems must transform the rotations and accelerations they sense and correctly relate their direction to the motion and attitude of the body and the center of gravity. Neck afferents provide information about head position, and make an important contribution to the control of body and sensory spatial orientation. The perception of head or trunk rotations in space would be erroneous if only vestibular stimulation or only neck stimulation was involved. However, if the two stimuli are combined (head rotations relative to the trunk), the perception of both trunk and head rotation in space reflects the true position” (Brandt 1996).
Although this is a “computationally difficult adjustment between the two coordinate systems of the head and body” (Yacovino and Hain 2013), there is nevertheless reasonable evidence that such a coordinate transformation does take place. Specifically, studies from primates “conclude that sensory vestibular signals are transformed from head-in-space coordinates to trunk-in-space coordinates on many secondary vestibular neurons in the vestibular nuclei by the addition of inputs related to head rotation on the trunk. This coordinate transformation is presumably important for controlling postural reflexes and constructing a central percept of body orientation and movement in space” (Gdowski and McCrea 1999).
A failure of multisensory integration (the process of reweighting and combining multiple input streams to produce a coherent perception) is the most commonly postulated mechanism underlying the idea of CV, with the failure being attributed to presumed erroneous proprioceptive cervical signals. Again, Brandt states:
“Somatosensory signals from musculotendinous receptors in the neck and joints provide an accurate kinesthetic feedback of the extent of head and limb movements. These signals contribute to the perception of self-motion during active locomotion by converging with vestibular and visual input on multimodal neurons in the vestibular nuclei and thalamus, which project to cortical multisensory areas in the parietal lobe” (Brandt 1996).
We will now review these, and other potential etiologies of disequilibrium related from the neck.
5. Candidate pathophysiological mechanisms
A number of pathophysiological mechanisms have been proposed to underlie CV. Some of the main ones are:
- Hypoperfusion. Neck movements may result in physical compromise of arteries in the neck by torque or compression, resulting in reduced blood flow to the brainstem. Another possibility is that neck movements may induce autonomic responses (e.g., through stimulation of carotid baroreceptors), also resulting in hypoperfusion.
- Anatomic. In an individual with craniocervical instability, neck movements may provoke brainstem compression.
- Ocular motor. Neck movements, through a variety of mechanisms, may induce abnormal ocular motor responses.
- Proprioception. In a diseased neck, neck movements may generate aberrant proprioceptive signals.
- Motoric. In a diseased neck, neck movements may incorrectly modulate efferent motor signals.
- Migraine. Neck disease may trigger migraine, and migraine can cause vertigo. Another possibility is that migraine causes both neck discomfort and vertigo.
We will discuss each in the following sections.
5.1. Hypoperfusion
Hypoperfusion, secondary to vascular compromise, is often discussed as a mechanism of CV. Rotational vertebral artery syndrome (RVAS), also called bowhunter syndrome, is a condition in which one of the vertebral arteries is transiently extrinsically compressed during neck rotation (Kamouchi, Kishikawa et al. 2003, Sakaguchi, Kitagawa et al. 2003, Weintraub and Khoury 2004, Helton and Bavry 2009, Mitchell 2009, Lu, Zador et al. 2010, Cornelius, George et al. 2012, Go, Hwang et al. 2013, Sarkar, Wolfe et al. 2014, Zaidi, Albuquerque et al. 2014, Duan, Xu et al. 2016, Araz Server, Edizer et al. 2018, Li, Xie et al. 2019). This appears more likely to provoke symptoms if the contralateral vertebral artery is already narrowed, such as by atherosclerotic disease. In some cases, this compression, perhaps combined with torquing of the artery, results in damage to the artery itself, such as a dissection (Vibert, Rohr-Le Floch et al. 1993). There are a few reports of RVAS manifesting with predominantly downbeat nystagmus (Choi, Shin et al. 2005, Ogawa, Itani et al. 2014), though such a pattern of nystagmus is not specific for the condition. If the vascular compromise is prolonged, it may culminate in infarction (Sorensen 1978). The discussions of RVAS are based primarily on case reports or small case series. Despite the apparent enthusiasm in the literature, this condition probably comprises only a small proportion of cases of CV. There is no consensus on the range of effects that neck turning can have on the vertebral arteries (Mitchell 2007), and while dynamic vascular imaging can provide corroborative evidence of RVAS, Hain (Hain 2015) pointed out that “Vertebral artery blood flow is compromised with full contralateral rotation in healthy individuals,” citing Mitchell (Mitchell 2009); thus, vascular imaging is not specific for this condition. Further, cadaveric animal model evidence suggests typical physiologic motions at the neck produce vertebral artery strains substantially lower than the failure point (dissection) (Symons, Leonard et al. 2002). An even less common mechanism of vascular compromise occurs in Chiari malformations, in which neck rotation torques the structures at an already crowded foramen magnum (Rousseaux, Salomez et al. 1983).
Hypoperfusion secondary to an autonomic abnormality triggered by neck rotation has been discussed in several forms. Barré–Lieou syndrome, proposed by Jean-Alexander Barré (Barré 1926) and Young-Choen Lieou (Lieou and Barré 1928), was thought to be the result of mechanical stimulation of paravertebral sympathetic ganglia during neck rotation. This theory was accepted by some early investigators (Jongkees 1969), but ultimately “No sympathetic or vascular changes were subsequently identified that could account for these symptoms and this theory lost favor” (Wrisley, Sparto et al. 2000), so the idea was dismissed by subsequent researchers, who state that “Positional nystagmus cannot be attributed to a disturbance of the cervical sympathetic chain as suggested by Barré” (Brandt 1996); see also Foster et al. (Foster and Jabbour 2007). A more plausible mechanism of autonomically-mediated hypoperfusion is “head turning-induced hypotension” (Schoon, Olde Rikkert et al. 2013) triggered by stimulation of overly sensitive carotid sinus baroreceptors during neck rotation. This should be detectable on physical examination.
5.2. Anatomic
Distortion of the anatomy at the craniocervical junction, such as in patients with craniocervical instability in whom neck movements may provoke brainstem compression (Rousseaux, Salomez et al. 1983), has been postulated as a mechanism for CV. This should be detectable on imaging. Given the neuroanatomical territory involved, brainstem compression should manifest with symptoms beyond simply vertigo.
5.3. Ocular motor abnormalities
Reports have documented a variety of ocular motor abnormalities occurring in association with neck rotation or neck pain; usually these appear to be abnormalities in the cervico-ocular reflex (Takemori and Suzuki 1971, Huygen, Verhagen et al. 1991, Kelders, Kleinrensink et al. 2005), but reports also describe other “Deficits in oculomotor control, such as decreased smooth pursuit velocity gain, altered velocity and latency of saccadic eye movements” (Kristjansson and Treleaven 2009). Some investigators have gone so far as to say that “The smooth pursuit neck torsion test developed by Tjell et al. (Tjell and Rosenhall 1998) is considered to be specific for detecting eye movement disturbances due to altered cervical afferent input” (Kristjansson and Treleaven 2009), but we will discuss below that this was not borne out.
5.4. Proprioception
Perhaps the most popular theory about CV pertains to cervical proprioception. Note that “Proprioception is not a function of the superficial neck muscles but of the deep short intervertebral neck muscles, which are extensively supplied with muscle spindles” (Brandt 1996), and in fact, “Of all the muscles in the body, it is the deep neck muscles that have the highest concentration of muscle spindles” (Rydevik, Szpalski et al. 2008). As a result, “The proprioceptive system of the cervical spine… is extremely well developed, as reflected by an abundance of mechanoreceptors, especially from the gamma-muscle spindles in the deep segmental upper cervical muscles” (Foster and Jabbour 2007), and “The dense network of mechanoreceptors in the soft tissues in this region… gives the CNS information about the orientation of the head with respect to the rest of the body via direct neurophysiological connections to the vestibular and visual systems” (Kristjansson and Treleaven 2009). Specifically, “Strong connections have been demonstrated between the cervical dorsal roots and the vestibular nuclei with the neck receptors (such as proprioceptors and joint receptors) playing a role in eye-hand coordination, perception of balance, and postural adjustments” (Wrisley, Sparto et al. 2000). Brandt and Bronstein (Brandt and Bronstein 2001) point out that studies of various kinds of neck stimulation can alter perception. Specifically, “Unilateral electrical stimulation of the neck (Wapner, Werner et al. 1951) causes deviation of the subjective vertical” and “Vibration of neck muscles, which stimulates the primary endings of the muscle spindles as if the muscle were being stretched (Matthews 1966) elicits an illusion of head tilt and apparent movement of a visual target (Biguer, Donaldson et al. 1988)”.
