By Marcello Cherchi, MD PhD
For patients
Your doctor may check your hearing at the bedside using one or more simple, quick tests. Some of these tests do not require any tools, such as when the doctor rubs fingers near your ear or whispers near your ear. Other tests involve the use of vibrating tuning forks. Each of these tests is brief, and even when combined, they usually take less than a minute. They are not uncomfortable. You do not need any special preparation for these tests. There are no specific things to do after these tests. If the results from these bedside tests are abnormal, then your doctor may suggest that you get a formal hearing test.
For clinicians
Overview
There is a variety of bedside tests that can assess for hearing loss, some of which require no instruments (finger rub test, whisper test), and others which require a tuning fork (Rinne’s test, Weber’s test). The tuning fork tests can distinguish between sensorineural and conductive hearing loss, while the other tests (finger rub, whisper) cannot. It is important to keep in mind that the tuning fork test only assesses hearing at the single frequency of the tuning fork. All these bedside tests comprise easy and reasonable screening tools, but are not a substitute for formal audiometry. If these screening tests are abnormal, or if there is a high suspicion for clinically relevant hearing loss, then it is appropriate to check formal audiometry.
Introduction
There are several bedside hearing tests that serve as reasonable screening tools, though none is a substitute for instrumented audiometry. The main tests are:
- Finger rub test
- Whisper test
- Rinne’s test
- Weber’s test
We will discuss each of these in turn.
Test: finger rub
For the finger rub test the examiner faces the patient and extends the arm laterally so as to be about 3 feet lateral from one of the patient’s ears. The examiner instructs the patient to say when she or he can hear the fingers rubbing. It is preferable for the patient to close their eyes during this test so that visual cues do not influence “auditory perception.” The examiner then rubs the thumb along the distal pads of the fingers of the same hand and gradually moves that hand towards the patient’s ear. At the point at which the patient states they can hear the finger rubbing, the examiner records that distance. The examiner then repeats the procedure for the other ear.
The Figure below, from Torres-Russotto and colleagues (Torres-Russotto et al. 2009), illustrates this procedure.

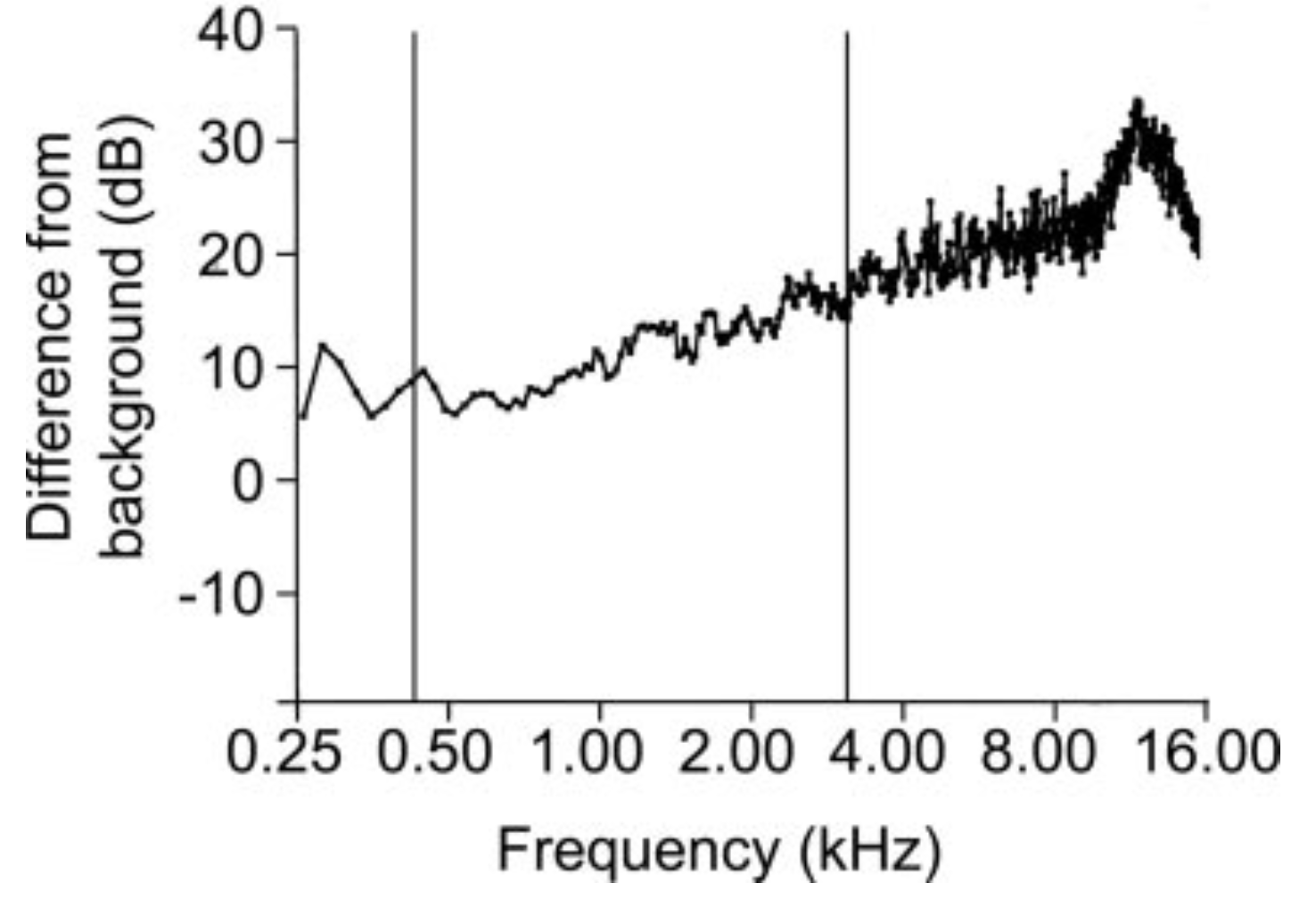
