By Marcello Cherchi, MD PhD
For patients
Visual snow syndrome (VSS) is a visual disorder in which patients perceive the world as if distorted by television static. This usually begins spontaneously in one’s 20s, and is often accompanied by other visual and non-visual symptoms. Some of the symptoms may resemble the visual aura of migraine. The symptoms may start as intermittent, but eventually become chronic, and can persist for years. Your doctor may consider checking various tests and brain imaging; these should be normal in VSS, and this helps exclude other diagnoses. You should also be examined by a general ophthalmologist or neuro-ophthalmologist to make sure that the eyes themselves are normal. Treatment with medication is usually unsuccessful, and medications have risks. Non-risk interventions include vestibular rehabilitation therapy and visual filters.
For clinicians
Practical summary
Visual snow (VS) refers to the experience of perceiving the entire visual scene as distorted by television static. In most patients VS occurs in the context of several other visual and non-visual symptoms, the constellation of which is referred to as visual snow syndrome (VSS). This is uncommon but probably under-recognized. In most patients VSS begins spontaneously (primary VSS), while in others it appears to occur following some other insult or event (secondary VSS), such as head trauma, use of medication of recreational drugs. There is some clinical overlap with migrainous visual aura, and there is debate in the literature about whether VSS lies on a continuum with migraine, or represents a discrete clinical entity. The underlying pathophysiology is unknown, and investigational studies report imaging or electrophysiologic abnormalities at multiple levels in the visual system. The peak age of onset is the 3rd decade, with a slight (53%) female preponderance. Symptoms may begin as intermittent, but in most patients eventually become continuous. Physical examination, bedside ocular motor examination and standard brain MRI are normal. Patients should be examined by a general ophthalmologist or neuro-ophthalmologist to exclude primary ophthalmic disease. Treatment has been attempted with a broad variety of medications, with largely unsatisfactory results. There is emerging evidence of benefit from vestibular rehabilitation therapy or treatment with visual filters, and these interventions incur no medical risk. Prognosis is guarded; symptoms can last for years.
Introduction
Although patients with visual snow syndrome (VSS) do not usually describe any symptoms of disequilibrium, they are nevertheless sometimes referred to otoneurology. Outside of ophthalmology and neuro-optometry, VSS is not known by most medical practitioners, and absent any vestibular symptoms, the rationale for referral to otoneurology is unclear.
In 1995 Liu and colleagues (Liu, Schatz et al. 1995) reported on ten migraine patients with “persistent positive visual phenomena lasting months to years.” As additional cases were reported in the literature this phenomenon eventually became known as visual snow (VS).
Visual snow is currently taken to the experience of a “continuous visual disturbance resembling a badly tuned analogue television” (Graber, Scutelnic et al. 2022), “seeing numerous tiny snow-like dots throughout the visual field” (Bou Ghannam and Pelak 2017), “innumerable flickering dots throughout the visual field, similar to ‘TV static’” (Metzler and Robertson 2018).
Although VS can occur in isolation, it more commonly occurs in conjunction with several other visual and sometimes non-visual symptoms, in which case the constellation of symptoms is referred to as visual snow syndrome (VSS).