Such data, as well as evidence from experiments involving injection of anesthetics into the neck, “leads to the current theory that cervicogenic dizziness results from abnormal input into the vestibular nuclei from the proprioceptors of the upper cervical region” (Wrisley, Sparto et al. 2000). While there may be compelling evidence of erroneous cervical proprioception, this in itself does not necessarily explain why that altered sensory input would manifest as vertigo. There are two plausible mechanisms.
The first manner in which erroneous cervical proprioception could manifest with vertigo is through “sensory mismatch”—which is to say a discrepancy between the erroneous input from cervical proprioception, and the correct input from vision and the inner ear (Foster and Jabbour 2007, Kristjansson and Treleaven 2009, Hain 2015, Thompson-Harvey and Hain 2019).
The second manner in which erroneous cervical proprioception could manifest with vertigo is through a mismatch between intended movement (“efference copy” or “corollary discharge”) and erroneously perceived actual movement; as Brandt comments, “a multisensory mismatch would be expected to result in CV… the resultant mismatch would be maximal during active head movements (when expected and actual reafferent input do not match)” (Brandt 1996). Evaluation of this possibility has been attempted with “cervical repositioning tests” (Kristjansson and Treleaven 2009), and “joint position error” tests (Treleaven, Jull et al. 2006, L’Heureux-Lebeau, Godbout et al. 2014).
5.5. Motor Mechanism
While most discussions of the mechanism of CV focus on a problem with input, the possibility of altered motor output is rarely mentioned. This hypothesis maintains that CV is due to impaired motor activity, perhaps due to incorrect modulation of motor pathways arising from an abnormality in the neck, and that this motoric impairment is truly manifesting with unsteadiness that the patient is correctly perceiving. These patients generally have normal motor examinations, so if this hypothesis is correct, then the findings may be more subtle than what is discernible on physical examination. Our group tried to evaluate this idea with triceps vestibular evoked myogenic potentials (Cherchi, Bellinaso et al. 2009, Cherchi, El-Kholy et al. 2015, Shirley, Cherchi et al. 2015), on the hypothesis that vestibulospinal reflexes may be impaired, but we failed to identify any findings specific to patients whose histories were compatible with CV.
5.6. Migrainous Mechanism
Yacovino and Hain proposed migraine as a mechanism for CV in the form of “migraine-associated cervicogenic vertigo” (Yacovino and Hain 2013). This concept is beginning to gain traction among other investigators (Li and Peng 2015). Thompson-Harvey and Hain (Thompson-Harvey and Hain 2019) noted that a carefully constructed questionnaire was unable to distinguish CV from migraine-associated vertigo. There are actually two possibilities covered by this idea.
The first possibility is that neck problems may trigger migraine (Bartsch and Goadsby 2003, Piovesan, Kowacs et al. 2003, Bartsch 2005, Wober, Brannath et al. 2007, Pradhan and Choudhury 2018), and migraine can cause vertigo (Neuhauser, Leopold et al. 2001, Beh, Masrour et al. 2019, Hain and Cherchi 2019); on this hypothesis, neck problems are the initial trigger for migraine, and migraine in turn causes vertigo.
The second possibility is that migraine may manifest with both neck pain (Blau and MacGregor 1994, Kelman 2005, Schoonman, Evers et al. 2006, Calhoun, Ford et al. 2010, Blaschek, Milde-Busch et al. 2012, Lampl, Rudolph et al. 2015, Pradhan and Choudhury 2018, Ozer and Benlier 2020, Dornhoffer, Liu et al. 2021) and vertigo (Neuhauser, Leopold et al. 2001, Beh, Masrour et al. 2019, Hain and Cherchi 2019); on this hypothesis, migraine is the common underlying etiology of both symptoms.
The idea of a relationship between migraine, neck pain, and vertigo is attractive in the sense that it suggests a unifying diagnosis, but its limitation is that it exchanges one untestable diagnosis (CV) with another (migraine-associated vertigo). However, one merit of this theory is that it opens a potential avenue for treatment (migraine prophylaxis).
6. Attempts at developing objective diagnostic tests and their failures
The range of hypothesized pathophysiological mechanisms for CV has led to a corresponding range of attempts at developing a test for CV. Some of the main ones are:
- Imaging. Imaging is usually intended to detect vascular compromise triggered by head-on-neck rotation, and thus include various types of angiography (CTA, MRA, transcranial Doppler ultrasound, dedicated catheter angiography).
- Posturography. Computerized dynamic posturography was originally designed to assess vestibular, visual, and proprioceptive contributions to an individual’s unsteadiness. Its utility in CV has also been explored.
- Ocular motor studies. A range of ocular motor findings have been reported in CV, including abnormalities in spontaneous nystagmus, smooth pursuit, caloric responses, optokinetic after-nystagmus, and cervico-ocular reflex responses.
We shall review each of these in the following sections.
6.1. Imaging
This usually is employed to investigate the possibility of dynamic vascular compromise. As discussed earlier, this may help corroborate clinical suspicion for pathologies such as rotational vertebral artery syndrome, but since normal subjects can exhibit similar imaging, the finding is not specific for RVAS (Mitchell 2009, Hain 2015).
6.2. Posturography
Numerous studies have explored computerized dynamic posturography in patients with possible CV (Norre, Forrez et al. 1987, Rubin, Woolley et al. 1995, Karlberg, Johansson et al. 1996, Karlberg, Magnusson et al. 1996, Koskimies, Sutinen et al. 1997, Kogler, Lindfors et al. 2000, Williams, Tarmizi et al. 2017, Micarelli, Viziano et al. 2021). However, “increased postural sway is a nonspecific finding that is also evident in patients with vestibular injury” (Wrisley, Sparto et al. 2000). Moreover, “postural instability can be simulated” (Hain 2015).
6.3. Ocular motor studies
Since relevant multisensory inputs converge at the vestibular nuclei (Brandt 1996, Gdowski and McCrea 1999, Wrisley, Sparto et al. 2000, Foster and Jabbour 2007) whence efferent pathways project to the oculomotor nuclei, it is logical to explore whether CV manifests with ocular motor abnormalities. A variety of ocular motor findings have been reported in patients with clinical histories compatible with CV (Johnston, Daye et al. 2017), including abnormalities in smooth pursuit, abnormal caloric responses, spontaneous and positional nystagmus (Wrisley, Sparto et al. 2000), latent nystagmus, and abnormalities on rotatory chair testing (Toglia 1976). Unfortunately, these have proven neither sensitive nor specific for CV. We will review several ocular motor tests that have been explored: smooth pursuit, optokinetic after-nystagmus, and the cervico-ocular reflex.
6.4. Smooth pursuit
Some investigators report abnormalities of smooth pursuit in whiplash patients with dizziness (Gimse, Tjell et al. 1996, Tjell and Rosenhall 1998). However, “Smooth pursuit is a complex multiple input system that is vulnerable to cognitive variables, age, and sedation. Neck pain and secondary gain, both disruptive of cognition, would also seem highly likely to influence performance of smooth pursuit. For these reasons, due to an intrinsic issue with specificity, it seems unlikely that any smooth-pursuit test could be of general utility for the diagnosis of cervical vertigo” (Yacovino and Hain 2013).
6.5. Optokinetic after-nystagmus
It has been hypothesized that optokinetic after-nystagmus may be abnormal in CV patients (Karlberg and Magnusson 1996). However, “Optokinetic after-nystagmus is difficult to obtain in humans and is generally of small velocity even in normal subjects. This makes it unlikely that this test could be sufficiently sensitive to be useful in cervical vertigo” (Yacovino and Hain 2013).
6.6. Cervico-ocular reflex on the head-still trunk-rotates protocol
One ocular motor testing protocol merits special attention. Fixing the head in space (thus neutralizing labyrinthine input) while oscillating the trunk underneath (Jongkees 1969, Takemori and Suzuki 1971, Huygen, Verhagen et al. 1991, Kelders, Kleinrensink et al. 2005) should, in theory, come close to selective manipulation of proprioceptive cervical input, and an output such as eye movements could then be analyzed. A passive version of this test has been studied (de Jong, Bles et al. 1981). An active version of this test—in which the subject has to attempt to keep the head stationary by pointing a “gunsight” laser at a stationary target while the trunk rotates beneath—has also been studied (Guitton, Kearney et al. 1986).