The finger rub test provides an auditory stimulus primarily in the middle and high frequencies. The Figure below, from Torres-Russotto and colleagues (Torres-Russotto et al. 2009), is a histogram showing the difference between the background noise level and the finger rub stimulus level (and thus the degree to which the auditory stimulus exceeds the background noise), and shows a predominantly upsloping pattern, reflecting that this test is a better assessment of middle and higher frequencies.
According to Torres-Russotto and colleagues (Torres-Russotto et al. 2009), compared to portable audiometry, the finger rub test has a specificity and positive predictive value of 100%, and a sensitivity and negative predictive value of 99%, for hearing loss.
Not all investigators arrived as such impressive results. Ting and Huang (Ting and Huang 2023) reported that in comparison to portable audiometry, the finger rub test in patients 65 – 80 years had a sensitivity of 54% and a specificity of 94%, while in patients >80 years it had a sensitivity of 64% and specificity of 89%.
Note that the finger rub test can identify hearing loss, but cannot distinguish sensorineural from conductive hearing loss.
Test: whisper test
In the whisper test the examiner comes close to the patient such that the examiner’s mouth is a few inches away from the patient’s ear, and then whispers several words. The patient repeats back the words heard. If the patient repeats some proportion of words correctly, then that ear has “passed,” otherwise it has “failed.” The examiner repeats the procedure on the patient’s other ear, using different words, and scores the patient’s performance similarly.
There are different protocols for conducting and interpreting the whisper test. A literature review by Pirozzo and colleagues (Pirozzo et al. 2003) found that four studies in adults reported that the sensitivity ranged from 90 – 100% and the specificity ranged from 70 – 87%, and four studies in children reported that the sensitivity ranged from 80 – 96% and the specificity ranged from 90 – 98%.
Note that the whisper test can identify hearing loss, but cannot distinguish sensorineural from conductive hearing loss.
Tests using a tuning fork
A large number of tuning fork tests of hearing have been proposed over the centuries (Ng and Jackler 1993). The ones most prevalent in clinical medicine are Rinne’s test and Weber’s test. There is debate regarding whether steel or aluminum tuning forks are best (Mackechnie et al. 2013). Most clinicians use a 128 Hz or 256 Hz tuning fork. Otoneurologists often prefer to use the 128 Hz tuning fork in the interest of detecting the low frequency sensorineural hearing loss associated with Meniere’s disease.