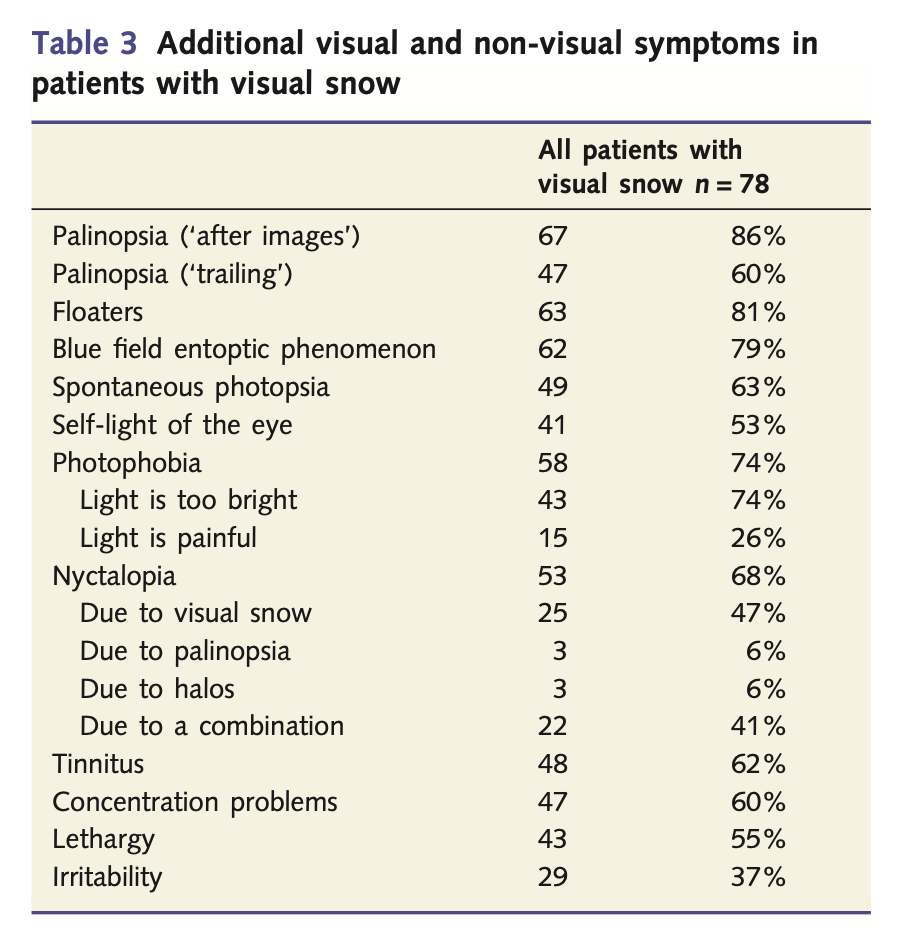
Schankin and colleagues (Schankin, Maniyar et al. 2014) studied 78 patients with VSS and reported the additional symptoms listed in the following Table.
Some investigators draw a distinction between primary and secondary VSS (Metzler and Robertson 2018, Mehta, Garza et al. 2021). Primary VSS occurs spontaneously, whereas secondary VSS appears to occur following some insult or event, such as concussion (Ciuffreda, Han et al. 2021, Mehta, Garza et al. 2021, Werner and Gustafson 2022), medication (Naguy, Naguy et al. 2022), infection or use of hallucinogenic and other recreational drugs including cannabis, ecstasy, cocaine or amphetamines (Schankin, Maniyar et al. 2014, Mehta, Garza et al. 2021).
There are no universally accepted criteria for diagnosing VSS, but Metzler and Robinson (Metzler and Robertson 2018), building on work by Schankin and colleagues (Schankin, Maniyar et al. 2014), proposed the criteria in the Table below.

Some investigators maintain that visual snow is distinct from migrainous visual aura (Schankin, Maniyar et al. 2014), but not all investigators agree that visual snow syndrome comprises a discrete clinical entity (Sampatakakis, Lymperopoulos et al. 2022).
Epidemiology
Visual snow syndrome is uncommon. In 2018 Metzler and Robertson (Metzler and Robertson 2018) stated that only 200 reports had been published. Referral patterns since then suggest that the diagnosis is being increasingly recognized, or at least increasingly suspected.
Schankin and colleagues (Schankin, Maniyar et al. 2014) studied 78 patients with VSS and reported the demographics listed in the following Table.

Notable features include the age of onset was 21 ± 9 years, symptom duration was 8 ± 10 years, and there was a slight female preponderance at 41/78 (53%) of patients.
Genetics
As of this writing, VSS has not been described as occurring in familial patterns, nor has any genetic pattern been published.
Pathophysiological mechanism of disease
The underlying pathobiology of VSS is unknown. Data from imaging and electrophysiology studies suggest several possibilities at multiple levels of the visual system.