The Figure below, from Jongkees (Jongkees 1969), shows the experimental setup in which the patient’s head is maintained in a fixed position (in space) while the body rotates underneath.
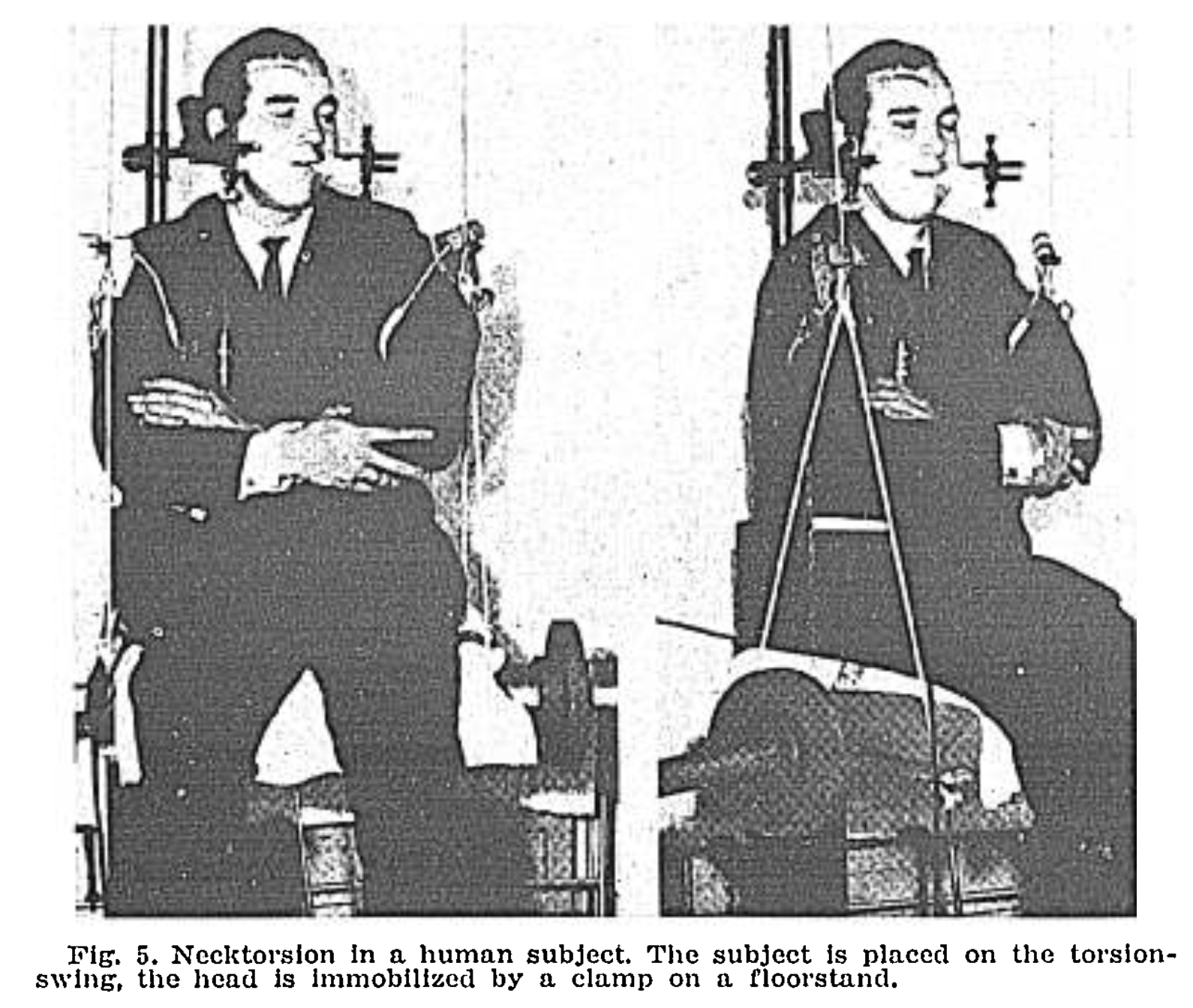
While this test strikes us as very logical, it has proven neither sensitive nor specific for CV (Treleaven, Joloud et al. 2020). In greater detail, the “test of cervical rotation, actually a test of the cervico-ocular reflex, consists of rotating the body about the earth’s vertical axis, while keeping the head still in space, and evaluating for nystagmus. This procedure has not been widely accepted… The cervico-ocular reflex also appears in other conditions, such as bilateral vestibular loss thus even if it were sufficiently sensitive, the finding of a cervico-ocular reflex could not be… a specific test for cervical vertigo” (Yacovino and Hain 2013). Moreover, Brandt (Brandt 1996) notes that “Cervical nystagmus also occurs in healthy subjects,” citing Norre (Norre 1987). It further turns out that even in normal subjects it is possible to induce asymmetry in the vestibulo-ocular reflex by passive sustained turning of the head-on-trunk (Padoan, Karlberg et al. 1998).
A more detailed explanation of this from Wrisley et al. (Wrisley, Sparto et al. 2000) is that:
“The neck torsion nystagmus test, or head-fixed, body-turned maneuver is considered by some to identify cervicogenic dizziness [(Philipszoon and Bos 1963)]. This test requires the head of the patient to be stabilized while the body is rotated underneath [(Norre 1987, Fitz-Ritson 1991)]. Theoretically, the neck proprioceptors are stimulated while the inner ear structures remain at their resting state [(Norre 1987)]. Nystagmus is elicited in a positive test. However, this test has not been demonstrated to be specific for cervicogenic dizziness. Oosterveld et al. [(Oosterveld, Kortschot et al. 1991)] reported that 64% of 262 patients with neck pain who presented to an otolaryngology department post-whiplash had nystagmus elicited with the head-fixed, body-turned maneuver. On the other hand, it has been demonstrated that up to 50% of subjects without cervical spine pathology have also demonstrated nystagmus with the head-fixed, body-turned maneuver [(Philipszoon and Bos 1963, Calseyde, Ampe et al. 1977, Norre 1987)]. A positive response (nystagmus) may not indicate pathology, but may instead be a manifestation of the cervical ocular reflex [(Norre 1987)]”.
6.7. Why has testing for CV failed?
It seems that it should be possible to isolate individual sensory inputs, with the relevant one for CV being proprioception. Yet, this has proven challenging to study. A few comments from investigators allude to this problem.
“Postural control is achieved through a multisensory control mechanism involving visual, vestibular and somatosensory information. These inputs are all interconnected allowing compensation of dysfunctions but making it very challenging to study the cues of one particular system without interference of another” (Freppel, Bisdorff et al. 2013).
“The neck not only modulates body posture, but it also stabilizes the head in space by cervicocollic reflexes, which are similarly integrated with vestibulocollic reflexes. In healthy human beings, neck reflexes form part of the multisensory postural control mechanism, thus making it impossible for the clinician to carry out a selective test of neck function by simple postural maneuvers” (Brandt 1996).
Essentially, it has proven difficult to manipulate selectively an individual input in complete isolation from the other inputs.
Thus, the failure to develop a test that is specific and sensitive for CV is due, at least in part, to the complex organization of the system, and in particular to its multi-modal nature. The input (perception of movement and of orientation) and output (execution of movement for maintenance of equilibrium) is a process that involves multimodal sensory afferents (vestibular, vision, proprioception), integration of those inputs, and multimodal efferents (ocular motor, somatomotor). This system has advantages and disadvantages. An example of an advantage for a patient is that the multiple inputs are not completely overlapping, but insofar as they do overlap and provide concordant information, this redundancy makes the system more resilient. An example of a disadvantage for a patient is that when the sensory inputs are discordant, the resulting mismatch can be perceived as vertigo. A chief disadvantage for the investigator is that it is difficult to manipulate selectively a single input while maintaining the other inputs constant.
If a successful test were to be developed, what might it look like?