Test: Rinne’s test
Heinrich Adolf Rinne (1819-1868) described a tuning fork test that differentiated between sensorineural hearing loss and conductive hearing loss. Ng and Jackler (Rinne 1855) translate Rinne’s description of his experimental results as follows:
“If the result of this experiment performed on a deaf person is the same as on a normal one, then we are justified in concluding that the condition of the entire conduction apparatus is normal. Therefore, the auditory nerve must be the diseased part. If, however, the patient hears the sound transmitted by the bone as long or even longer than he hears it in the normal way, then we have to assume a disease of one of the parts of the conduction apparatus including the membrana of the fenestra ovalis.”
Rinne’s original experiments involved applying the stem of the tuning fork to the patient’s teeth. For the technique of applying the stem of the tuning fork to the mastoid process, Ng. and Jackler (Ng and Jackler 1993) credit Johann Constantin August Lucae (1835-1911) (Lucae 1882).
Today the examiner performs this test by stimulating the tines of the tuning fork, firmly applying the stem of the tuning fork to the patient’s mastoid (providing a bone-conducted stimulus), and asking the patient to signal when they no longer hear the tone; that point reflects the threshold of conductive hearing in that ear at that frequency. Then the examiner quickly removes the tuning fork’s stem from the patient’s mastoid and brings the tines very close to the patient’s external ear (providing an air-conducted stimulus); the examiner then asks the patient whether they hear the tone again.
- If the patient responds “yes,” then that indicates that air conduction is better than bone conduction.
- If the patient responds “no,” then that indicates that bone conduction is better than air conduction (suggesting conductive hearing loss in that ear at that frequency).
Test: Weber’s test
Ernst Heinrich Weber (1795-1878) provided the original description of this test in 1834 (Weber 1834). According to Ng and Jackler (Ng and Jackler 1993) the clinical utility of the lateralizing result of this test was described by Eduard Schmaltz (Schmaltz 1846).
After stimulating the tines, the examiner applies the stem of the tuning fork to the center of the forehead and asks the patient whether they hear the tone “in the middle” or “more on one side.”
In the identification of conductive hearing loss (see below), the reported sensitivity of Weber’s test is variable (Shuman et al. 2013), and appears to depend in part on the frequency tested (Abdullah et al. 2022).
Test: combining Weber’s and Rinne’s tests
If, with a specific frequency tuning fork, Weber’s test lateralizes to a particular side, then the examiner performs Rinne’s test on that side.
- If on that side (the side to which Weber’s test lateralizes) air conduction is better than bone conduction, then that means there is contralateral sensorineural hearing loss at that frequency.
- If on that side (the side to which Weber’s test lateralizes) bone conduction is better than air conduction, then that means there is ipsilateral conductive hearing loss at that frequency.
For possibility #2 (bone conduction is better than air conduction), Rinne’s test alone (without the lateralizing information from Weber’s test) already tells us that there is conductive hearing loss on that side. So what is Weber’s test adding in this circumstance?
In fact, why does Weber’s test lateralize to the side with conductive hearing loss at all? This has been debated (Mbubaegbu and Kroukamp 2002), but ultimately is thought to be due to Bing’s phenomenon, after Alfred Bing’s observations (Bing 1891), also called the occlusion phenomenon by Tonndorf and colleagues (Tonndorf et al. 1966). Csovanyos (Csovanyos 1961) summarized Bing’s insight as follows:
“He explained this phenomenon with Mach’s theory of bone conduction. According to this theory, the vibratory energy is transferred to the cochlea from the vibrating head [caused by application of the tuning fork]. Since ‘the sound conducting apparatus’ is well adapted for transmitting sound energy from the air to the labyrinth, according to the law of reciprocity, it is equally well adapted for transmitting energy in the opposite direction. An obturation of the [external auditory] meatus, which stops the drain [of kinetic energy into the external environment], increases the level of kinetic energy in the labyrinth and increases bone conduction” (Csovanyos 1961).
In other words, in conductive hearing loss, the kinetic energy (from the head vibrating) that would usually “escape” into the outside world, instead remains in the temporal bone and stimulates the cochlea, and thus the patient will perceive that stimulus more strongly ipsilateral to the conductive hearing loss than contralaterally (assuming that contralateral hearing is normal).