Some studies suggest dysfunction as early in the visual pathway as the retina:
- Alissa and colleagues (Alissa, W et al. 2012) studied 7 patients with visual snow (VS) and 9 healthy controls by exposing subjects to various colored stimuli and measuring pupillary responses. They observed that, “The pupil responses in three of the VS patients lacked the rapid recovery phase following the initial constriction to stimulus onset,” and concluded that, “The absence of recovery following the initial constriction of the pupil in three of the VS patients deviates from normal responses and suggests the presence of a more sustained retinal afferent signal that drives the pupil response.” In other words, they are suggesting that at least part of the pathophysiology localizes to the retina.
Some studies identify dysfunction in primary visual cortex:
- McKendrick and colleagues (McKendrick, Chan et al. 2017) compared 16 visual snow patients with 18 healthy controls on a series of visual perceptual tasks. They reported that, “Our study demonstrates that visual perceptual measures involving the suprathreshold processing of contrast and luminance are abnormal in a group of individuals with visual snow,” and concluded that, “Our data are consistent with elevated excitability in primary visual cortex; however, further research is required to provide more direct evidence for this proposed mechanism.”
- White and colleagues (White, Clough et al. 2018) performed a literature review on visual snow syndrome and concluded that, “VSS is likely associated with either hyperactive visual cortices or, alternatively, impaired processing of simultaneous afferent information projecting to cortex.”
- Yildiz and colleagues (Yildiz, Turkyilmaz et al. 2019) compared repetitive pattern reversal visual evoked potentials from transcranial magnetic stimulation-induced phosphene in 17 VS patients (10 with migraine, 7 without migraine) and 12 healthy controls. They reported that, “The loss of habituation and lower threshold for occipital cortex excitability were demonstrated electrophysiologically in VS patients.”
Some studies suggest that the dysfunction lies in secondary visual cortex involved in higher-level visual processing:
- Schankin and Goadsby (Schankin and Goadsby 2015) review fMRI data in patients with visual snow (VS) and note “hypermetabolism in the supplementary visual cortex,” adding that, “the primary visual cortex (cuneus) did not show hypermetabolism in VS patients arguing for VS being a disorder of visual post-processing outside of the retino-geniculo-cortical pathway.”
- Eren and colleagues (Eren, Rauschel et al. 2018) compared visual evoked potentials in 18 visual snow patients with age-matched migraineurs and healthy controls. They reported that, “Visual evoked potentials from patients with VS demonstrated increased N145 latency and reduced N75-P100 amplitudes,” and concluded that, “These findings are in agreement with the idea that the primary disturbance in VS is a dysfunction of the visual association cortex.”
- Aldusary and colleagues (Aldusary, Traber et al. 2020) compared fMRI in 19 visual snow patients and 16 age- and sex-matched healthy control subjects. They reported that, “Patients with VS showed hyperconnectivity between extrastriate visual and inferior temporal brain regions and also between prefrontal and parietal (angular cortex) regions,” and interpreted this as showing “VS to be associated with both functional and structural changes in the early and higher visual cortex, as well as the temporal cortex.”
Some studies characterize VSS as a dysfunction at a broader “network” level:
- Klein and Schankin (Klein and Schankin 2021) performed a literature review of 53 studies on VSS and concluded that, “The studies that have been included in this review demonstrate structural, functional, and metabolic alterations in the primary and/or secondary visual areas of the brain. Beyond that, results indicate a disruption in the pre-cortical visual pathways and large-scale networks including the default mode network and the salience network.”
- Fraser (Fraser 2022) reviewed literature suggesting that VSS, “is due to a widespread cortical dysfunction. Cortical hyperexcitability coupled with changes in thalamocortical pathways and higher-level salience network controls have all shown differences in patients with visual snow syndrome compared to controls.”
- Strik and colleagues (Strik, Clough et al. 2023) compared resting-state MRI in 40 VSS patients and 60 healthy controls. They reported that, “This study revealed reduced dynamic variation in modularity and local efficiency strength in the VSS brain, suggesting that brain network dynamics are less variable in terms of segregation and local clustering.”
Some investigators suggest that VSS is one presentation along a continuum of disease that may include migraine (Puledda, Schankin et al. 2020) or other “perceptual disorders” such as persistent postural perceptual dizziness, fibromyalgia and chronic tinnitus (Klein and Schankin 2021).