A general principle of sensory input is that biological sensors are better at detecting change (dynamic stimulation) than stasis (constant stimulation) (Gray and Malcolm 1950). This general principle underlies Brandt’s idea that “a multisensory mismatch would be expected to result in CV… the resultant mismatch would be maximal during active head movements (when expected and actual reafferent input do not match)” (Brandt 1996), which in turn leads to his suggestion that “Since assessment of all these measures under static conditions has so far proven inconclusive, further investigations should focus on dynamic studies” (Brandt 1996).
Given these considerations, if a test is ever devised that successfully identifies cervicogenic vertigo (and distinguishes it from other diseases), it seems likely that the test will involve dynamic input, probably in the form of some change in position. Until such a test is developed, we need to bear in mind that patients with suspected cervicogenic vertigo usually perceive their symptoms to be more pronounced during movement.
6.8. Dynamic testing may be more sensitive than static testing, but…
However, a test that involves a change in position will still run the risk of stimulating multiple inputs. Positional changes can trigger vertigo in diseases other than putative CV, of course. Yacovino and Hain (Yacovino and Hain 2013) pointed out that four out of the five cases reported in the very paper that gave us the term “cervical vertigo” (Ryan and Cope 1955) sound much more like benign paroxysmal positional vertigo (BPPV). Let us review the cases described by Ryan and Cope.
Case 1: “A man, aged 57, had been in excellent health… While he was building a wall a brick had struck him in the head; his neck was flexed at that time and the blow jarred his neck to one side… On lying down that night he had a sudden and fairly severe attack of vertigo — ‘everything started going round and I felt sick.’ He did not vomit, and after a minute or two the vertigo subsided; but the neck pain did not allow him much sleep… He was… placed flat on a couch, and his head and trunk lowered over the end… At once he complained of vertigo, and we noticed that nystagmus appeared in association with this symptom. The vertigo and nystagmus occurred irrespective of whether the head was to the left, central, or to the right, and disappeared if the patient maintained his position for a little time.”
Case 2: “A man, aged 60, was involved in an explosion… and he subsequently complained of pain and paresthesiae in the arms… He was subjected to manipulation, and thereafter slow neck traction was applied… Three days later on getting up in the morning he had an acute attack of vertigo and fell to the left. There was no vomiting, sweating, or syncope. On trying to move to the right or the left he experienced vertigo and was unable to walk straight. He stayed in bed for a week and then got up cautiously, finding that the vertigo was brought on only by rapid movement of the head. The symptoms slowly diminished and had disappeared within two weeks.”
Case 4: “A married woman, aged 45… fell on to the base of her spine and also injured the back of her head… She… had slight pain in the occipital region. About three weeks after this injury she was wakened in the night by a throbbing sensation in the right side of her neck; and in the morning she sat up in bed, felt her head swimming, and fell to the left. This sensation, which was momentary, was accompanied by slight nausea. About ten minutes later she ‘felt fine,’ and got up to do her housework. Just before luncheon she looked up at the warming-rack and then bent down to attend to the stove, and immediately the kitchen ‘seemed to spin round’ to the left, and she fell on her left side.”
Case 5: “A married woman, aged 40, slipped and fell on the back of her head… The next day she had a severe pain in the occipital region… Some time later she had a severe attack of vertigo, with a feeling that her environment was rotating in a clockwise direction. Since then the attacks had occurred twice a week, and on two occasions she had fallen to the ground and bruised herself.”
These cases all sound like attention was being drawn to the neck due to the circumstances in which the patient was injured, but the descriptions of the vertiginous symptoms themselves and their positional triggers are far more suggestive of benign paroxysmal positional vertigo; the cervical symptoms are more likely to be “distractors.” In other words, these were probably patients with BPPV that happened to be occurring in the context of trauma to the head or neck. Since BPPV is the most common cause of vertigo (von Brevern, Radtke et al. 2007), it is statistically likely that its occurrence will coincide with that of other diseases (such as neck pain, head trauma, etc.).
Bear in mind that when Ryan and Cope were writing in 1955, benign paroxysmal positional vertigo had barely been described. In 1920, Robert Bárány (Bárány 1920) described a case of a young woman who had been suffering from vertiginous episodes triggered by lying on her right side. Numerous similar cases were described subsequently, and in 1952, Margaret Ruth Dix and Charles Skinner Hallpike (Dix and Hallpike 1952, Dix and Hallpike 1952) described their own cases of “positional nystagmus,” noting that symptoms (and simultaneous nystagmus) were induced “by a critical position of the head in space.” Ryan and Cope appear to have been aware of the work of Dix and Hallpike since they cite one of their 1952 papers, but in reading Ryan and Cope’s paper with hindsight, it seems likely that the “cervical circumstances” in these cases were distractors from the true pathology.
This reinforces the point made by other investigators that “Benign paroxysmal positional vertigo (BPPV) is often misdiagnosed as cervical vertigo” (Li and Peng 2015), or more generally, “Lesions of the vestibular organs, particularly the otolithic organs, after whiplash injuries are probably underestimated by attributing dizziness and vertigo symptoms mainly to cervical damage and lesions of the central nervous system” (Vibert and Hausler 2003); see also Dispenza et al. (Dispenza, De Stefano et al. 2011).
The relevance here is that in a patient with positional vertigo, before entertaining the evasive diagnosis of CV, be sure to evaluate for common diagnoses, such as BPPV.
7. Many patients preliminarily diagnosed with CV are found to have other disorders
Mistaking BPPV for CV is a particularly good illustration of why, when a diagnosis of CV is being considered, one must maintain a broad differential.
Yacovino and Hain comment that, “Many patients preliminarily diagnosed with such a disorder are ultimately found to have other pathologies” (Yacovino and Hain 2013). Brandt states this more forcefully: “Reliable and well-established signs and tests can support a convincing alternative diagnosis in almost all patients presenting with vertigo” (Brandt 1996).
This serves as a reminder that CV remains a diagnosis of exclusion.
8. A Diagnosis of exclusion
Given the difficulty of devising a “proof positive” test for CV, and the repeatedly cited observation that most cases preliminarily diagnosed with CV are ultimately found to have a different cause, most reviews come to the conclusion that CV is a diagnosis of exclusion (Wrisley, Sparto et al. 2000, Kristjansson and Treleaven 2009, Yacovino and Hain 2013, Li and Peng 2015).
Taking the “diagnosis of exclusion” criterion with the definitions, conditions, and assumptions mentioned earlier brings us back to Wrisley’s description that “the diagnosis of cervicogenic dizziness is suggested by (1) a close temporal relationship between neck discomfort and symptoms of dizziness, including time of onset and occurrence of episodes, (2) previous neck injury or pathology, and (3) elimination of other causes of dizziness” (Wrisley, Sparto et al. 2000).
9. What constitutes an adequate workup?
If one takes the position that CV is a diagnosis of exclusion, then the next logical question is, what other diagnoses need to be excluded? Beyond a thorough history and physical examination, there is no consensus on what constitutes an adequate workup to exclude alternative diagnoses.
Practically, since inner ear disturbances are so common, it is reasonable to consider a screening otovestibular workup. At the discretion of the clinician, this could include:
- Ocular vestibular evoked myogenic potentials and videonystagmography.
- If available, rotatory chair testing and computerized dynamic posturography may also be appropriate.
- If the patient’s neck will tolerate it, consider cervical vestibular-evoked myogenic potentials and video head impulse testing.
- If neck rotation provokes symptoms other than vertigo, or reveals physical examination signs of brainstem dysfunction, then imaging is probably warranted. At the discretion of the clinician, this could include:
- Vascular imaging, preferably dynamic, such as CTA, MRA, or dedicated catheter angiography. There is some evidence that transcranial Doppler ultrasound may also have some role (Simon, Niederkorn et al. 1994).
- Imaging of the bony structures (usually by CT) and soft tissue structures (usually by MRI) of the cervical spine.
10. Treatment
The controversy surrounding CV has not prevented clinicians from attempting to treat it, though the optimal therapeutic protocol is uncertain since the underlying mechanism of the disease remains unclear.
10.1. Physical therapy
There has been extensive reporting on physical therapy for the neck as treatment for CV (Karlberg, Magnusson et al. 1996, Borg-Stein, Rauch et al. 2001, Reid and Rivett 2005, Lystad, Bell et al. 2011, Reid, Callister et al. 2014, Yaseen, Hendrick et al. 2018, Alqahtani and Kashoo 2020, Hoppes, Romanello et al. 2020, Yao, Tang et al. 2020), though, “Regarding the treatment of proprioceptive cervical vertigo, in which pain and imbalance or vertigo are the limiting symptoms, the quality of published studies in the current literature is poor” (Yacovino and Hain 2013).