Clinical presentation
Symptoms of visual snow syndrome (VSS) include not just visual snow itself, but also other visual symptoms, and often non-visual symptoms as well.
Schankin and colleagues (Schankin, Maniyar et al. 2014) studied 78 patients with VSS and reported that, besides the symptom of visual snow itself, other visual and non-visual symptoms included:
- Visual symptoms:
- Palinopsia. This refers to the perception that, after an object moves, it leaves after-images (in 86% of patients), visual trailing (in 60%) or visual ghosting.
- Excessive floaters (81%).
- “Blue field entopic phenomenon” (79%) which refers to “little bright dots traveling on a wiggly path when looking at a blue background.”
- Photophobia, manifesting as light being perceived as too bright (74%) or painful (26%).
- Spontaneous photopsia (63%) (flashes of light).
- “Self-light of the eye” (53%) which refers to, “clouds, swirls, or waves with eyes closed.”
- Nyctalopia (68%) (impaired night vision).
- Cognitive symptoms:
- Concentration problems (60%).
- Lethargy (55%).
- Irritability (37%).
- Tinnitus (62%).
Lauschke and colleagues (Lauschke, Plant et al. 2016) studied a cohort of 32 patients with VS and reported that 22% complained of tremor.
Solly and colleagues (Solly, Clough et al. 2021) add that VSS patients endorse considerable psychiatric comorbidity.
We find it noteworthy that, besides perhaps nyctalopia, all of the visual abnormalities are positive phenomena. Notably absent are negative visual phenomena (such as scotomata) or visual distortions (tunnel vision, macropsia) that occur in migraine with visual aura.
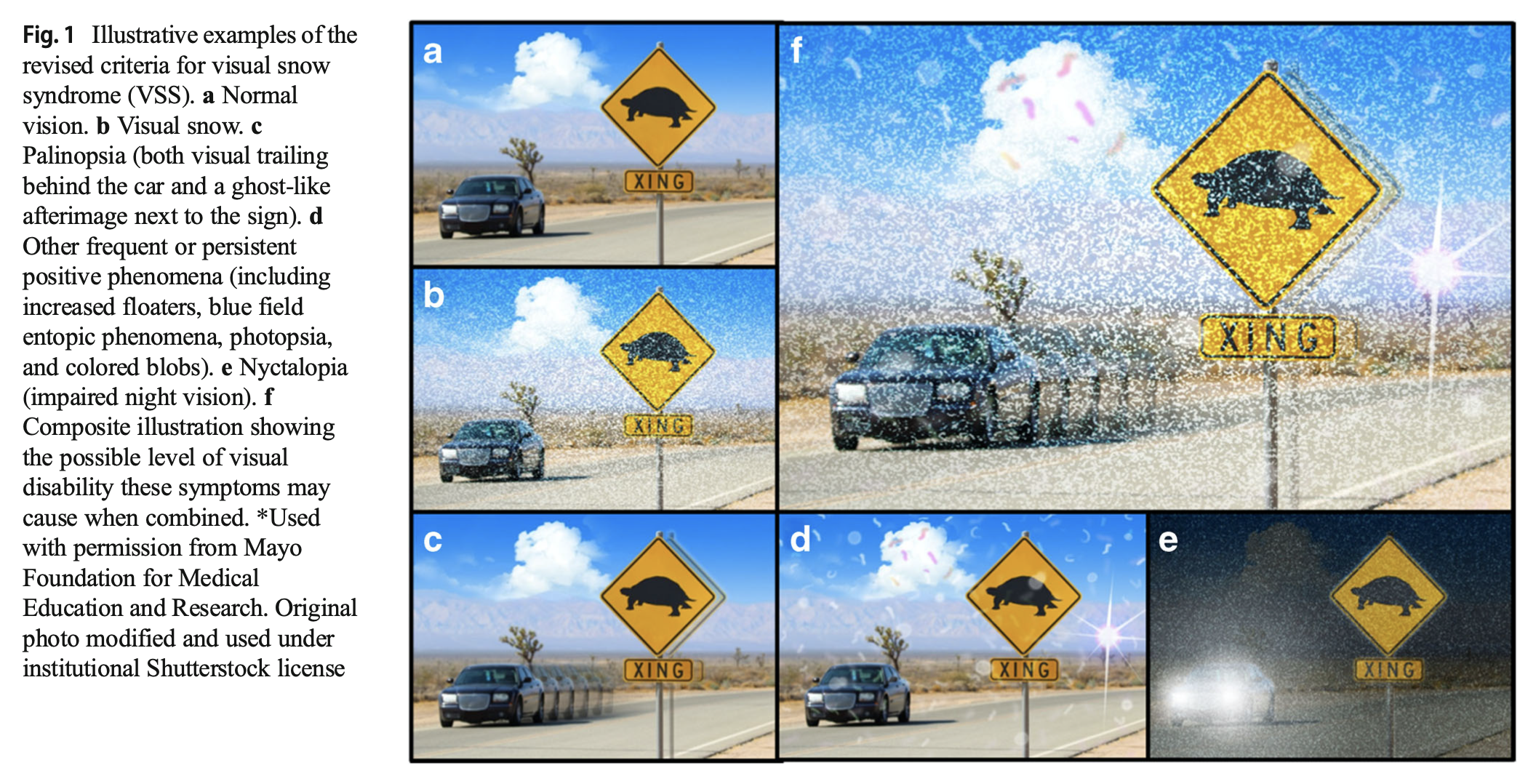
The Figure below, from Metzler and Robertson (Metzler and Robertson 2018), illustrates some of the visual phenomena experienced in visual snow syndrome.
With respect to chronology, Schankin and colleagues (Schankin, Maniyar et al. 2014) studied 78 patients with VSS and reported that:
- Of 78 patients, 19 (24%) described symptoms since childhood (“as long as the patient can recall”), and 59 (76%) at some point thereafter (“patient recalls period of life without visual snow”).
- Of 78 patients, 32 (41%) described symptoms as being continuous since onset, 33 (42%) as gradually progressive worsening, 10 (13%) as stepwise worsening, and 3 (4%) as both progressive and stepwise worsening.
Physical examination
In patients with VSS who are otherwise healthy, physical examination should be normal (Eren and Schankin 2020).
Ocular motor examination
As of this writing there were no published studies of bedside ocular motor findings in VSS.
Testing: vestibular
As of this writing there were no published studies of standard otovestibular test results in patients with VSS.
However, several studies describe various abnormalities on specific saccade tasks in VSS patients compared to controls.
- Solly and colleagues (Solly, Clough et al. 2020) compared 64 VSS patients (32 with migraine and 32 without migraine) and 23 healthy controls on several saccade tasks: prosaccades (PS), antisaccades (AS) and interleaved AS-PS tasks. They observed that, “compared to controls, the VSS group generated significantly shortened PS latencies (p = 0.029) and an increased rate of AS errors (p = 0.001), irrespective of the demands placed on visual processing (i.e., task context),” and concluded that, “The absence of any additional switch cost on the AS-PS task in VSS suggests that the PS latency and AS error differences are attributable to a speeded PS response rather than to impaired executive processes more commonly implicated in poorer AS performance.”
- Foletta and colleagues (Foletta, Clough et al. 2021) compared 40 VSS patients (20 with migraine, 20 without migraine) and 20 healthy controls on the “inhibition of return (IOR) phenomenon that “ describes the relative slowing of a response to a validly cued location compared to invalidly cued location with longer cue/target intervals.” They concluded that, “Our results are consistent with the proposal that in VSS, a shift of attention elicits a stronger increase in saccade-related activity than healthy controls.”
These tests are interesting, though not (yet) broadly applied in clinical practice because of the specialized equipment needed. Both of the cited studies used EyeLink® 1000 video oculography hardware that has a frame rate acquisition of 1,000 Hz (which is not available on most commercial videonystagmography software).
Imaging
Several MRI studies report morphological abnormalities in VSS patients.
- Aldusary and colleagues (Aldusary, Traber et al. 2020) compared fMRI in 19 visual snow patients and 16 age- and sex-matched healthy control subjects. They reported that VSS patients, “showed increased GMV [gray matter volume] in the right lingual gyrus.”