Some authors suggest that a multimodal approach to treatment may be warranted, as evidenced here: “A combined approach is likely to best address the perpetuation of a vicious cycle of events where secondary adaptive changes in the sensorimotor control system could lead to altered cervical muscle function and joint mechanics further altering cervical afferent input… Physical therapy interventions such as pain management, manipulative therapy, active range-of-motion exercises, and exercises to improve neuromuscular control will all be important in reducing possible causes of altered afferent cervical input and subsequent disturbances to sensorimotor control” (Kristjansson and Treleaven 2009). It may also be helpful to incorporate treatment from other disciplines, such as vision therapy.
Although vertigo is one of the cardinal symptoms of CV, “Vestibular physical therapy is not a substitute for physical therapy for the neck” (Hain 2015).
10.2. Why does PT work at all?
If we do not yet know the pathophysiological mechanism underlying CV, then applying physical therapy in this clinical scenario is treating blindly, and seems unlikely to correct the problem by chance; and yet, the physical therapy literature generally describes encouraging outcomes. How can this be?
Whichever factor initiates the process that manifests with one of the symptoms (vertigo or neck pain) may in turn provoke the other, leading to the vicious cycle of a positive feedback loop. Patients who are dizzy from any cause tend to develop neck stiffness (Brandt and Bronstein 2001, Yacovino and Hain 2013), and neck problems causing vertigo defines CV. In other words, these phenomena may exacerbate each other; “interconnections between the cervical proprioceptors and the vestibular nuclei may contribute to a cyclic pattern, such that cervical muscle spasms contribute to dizziness and dizziness contributes to muscle spasm” (Wrisley, Sparto et al. 2000).
Whether the neck symptoms are the cause or the consequence of vertigo, any treatments that reduce neck pain and normalize cervical muscle tone and joint mobility — basically any treatments that normalize cervical mechanics (Johnston, Daye et al. 2017, Williams, Sarig-Bahat et al. 2017) — will interrupt this positive feedback loop, thereby increasing the opportunity for recovery. This idea is reflected in Brandt’s comment that “If CV exists, appropriate management is the same as that for the cervical pain syndrome” (Brandt 1996).
10.3. Medication
Most pharmacologic attempts at management have included muscle relaxants, though there are no good data to suggest that this is effective. On the theory of “migraine-associated cervicogenic vertigo,” a trial of migraine prophylaxis may be reasonable. There has been some exploration of other approaches, such as moxibustion (Li, Yu et al. 2020) and onabotulinum toxin (Odderson 2020).
10.4. Surgery and other invasive procedures
A variety of invasive interventions for CV have been explored, including cervical medial branch blocks (Hahn, Halatsch et al. 2018, Zhu and Grover 2018), percutaneous cervical nucleoplasty (Li, Qi et al. 2020), radiofrequency ablation nucleoplasty (Yin, Zhang et al. 2017), percutaneous laser disc decompression (Ren, Guo et al. 2014), intervertebral disc replacement (Zheng, Muheremu et al. 2020), and surgery for cervical spondylosis or disc herniation (Freppel, Bisdorff et al. 2013). Case series of the various invasive treatments for presumed CV generally report variable outcomes. Given the uncertainty in establishing the diagnosis, and the risks of invasive procedures, we would view invasive procedures as a last-resort approach.
10.5. Alternative therapies
Dry needling (Escaloni, Butts et al. 2018) and acupotomy (Xie, You et al. 2020) have been explored, with limited data.
References
Alqahtani M, Kashoo F (2020) Physical therapy in cervicogenic dizziness. Saudi Journal for Health Sciences 9. doi: 10.4103/sjhs.sjhs_11_20
Araz Server E, Edizer DT, Yigit O, Yasak AG, Erdim C (2018) Relationship between vertebral artery blood flow in different head positions and vertigo. Acta Otolaryngol 138: 1-5. doi: 10.1080/00016489.2017.1373849
Bárány E (1920) Diagnose von Krankheitserscheinungen im Bereiche des Otolithenapparates [Diagnosis of symptoms in the area of the otolith apparatus]. Acta Oto-Laryngologica 2: 434-437. doi: 10.3109/00016482009123103
Barré J-A (1926) Sur un syndrome sympathique cervical postérieur et sa cause frequente, l’arthrite cervicale. Revue Neurologique: 1246-1248.
Bartsch T (2005) Migraine and the neck: new insights from basic data. Curr Pain Headache Rep 9: 191-6. doi: 10.1007/s11916-005-0061-0
Bartsch T, Goadsby PJ (2003) The trigeminocervical complex and migraine: current concepts and synthesis. Curr Pain Headache Rep 7: 371-6. doi: 10.1007/s11916-003-0036-y
Beh SC, Masrour S, Smith SV, Friedman DI (2019) The Spectrum of Vestibular Migraine: Clinical Features, Triggers, and Examination Findings. Headache 59: 727-740. doi: 10.1111/head.13484
Biguer B, Donaldson IM, Hein A, Jeannerod M (1988) Neck muscle vibration modifies the representation of visual motion and direction in man. Brain 111 ( Pt 6): 1405-24. doi: 10.1093/brain/111.6.1405
Blaschek A, Milde-Busch A, Straube A, Schankin C, Langhagen T, Jahn K, Schroder SA, Reiter K, von Kries R, Heinen F (2012) Self-reported muscle pain in adolescents with migraine and tension-type headache. Cephalalgia 32: 241-9. doi: 10.1177/0333102411434808
Blau JN, MacGregor EA (1994) Migraine and the neck. Headache 34: 88-90. doi: 10.1111/j.1526-4610.1994.hed3402088.x
Borg-Stein J, Rauch S, Krabak B (2001) Evaluation and Management of Cervicogenic Dizziness. Critical Reviews in Physical and Rehabilitation Medicine 13: 10. doi: 10.1615/CritRevPhysRehabilMed.v13.i2-3.70
Brandt T (1996) Cervical vertigo–reality or fiction? Audiol Neurootol 1: 187-96. doi: 10.1159/000259201
Brandt T, Bronstein AM (2001) Cervical vertigo. J Neurol Neurosurg Psychiatry 71: 8-12. doi: 10.1136/jnnp.71.1.8
Calhoun AH, Ford S, Millen C, Finkel AG, Truong Y, Nie Y (2010) The prevalence of neck pain in migraine. Headache 50: 1273-7. doi: 10.1111/j.1526-4610.2009.01608.x
Calseyde P, Ampe W, Depondt M (1977) E.N.G. and the cervical syndrome neck torsion nystagmus. Adv Otorhinolaryngol 22: 119-24. doi: 10.1159/000399494
Cherchi M, Bellinaso NP, Card K, Covington A, Krumpe A, Pfeifer MS, Truitt A, Yoo HJ, Rudisill HE, Hain TC (2009) Sound evoked triceps myogenic potentials. Otol Neurotol 30: 545-50. doi: 10.1097/MAO.0b013e31819d89eb
Cherchi M, DiLiberto FE, Yacovino DA, Das S (2021) The Enduring Controversy of Cervicogenic Vertigo, and Its Place among Positional Vertigo Syndromes. Audiology Research 11: 491-507. doi: 10.3390/audiolres11040045
Cherchi M, El-Kholy W, Shirley D, Hain TC (2015) Amplitude of sound evoked triceps myogenic potential scales with force. Journal of Neurology and Neurophysiology 6. doi: 10.4172/2155-9562.1000286
Choi KD, Shin HY, Kim JS, Kim SH, Kwon OK, Koo JW, Park SH, Yoon BW, Roh JK (2005) Rotational vertebral artery syndrome: oculographic analysis of nystagmus. Neurology 65: 1287-1290. doi: PMID: 16247059
Cornelius JF, George B, N’Dri Oka D, Spiriev T, Steiger HJ, Hanggi D (2012) Bow-hunter’s syndrome caused by dynamic vertebral artery stenosis at the cranio-cervical junction–a management algorithm based on a systematic review and a clinical series. Neurosurg Rev 35: 127-35; discussion 135. doi: 10.1007/s10143-011-0343-4
de Jong JM, Bles W, Bovenkerk G (1981) Nystagmus, gaze shift, and self-motion perception during sinusoidal head and neck rotation. Ann N Y Acad Sci 374: 590-9. doi: 10.1111/j.1749-6632.1981.tb30903.x
Dispenza F, De Stefano A, Mathur N, Croce A, Gallina S (2011) Benign paroxysmal positional vertigo following whiplash injury: a myth or a reality? Am J Otolaryngol 32: 376-80. doi: 10.1016/j.amjoto.2010.07.009
Dix MR, Hallpike CS (1952a) The pathology symptomatology and diagnosis of certain common disorders of the vestibular system. Proc R Soc Med 45: 341-54.
Dix MR, Hallpike CS (1952b) The pathology, symptomatology and diagnosis of certain common disorders of the vestibular system. Ann Otol Rhinol Laryngol 61: 987-1016. doi: 10.1177/000348945206100403
Dornhoffer JR, Liu YF, Donaldson L, Rizk HG (2021) Factors implicated in response to treatment/prognosis of vestibular migraine. Eur Arch Otorhinolaryngol 278: 57-66. doi: 10.1007/s00405-020-06061-0
Duan G, Xu J, Shi J, Cao Y (2016) Advances in the Pathogenesis, Diagnosis and Treatment of Bow Hunter’s Syndrome: A Comprehensive Review of the Literature. Interv Neurol 5: 29-38. doi: 10.1159/000444306
Dunlap PM, Khoja SS, Whitney SL, Freburger JK (2019) Assessment of Health Care Utilization for Dizziness in Ambulatory Care Settings in the United States. Otol Neurotol 40: e918-e924. doi: 10.1097/MAO.0000000000002359
Escaloni J, Butts R, Dunning J (2018) The use of dry needling as a diagnostic tool and clinical treatment for cervicogenic dizziness: a narrative review & case series. J Bodyw Mov Ther 22: 947-955. doi: 10.1016/j.jbmt.2018.02.015
Fitz-Ritson D (1991) Assessment of cervicogenic vertigo. J Manipulative Physiol Ther 14: 193-8.
Foster CA, Jabbour P (2007) Barre-Lieou syndrome and the problem of the obsolete eponym. J Laryngol Otol 121: 680-3. doi: 10.1017/S002221510600346X
Freppel S, Bisdorff A, Colnat-Coulbois S, Ceyte H, Cian C, Gauchard G, Auque J, Perrin P (2013) Visuo-proprioceptive interactions in degenerative cervical spine diseases requiring surgery. Neuroscience 255: 226-32. doi: 10.1016/j.neuroscience.2013.09.060
Gdowski GT, McCrea RA (1999) Integration of vestibular and head movement signals in the vestibular nuclei during whole-body rotation. J Neurophysiol 82: 436-49. doi: 10.1152/jn.1999.82.1.436
Gimse R, Tjell C, Bjorgen IA, Saunte C (1996) Disturbed eye movements after whiplash due to injuries to the posture control system. J Clin Exp Neuropsychol 18: 178-86. doi: 10.1080/01688639608408273
Go G, Hwang SH, Park IS, Park H (2013) Rotational Vertebral Artery Compression : Bow Hunter’s Syndrome. J Korean Neurosurg Soc 54: 243-5. doi: 10.3340/jkns.2013.54.3.243
Gray JA, Malcolm JL (1950) The initiation of nerve impulses by mesenteric Pacinian corpuscles. Proc R Soc Lond B Biol Sci 137: 96-114. doi: 10.1098/rspb.1950.0026
Guitton D, Kearney RE, Wereley N, Peterson BW (1986) Visual, vestibular and voluntary contributions to human head stabilization. Exp Brain Res 64: 59-69. doi: 10.1007/BF00238201
Hahn T, Halatsch ME, Wirtz C, Klessinger S (2018) Response to Cervical Medial Branch Blocks In Patients with Cervicogenic Vertigo. Pain Physician 21: 285-294.
Hain TC (2015) Cervicogenic causes of vertigo. Curr Opin Neurol 28: 69-73. doi: 10.1097/WCO.0000000000000161
Hain TC, Cherchi M (2019) Migraine Associated Vertigo. In: Lea J, Pothier D (eds) Advances in Otorhinolaryngology, 2019/04/05 edn, vol 82, pp 119-126
Helton T, Bavry A (2009) Images in Cardiovascular Medicine. Don’t turn your head! Circulation 120: e162. doi: 10.1161/CIRCULATIONAHA.109.896043
Hoppes CW, Romanello AJ, Gaudette KE, Herron WK, McCarthy AE, McHale CJ, Bares J, Turner R, Whitney SL (2020) Physical therapy interventions for cervicogenic dizziness in a military-aged population: protocol for a systematic review. Syst Rev 9: 62. doi: 10.1186/s13643-020-01335-4
Huygen PL, Verhagen WI, Nicolasen MG (1991) Cervico-ocular reflex enhancement in labyrinthine-defective and normal subjects. Exp Brain Res 87: 457-64. doi: 10.1007/BF00231863
Johnston JL, Daye PM, Thomson GT (2017) Inaccurate Saccades and Enhanced Vestibulo-Ocular Reflex Suppression during Combined Eye-Head Movements in Patients with Chronic Neck Pain: Possible Implications for Cervical Vertigo. Front Neurol 8: 23. doi: 10.3389/fneur.2017.00023
Jongkees LB (1969) Cervical vertigo. Laryngoscope 79: 1473-84. doi: 10.1288/00005537-196908000-00011
Kamouchi M, Kishikawa K, Matsuo R, Yasumori K, Inoue T, Okada Y, Ibayashi S (2003) Ultrasonographic detection of extracranial vertebral artery compression in bow hunter’s brain ischemia caused by neck rotation. Cerebrovasc Dis 16: 303-5. doi: 10.1159/000071134
Karlberg M, Johansson R, Magnusson M, Fransson P-A (1996a) Dizziness of suspected cervical origin distinguished by posturographic assessment of human postural dynamics. Journal of vestibular research : equilibrium & orientation 6: 37-47. doi: 10.1016/0957-4271(95)02005-5
Karlberg M, Magnusson M (1996) Asymmetric optokinetic after-nystagmus induced by active or passive sustained head rotations. Acta Otolaryngol 116: 647-51. doi: 10.3109/00016489609137903
Karlberg M, Magnusson M, Malmstrom EM, Melander A, Moritz U (1996b) Postural and symptomatic improvement after physiotherapy in patients with dizziness of suspected cervical origin. Arch Phys Med Rehabil 77: 874-82. doi: 10.1016/s0003-9993(96)90273-7
Kelders WP, Kleinrensink GJ, van der Geest JN, Schipper IB, Feenstra L, De Zeeuw CI, Frens MA (2005) The cervico-ocular reflex is increased in whiplash injury patients. J Neurotrauma 22: 133-7. doi: 10.1089/neu.2005.22.133
Kelman L (2005) Migraine pain location: a tertiary care study of 1283 migraineurs. Headache 45: 1038-47. doi: 10.1111/j.1526-4610.2005.05185.x
Kogler A, Lindfors J, Odkvist LM, Ledin T (2000) Postural stability using different neck positions in normal subjects and patients with neck trauma. Acta Otolaryngol 120: 151-5. doi: 10.1080/000164800750000801
Koskimies K, Sutinen P, Aalto H, Starck J, Toppila E, Hirvonen T, Kaksonen R, Ishizaki H, Alaranta H, Pyykko I (1997) Postural stability, neck proprioception and tension neck. Acta Otolaryngol Suppl 529: 95-7. doi: 10.3109/00016489709124093
Kristjansson E, Treleaven J (2009) Sensorimotor function and dizziness in neck pain: implications for assessment and management. J Orthop Sports Phys Ther 39: 364-77. doi: 10.2519/jospt.2009.2834
L’Heureux-Lebeau B, Godbout A, Berbiche D, Saliba I (2014) Evaluation of paraclinical tests in the diagnosis of cervicogenic dizziness. Otol Neurotol 35: 1858-65. doi: 10.1097/MAO.0000000000000506
Lampl C, Rudolph M, Deligianni CI, Mitsikostas DD (2015) Neck pain in episodic migraine: premonitory symptom or part of the attack? J Headache Pain 16: 566. doi: 10.1186/s10194-015-0566-9
Lee JD, Park MK, Lee BD, Park JY, Lee TK, Sung KB (2011) Otolith function in patients with head trauma. Eur Arch Otorhinolaryngol 268: 1427-30. doi: 10.1007/s00405-010-1426-5
Li C, Qi Y, Liu G, Yin X, Jin Y, Jiang Z, Li P, Kang X, Ye C (2020a) Long-Term Clinical Outcomes of Percutaneous Cervical Nucleoplasty for Cervical Degenerative Diseases with Neck Pain and Cervical Vertigo. World Neurosurg 133: e205-e210. doi: 10.1016/j.wneu.2019.08.210
Li H, Yu T, Cheng P, Qin S, Jiao L, Chen R (2020b) Moxibustion for cervical vertigo: A protocol for a systematic review and meta-analysis. Medicine (Baltimore) 99: e21405. doi: 10.1097/MD.0000000000021405
Li Q, Xie P, Yang WS, Yan B, Davis S, Caplan LR (2019) Vertebral Artery Compression Syndrome. Front Neurol 10: 1075. doi: 10.3389/fneur.2019.01075
Li Y, Peng B (2015) Pathogenesis, Diagnosis, and Treatment of Cervical Vertigo. Pain Physician 18: E583-95.