- Puledda and colleagues (Puledda, Bruchhage et al. 2020) compared MRI-based voxel morphometry in 24 VSS patients and 24 age- and sex-matched healthy controls. They reported that, “Compared to healthy controls, patients with visual snow syndrome had increased gray matter volume in the left primary and secondary visual cortices, the left visual motion area V5, and the left cerebellar crus I/lobule VI area.”
- Strik and colleagues (Strik, Clough et al. 2022) used a 7-Tesla MRI to compare 40 VSS patients with 43 healthy controls. They reported that, “widespread changes in grey matter microstructure, which followed a caudal-rostral pattern and affected the occipital cortices most profoundly.”
The studies cited above lie in the domain of research. In clinical practice, regular MRI is unlikely to reveal findings that confirm a diagnosis of VSS; the main value of MRI is to exclude competing diagnoses.
Histopathology
As of this writing there were no published autopsy reports of patients with VSS.
Differential diagnosis
Each individual component of VSS can occur in other diseases as well. Since the majority of the symptoms in VSS involve visual perception, it is important for patients to have a general ophthalmological, or neuro-ophthalmological evaluation, in order to exclude primary ophthalmological disease; patients with VSS who are otherwise healthy should have normal ophthalmological examinations (Yoo, Yang et al. 2020).
Patel and colleagues (Patel, Vitale et al. 2021) report a case of a patient diagnosed with VSS who in fact had birdshot chorioretinopathy.
Treatment: Visual rehabilitation
There is emerging evidence that vestibular rehabilitation therapy (VRT) may play a role in the management of VSS (Tsang, Shidlofsky et al. 2022). We favor a trial of VRT as it incurs no medical risk.
Treatment: Visual filters
Lauschke and colleagues (Lauschke, Plant et al. 2016) studied a cohort of 32 patients with visual snow (VS) and reported that, “ninety-two percent of patients felt that symptoms improved during the testing with a particular coloured filter,” “particularly in the yellow-blue color spectrum.” This finding still has to be replicated, but we support a trial of this intervention given that it incurs no medical risk. Eren and Schankin (Eren and Schankin 2020) note that this visual intervention can be applied for everyday use.
Treatment: Medication
Bou Ghannam and Pelak (Bou Ghannam and Pelak 2017) reviewed treatment trials medications used for treatment “persistent visual phenomena and/or visual snow.” The results are summarized by results and class of evidence in the Table below.
|
Effective |
Ineffective |
Mixed results |
|
|
Class I evidence |
— |
|
— |
|
Class II evidence |
|
|
— |
|
Class III evidence |
|
|
— |
|
Class IV evidence |
|
|
|
In short, there was only one Class I study, which concluded that sumatriptan was ineffective. There was one Class II study which concluded that ketamine was effective. There were two Class II studies that nimodipine and metoprolol were ineffective. The remaining studies (showing efficacy, inefficacy or mixed results) were all Class III or Class IV.
Despite these weak data, Bou Ghannam and colleagues (Bou Ghannam and Pelak 2017) recommended the following treatments:
- Lamotrigine, starting at 25 mg per day, tapering up to 200 – 300 mg per day in divided doses.
- Acetazolamide, starting at 250 mg per day, tapering up to 1000 mg per day in divided doses.
- Verapamil ER, starting at 120 mg per day, tapering up ton 240 mg per day.
Eren and Schankin (Eren and Schankin 2020) reviewed studies of other medications as well, including fluoxetine, esketamine, magnesium, amitriptyline, sertraline, baclofen, gabapentin, carbamazepine, coenzyme Q10, methylphenidate, flubiprofen, duloxetine, paroxetine, pizotifen and dothiepin. They concluded that, “Currently, there is no treatment available that would effectively improve VSS,” but added that, “The best data is available for lamotrigine. It has been used in 36 patients, was effective in 22.2% including one total response, and did not result in worsening. The second most often used medication was topiramate. It is both, an anti-epileptic drug and usually highly effective for migraine. Only two out of 13 patients with VSS (15.4%) had some effect, and one had worsening.”