Lieou Y-C, Barré J-A (1928) Syndrome sympathique cervical postérieur et arthrite chronique de la colonne vertébrale cervicale : (étude clinique et radiologique), Université de Strasbourg
Lu DC, Zador Z, Mummaneni PV, Lawton MT (2010) Rotational vertebral artery occlusion-series of 9 cases. Neurosurgery 67: 1066-72; discussion 1072. doi: 10.1227/NEU.0b013e3181ee36db
Lystad RP, Bell G, Bonnevie-Svendsen M, Carter CV (2011) Manual therapy with and without vestibular rehabilitation for cervicogenic dizziness: a systematic review. Chiropr Man Therap 19: 21. doi: 10.1186/2045-709X-19-21
Mallinson AI, Longridge NS (1998) Dizziness from whiplash and head injury: differences between whiplash and head injury. Am J Otol 19: 814-8.
Matthews PB (1966) The reflex excitation of the soleus muscle of the decerebrate cat caused by vibbration applied to its tendon. J Physiol 184: 450-72. doi: 10.1113/jphysiol.1966.sp007926
Mergner T, Huber W, Becker W (1997) Vestibular-neck interaction and transformation of sensory coordinates. J Vestib Res 7: 347-67.
Mergner T, Siebold C, Schweigart G, Becker W (1991) Human perception of horizontal trunk and head rotation in space during vestibular and neck stimulation. Exp Brain Res 85: 389-404. doi: 10.1007/BF00229416
Micarelli A, Viziano A, Augimeri I, Micarelli B, Capoccia D, Alessandrini M (2021) Diagnostic route of cervicogenic dizziness: usefulness of posturography, objective and subjective testing implementation and their correlation. Disabil Rehabil 43: 1730-1737. doi: 10.1080/09638288.2019.1680747
Mitchell J (2007) Doppler insonation of vertebral artery blood flow changes associated with cervical spine rotation: Implications for manual therapists. Physiother Theory Pract 23: 303-13. doi: 10.1080/09593980701593771
Mitchell J (2009) Vertebral Artery Blood flow Velocity Changes Associated with Cervical Spine rotation: A Meta-Analysis of the Evidence with implications for Professional Practice. J Man Manip Ther 17: 46-57. doi: 10.1179/106698109790818160
Neuhauser H, Leopold M, von Brevern M, Arnold G, Lempert T (2001) The interrelations of migraine, vertigo, and migrainous vertigo. Neurology 56: 436-41.
Norre ME (1987) Cervical vertigo. Diagnostic and semiological problem with special emphasis upon “cervical nystagmus”. Acta Otorhinolaryngol Belg 41: 436-52.
Norre ME, Forrez G, Stevens A, Beckers A (1987) Cervical vertigo diagnosed by posturography? Preliminary report. Acta Otorhinolaryngol Belg 41: 574-81.
Odderson IR (2020) A new treatment for cervical vertigo with botulinum toxin. J Clin Neurosci 73: 316-317. doi: 10.1016/j.jocn.2020.01.016
Ogawa Y, Itani S, Otsuka K, Inagaki T, Shimizu S, Kondo T, Nishiyama N, Nagai N, Suzuki M (2014) Intermittent positional downbeat nystagmus of cervical origin. Auris Nasus Larynx 41: 234-7. doi: 10.1016/j.anl.2013.07.012
Oosterveld WJ, Kortschot HW, Kingma GG, de Jong HA, Saatci MR (1991) Electronystagmographic findings following cervical whiplash injuries. Acta Otolaryngol 111: 201-5. doi: 10.3109/00016489109137375
Ozer G, Benlier N (2020) Neck pain: is it part of a migraine attack or a trigger before a migraine attack? Acta Neurol Belg 120: 289-293. doi: 10.1007/s13760-018-1030-9
Padoan S, Karlberg M, Fransson PA, Magnusson M (1998) Passive sustained turning of the head induces asymmetric gain of the vestibulo-ocular reflex in healthy subjects. Acta Otolaryngol 118: 778-82. doi: 10.1080/00016489850182431
Pearce JM (1989) Whiplash injury: a reappraisal. J Neurol Neurosurg Psychiatry 52: 1329-31. doi: 10.1136/jnnp.52.12.1329
Peng B (2018) Cervical Vertigo: Historical Reviews and Advances. World Neurosurg 109: 347-350. doi: 10.1016/j.wneu.2017.10.063
Philipszoon AJ, Bos JH (1963) Neck Torsion Nystagmus. Pract Otorhinolaryngol (Basel) 25: 339-44. doi: 10.1159/000274540
Piovesan EJ, Kowacs PA, Oshinsky ML (2003) Convergence of cervical and trigeminal sensory afferents. Curr Pain Headache Rep 7: 377-83. doi: 10.1007/s11916-003-0037-x
Pradhan S, Choudhury SS (2018) Clinical characterization of neck pain in migraine. Neurol India 66: 377-384. doi: 10.4103/0028-3886.227302
Reid SA, Callister R, Katekar MG, Rivett DA (2014) Effects of cervical spine manual therapy on range of motion, head repositioning, and balance in participants with cervicogenic dizziness: a randomized controlled trial. Arch Phys Med Rehabil 95: 1603-12. doi: 10.1016/j.apmr.2014.04.009
Reid SA, Rivett DA (2005) Manual therapy treatment of cervicogenic dizziness: a systematic review. Man Ther 10: 4-13. doi: 10.1016/j.math.2004.03.006
Ren L, Guo B, Zhang J, Han Z, Zhang T, Bai Q, Zeng Y (2014) Mid-term efficacy of percutaneous laser disc decompression for treatment of cervical vertigo. Eur J Orthop Surg Traumatol 24 Suppl 1: S153-8. doi: 10.1007/s00590-013-1264-4
Rousseaux M, Salomez JL, Petit H (1983) [Syncopes and transitory neurologic manifestations revealing cervico-occipital joint malformations. Evidence of a vascular mechanism]. Sem Hop 59: 729-32.
Rubin AM, Woolley SM, Dailey VM, Goebel JA (1995) Postural stability following mild head or whiplash injuries. Am J Otol 16: 216-21.