Puledda and colleagues (Puledda, Vandenbussche et al. 2022) concluded that, “medications are generally ineffective in VSS.”
Prognosis
With or without treatment, symptoms of VSS can last years (Graber, Scutelnic et al. 2022).
References
Aldusary N, Traber GL, Freund P, Fierz FC, Weber KP, Baeshen A, Alghamdi J, Saliju B, Pazahr S, Mazloum R, Alshehri F, Landau K, Kollias S, Piccirelli M, Michels L (2020) Abnormal Connectivity and Brain Structure in Patients With Visual Snow. Frontiers in Human Neuroscience 14: 476.
Alissa R, W B, Bessero A, Plant G, JL B (2012) Vision in subjects with hyperawareness of afterimages and “visual snow”. 90: 0-0. doi: doi:10.1111/j.1755-3768.2012.F066.x
Bou Ghannam A, Pelak VS (2017) Visual Snow: a Potential Cortical Hyperexcitability Syndrome. Curr Treat Options Neurol 19: 9. doi: 10.1007/s11940-017-0448-3
Ciuffreda KJ, Han ME, Tannen B, Rutner D (2021) Visual snow syndrome: evolving neuro-optometric considerations in concussion/mild traumatic brain injury. Concussion 6: CNC89. doi: 10.2217/cnc-2021-0003
Eren O, Rauschel V, Ruscheweyh R, Straube A, Schankin CJ (2018) Evidence of dysfunction in the visual association cortex in visual snow syndrome. Ann Neurol 84: 946-949. doi: 10.1002/ana.25372
Eren O, Schankin CJ (2020) Insights into pathophysiology and treatment of visual snow syndrome: A systematic review. Prog Brain Res 255: 311-326. doi: 10.1016/bs.pbr.2020.05.020
Foletta PJ, Clough M, McKendrick AM, Solly EJ, White OB, Fielding J (2021) Delayed Onset of Inhibition of Return in Visual Snow Syndrome. Front Neurol 12: 738599. doi: 10.3389/fneur.2021.738599
Fraser CL (2022) Visual Snow: Updates on Pathology. Curr Neurol Neurosci Rep 22: 209-217. doi: 10.1007/s11910-022-01182-x
Graber M, Scutelnic A, Klein A, Puledda F, Goadsby PJ, Schankin CJ (2022) Natural course of visual snow syndrome: a long-term follow-up study. Brain Commun 4: fcac230. doi: 10.1093/braincomms/fcac230
Klein A, Schankin CJ (2021a) Visual Snow Syndrome as a Network Disorder: A Systematic Review. Front Neurol 12: 724072. doi: 10.3389/fneur.2021.724072
Klein A, Schankin CJ (2021b) Visual snow syndrome, the spectrum of perceptual disorders, and migraine as a common risk factor: A narrative review. Headache 61: 1306-1313. doi: 10.1111/head.14213
Lauschke JL, Plant GT, Fraser CL (2016) Visual snow: A thalamocortical dysrhythmia of the visual pathway? J Clin Neurosci 28: 123-7. doi: 10.1016/j.jocn.2015.12.001
Liu GT, Schatz NJ, Galetta SL, Volpe NJ, Skobieranda F, Kosmorsky GS (1995) Persistent positive visual phenomena in migraine. Neurology 45: 664-8. doi: 10.1212/wnl.45.4.664
McKendrick AM, Chan YM, Tien M, Millist L, Clough M, Mack H, Fielding J, White OB (2017) Behavioral measures of cortical hyperexcitability assessed in people who experience visual snow. Neurology 88: 1243-1249. doi: 10.1212/WNL.0000000000003784
Mehta DG, Garza I, Robertson CE (2021) Two hundred and forty-eight cases of visual snow: A review of potential inciting events and contributing comorbidities. Cephalalgia 41: 1015-1026. doi: 10.1177/0333102421996355
Metzler AI, Robertson CE (2018) Visual Snow Syndrome: Proposed Criteria, Clinical Implications, and Pathophysiology. Curr Neurol Neurosci Rep 18: 52. doi: 10.1007/s11910-018-0854-2
Naguy A, Naguy C, Singh A (2022) Probable Methylphenidate-Related Reversible “Visual Snow” in a Child With ADHD. Clin Neuropharmacol 45: 105-106. doi: 10.1097/WNF.0000000000000512
Patel RC, Vitale AT, Creel DJ, Digre KB (2021) Not All That Flickers Is Snow. J Neuroophthalmol 41: e97-e99. doi: 10.1097/WNO.0000000000000935
Puledda F, Bruchhage M, O’Daly O, Ffytche D, Williams SCR, Goadsby PJ (2020a) Occipital cortex and cerebellum gray matter changes in visual snow syndrome. Neurology 95: e1792-e1799. doi: 10.1212/WNL.0000000000010530
Puledda F, Schankin C, Goadsby PJ (2020b) Visual snow syndrome: A clinical and phenotypical description of 1,100 cases. Neurology 94: e564-e574. doi: 10.1212/WNL.0000000000008909
Puledda F, Vandenbussche N, Moreno-Ajona D, Eren O, Schankin C, Goadsby PJ (2022) Evaluation of treatment response and symptom progression in 400 patients with visual snow syndrome. Br J Ophthalmol 106: 1318-1324. doi: 10.1136/bjophthalmol-2020-318653
Sampatakakis SN, Lymperopoulos L, Mavridis T, Karagiorgis G, Papadopoulos C, Deligianni CI, Mitsikostas DD (2022) Visual snow: A systematic review and a case series. Cephalalgia 42: 1409-1419. doi: 10.1177/03331024221118917
Schankin CJ, Goadsby PJ (2015) Visual snow–persistent positive visual phenomenon distinct from migraine aura. Curr Pain Headache Rep 19: 23. doi: 10.1007/s11916-015-0497-9
Schankin CJ, Maniyar FH, Digre KB, Goadsby PJ (2014) ‘Visual snow’ – a disorder distinct from persistent migraine aura. Brain 137: 1419-28. doi: 10.1093/brain/awu050
Solly EJ, Clough M, Foletta P, White OB, Fielding J (2021) The Psychiatric Symptomology of Visual Snow Syndrome. Front Neurol 12: 703006. doi: 10.3389/fneur.2021.703006
Solly EJ, Clough M, McKendrick AM, Foletta P, White OB, Fielding J (2020) Ocular motor measures of visual processing changes in visual snow syndrome. Neurology 95: e1784-e1791. doi: 10.1212/WNL.0000000000010372
Strik M, Clough M, Solly EJ, Glarin R, White OB, Kolbe SC, Fielding J (2022) Microstructure in patients with visual snow syndrome: an ultra-high field morphological and quantitative MRI study. Brain Commun 4: fcac164. doi: 10.1093/braincomms/fcac164
Strik M, Clough M, Solly EJ, Glarin R, White OB, Kolbe SC, Fielding J (2023) Brain network dynamics in people with visual snow syndrome. Hum Brain Mapp 44: 1868-1875. doi: 10.1002/hbm.26176
Tsang T, Shidlofsky C, Mora V (2022) The efficacy of neuro-optometric visual rehabilitation therapy in patients with visual snow syndrome. Front Neurol 13: 999336. doi: 10.3389/fneur.2022.999336
Werner RN, Gustafson JA (2022) Case Report: Visual Snow Syndrome after Repetitive Mild Traumatic Brain Injury. Optom Vis Sci 99: 413-416. doi: 10.1097/OPX.0000000000001862
White OB, Clough M, McKendrick AM, Fielding J (2018) Visual Snow: Visual Misperception. J Neuroophthalmol 38: 514-521. doi: 10.1097/WNO.0000000000000702
Yildiz FG, Turkyilmaz U, Unal-Cevik I (2019) The Clinical Characteristics and Neurophysiological Assessments of the Occipital Cortex in Visual Snow Syndrome With or Without Migraine. Headache 59: 484-494. doi: 10.1111/head.13494
Yoo YJ, Yang HK, Choi JY, Kim JS, Hwang JM (2020) Neuro-ophthalmologic Findings in Visual Snow Syndrome. J Clin Neurol 16: 646-652. doi: 10.3988/jcn.2020.16.4.646
![]()