Ryan GM, Cope S (1955) Cervical vertigo. Lancet 269: 1355-8. doi: 10.1016/s0140-6736(55)93159-7
Rydevik B, Szpalski M, Aebi M, Gunzburg R (2008) Whiplash injuries and associated disorders: new insights into an old problem. European spine journal. 17: 359-416. doi: 10.1007/s00586-007-0484-x
info:doi/10.1007/s00586-007-0484-x
Saber Tehrani AS, Coughlan D, Hsieh YH, Mantokoudis G, Korley FK, Kerber KA, Frick KD, Newman-Toker DE (2013) Rising annual costs of dizziness presentations to U.S. emergency departments. Acad Emerg Med 20: 689-96. doi: 10.1111/acem.12168
Sakaguchi M, Kitagawa K, Hougaku H, Hashimoto H, Nagai Y, Yamagami H, Ohtsuki T, Oku N, Hashikawa K, Matsushita K, Matsumoto M, Hori M (2003) Mechanical compression of the extracranial vertebral artery during neck rotation. Neurology 61: 845-7. doi: 10.1212/01.wnl.0000078081.12097.ae
Sarkar J, Wolfe SQ, Ching BH, Kellicut DC (2014) Bow hunter’s syndrome causing vertebrobasilar insufficiency in a young man with neck muscle hypertrophy. Ann Vasc Surg 28: 1032 e1-1032 e10. doi: 10.1016/j.avsg.2013.06.038
Schoon Y, Olde Rikkert MG, Rongen S, Lagro J, Schalk B, Claassen JA (2013) Head turning-induced hypotension in elderly people. PLoS One 8: e72837. doi: 10.1371/journal.pone.0072837
Schoonman GG, Evers DJ, Terwindt GM, van Dijk JG, Ferrari MD (2006) The prevalence of premonitory symptoms in migraine: a questionnaire study in 461 patients. Cephalalgia 26: 1209-13. doi: 10.1111/j.1468-2982.2006.01195.x
Shirley D, Cherchi M, Hain TC (2015) Triceps acoustically evoked myogenic potentials in patients with spinal cord lesions. Journal of Neurology and Neurophysiology 6. doi: 10.4172/2155-9562.1000288
Simon H, Niederkorn K, Horner S, Duft M, Schrockenfuchs M (1994) [Effect of head rotation on the vertebrobasilar system. A transcranial Doppler ultrasound contribution to the physiology]. HNO 42: 614-8.
Sorensen BF (1978) Bow hunter’s stroke. Neurosurgery 2: 259-61.
Symons BP, Leonard T, Herzog W (2002) Internal forces sustained by the vertebral artery during spinal manipulative therapy. J Manipulative Physiol Ther 25: 504-10. doi: 10.1067/mmt.2002.127076
Takemori S, Suzuki JI (1971) Eye deviations from neck torsion in humans. Ann Otol Rhinol Laryngol 80: 439-44. doi: 10.1177/000348947108000323
Thompson-Harvey A, Hain TC (2019) Symptoms in cervical vertigo. Laryngoscope Investig Otolaryngol 4: 109-115. doi: 10.1002/lio2.227
Tjell C, Rosenhall U (1998) Smooth pursuit neck torsion test: a specific test for cervical dizziness. Am J Otol 19: 76-81.
Toglia JU (1976) Acute flexion-extension injury of the neck. Electronystagmographic study of 309 patients. Neurology 26: 808-14. doi: 10.1212/wnl.26.9.808
Treleaven J, Joloud V, Nevo Y, Radcliffe C, Ryder M (2020) Normative Responses to Clinical Tests for Cervicogenic Dizziness: Clinical Cervical Torsion Test and Head-Neck Differentiation Test. Phys Ther 100: 192-200. doi: 10.1093/ptj/pzz143
Treleaven J, Jull G, LowChoy N (2006) The relationship of cervical joint position error to balance and eye movement disturbances in persistent whiplash. Man Ther 11: 99-106. doi: 10.1016/j.math.2005.04.003
van Leeuwen RB, van der Zaag-Loonen H (2017) Dizziness and neck pain: a correct diagnosis is required before consulting a physiotherapist. Acta Neurol Belg 117: 241-244. doi: 10.1007/s13760-016-0694-2
Vibert D, Hausler R (2003) Acute peripheral vestibular deficits after whiplash injuries. Ann Otol Rhinol Laryngol 112: 246-51. doi: 10.1177/000348940311200310
Vibert D, Rohr-Le Floch J, Gauthier G (1993) Vertigo as manifestation of vertebral artery dissection after chiropractic neck manipulations. ORL J Otorhinolaryngol Relat Spec 55: 140-2. doi: 10.1159/000276405
von Brevern M, Radtke A, Lezius F, Feldmann M, Ziese T, Lempert T, Neuhauser H (2007) Epidemiology of benign paroxysmal positional vertigo: a population based study. J Neurol Neurosurg Psychiatry 78: 710-5. doi: 10.1136/jnnp.2006.100420
Walton DM, Elliott JM (2017) An Integrated Model of Chronic Whiplash-Associated Disorder. J Orthop Sports Phys Ther 47: 462-471. doi: 10.2519/jospt.2017.7455
Wapner S, Werner H, Chandler KA (1951) Experiments on sensory-tonic field theory of perception. I. Effect of extraneous stimulation on the visual perception of verticality. J Exp Psychol 42: 341-4. doi: 10.1037/h0053846
Weintraub MI, Khoury A (2004) Mechanical compression of the extracranial vertebral artery during neck rotation. Neurology 62: 2143; author reply 2144. doi: 10.1212/wnl.62.11.2143-a
Williams G, Sarig-Bahat H, Williams K, Tyrrell R, Treleaven J (2017a) Cervical kinematics in patients with vestibular pathology vs. patients with neck pain: A pilot study. J Vestib Res 27: 137-145. doi: 10.3233/VES-170615
Williams K, Tarmizi A, Treleaven J (2017b) Use of neck torsion as a specific test of neck related postural instability. Musculoskeletal Science and Practice 29: 115-119. doi: https://doi.org/10.1016/j.msksp.2017.03.012
Wober C, Brannath W, Schmidt K, Kapitan M, Rudel E, Wessely P, Wober-Bingol C, Group PS (2007) Prospective analysis of factors related to migraine attacks: the PAMINA study. Cephalalgia 27: 304-14. doi: 10.1111/j.1468-2982.2007.01279.x
Wrisley DM, Sparto PJ, Whitney SL, Furman JM (2000) Cervicogenic dizziness: a review of diagnosis and treatment. J Orthop Sports Phys Ther 30: 755-66. doi: 10.2519/jospt.2000.30.12.755
Xie R, You J, Liu L, Huang C, Liang Y (2020) Acupotomy therapy for cervical vertigo: A protocol for a systematic review and meta-analysis. Medicine (Baltimore) 99: e20662. doi: 10.1097/MD.0000000000020662
Yacovino DA, Hain TC (2013) Clinical characteristics of cervicogenic-related dizziness and vertigo. Semin Neurol 33: 244-55. doi: 10.1055/s-0033-1354592
Yao M, Tang ZY, Cui XJ, Sun YL, Ye XL, Wang P, Zhong WH, Zhang RC, Li HY, Hu ZJ, Wang WM, Qiao WP, Li J, Gao Y, Shi Q, Wang YJ (2020) Shi-Style Cervical Mobilizations Versus Massage for Cervical Vertigo: A Multicenter, Randomized, Controlled Clinical Trial. J Altern Complement Med 26: 58-66. doi: 10.1089/acm.2019.0113
Yaseen K, Hendrick P, Ismail A, Felemban M, Alshehri MA (2018) The effectiveness of manual therapy in treating cervicogenic dizziness: a systematic review. J Phys Ther Sci 30: 96-102. doi: 10.1589/jpts.30.96
Yin HD, Zhang XM, Huang MG, Chen W, Song Y, Du QJ, Wu YN, Yang RB (2017) Curative effect and mechanism of radiofrequency ablation nucleoplasty in the treatment of cervical vertigo. Br J Radiol 90: 20150772. doi: 10.1259/bjr.20150772
Zaidi HA, Albuquerque FC, Chowdhry SA, Zabramski JM, Ducruet AF, Spetzler RF (2014) Diagnosis and management of bow hunter’s syndrome: 15-year experience at barrow neurological institute. World Neurosurg 82: 733-8. doi: 10.1016/j.wneu.2014.02.027
Zajacova A, Grol-Prokopczyk H, Zimmer Z (2021) Pain Trends Among American Adults, 2002-2018: Patterns, Disparities, and Correlates. Demography 58: 711-738. doi: 10.1215/00703370-8977691
Zheng S, Muheremu A, Sun Y, Tian W, Wu CA (2020) Preoperative imaging differences of patients with cervical spondylosis with cervical vertigo indicate the prognosis after cervical total disc replacement. J Int Med Res 48: 300060519877033. doi: 10.1177/0300060519877033
Zhu X, Grover MJ (2018) Cervicogenic Dizziness Successfully Treated With Upper Cervical Medial Branch Nerve Radiofrequency Ablation: A Case Report. A A Pract 10: 150-153. doi: 10.1213/XAA.0000000000000717
![]()