So in essence, when Weber’s test lateralizes to a particular side, then at that frequency there is either ipsilateral conductive hearing loss, or contralateral sensorineural hearing loss, and applying Rinne’s test distinguishes between the two. The combined use of Weber’s and Rinne’s tests is superior to either test used in isolation (Miltenburg 1994).
Criticism of tuning-fork-based assessments of hearing cites their variability (Kelly et al. 2018), and inferior sensitivity and specificity compared to standard audiometry (Stankiewicz and Mowry 1979). While we view tuning-fork-based tests as reasonable screening tools, we would agree that they are not a substitute for formal audiometry, particularly when there is a high clinical index of suspicion.
References
Abdullah SN, Zakaria MN, Salim R, Md Daud MK, Nik Othman NA (2022) Comparing the diagnostic accuracy of audiometric Weber test and tuning fork Weber test in patients with conductive hearing loss. Laryngoscope Investig Otolaryngol 7: 523-529. doi: 10.1002/lio2.747
Bing A (1891) Ein neuer Stimmgabelversuch. Beitrag zur Differential-Diagnostik der Krankheiten des mechanischen Schallleitungs- und nervösen Hörapparates [A new tuning fork test. A contribution to the differential diagnosis of the diseases of the conductive and perceptive hearing apparatus]. Wiener medizinische Blätter 41.
Csovanyos L (1961) The Bing test in the diagnosis of deafness. Laryngoscope 71: 1548-60. doi: 10.1288/00005537-196112000-00004
Kelly EA, Li B, Adams ME (2018) Diagnostic Accuracy of Tuning Fork Tests for Hearing Loss: A Systematic Review. Otolaryngol Head Neck Surg 159: 220-230. doi: 10.1177/0194599818770405
Lucae A (1882) Buchbesprechung [Book review]. Arch Ohr Nas 16: 88.
Mackechnie C, Greenberg J, Gerkin R, McCall A, Hirsch B, Durrant J, Raz Y (2013) Rinne Revisited: Steel versus Aluminum Tuning Forks. Otolaryngology–head and neck surgery : official journal of American Academy of Otolaryngology-Head and Neck Surgery 147. doi: 10.1177/0194599813505828
Mbubaegbu CE, Kroukamp G (2002) Weber’s test demystified: Physics renders Weber’s test not so mysterious… and a collaborative group of otorhinolaryngologists reports its findings. BMJ 325: 1117. doi: 10.1136/bmj.325.7372.1117
Miltenburg DM (1994) The validity of tuning fork tests in diagnosing hearing loss. J Otolaryngol 23: 254-9.
Ng M, Jackler RK (1993) Early history of tuning-fork tests. Am J Otol 14: 100-5.
Pirozzo S, Papinczak T, Glasziou P (2003) Whispered voice test for screening for hearing impairment in adults and children: systematic review. BMJ 327: 967. doi: 10.1136/bmj.327.7421.967
Rinne HA (1855) Beitrage zur Physiologie des menschlichen Ohres. vol 45. Prague: Kark Andre Publishers
Schmaltz E (1846) Erfahrungen über die Krankheiten des Gehöres und ihre Heilung [Practice of hearing diseases and their treatment]. B.G. Teubner, Leipzig
Shuman AG, Li X, Halpin CF, Rauch SD, Telian SA (2013) Tuning fork testing in sudden sensorineural hearing loss. JAMA Intern Med 173: 706-7. doi: 10.1001/jamainternmed.2013.2813
Stankiewicz JA, Mowry HJ (1979) Clinical accuracy of tuning fork tests. Laryngoscope 89: 1956-63. doi: 10.1288/00005537-197912000-00009
Ting HC, Huang YY (2023) Sensitivity and specificity of hearing tests for screening hearing loss in older adults. J Otol 18: 1-6. doi: 10.1016/j.joto.2022.11.003
Tonndorf J, Campbell RA, Bernstein L, Reneau JP (1966) Quantitative Evaluation of Bone Conduction Components in Cats. Acta Oto-Laryngologica 61: 10-38. doi: 10.3109/00016486609120797
Torres-Russotto D, Landau WM, Harding GW, Bohne BA, Sun K, Sinatra PM (2009) Calibrated finger rub auditory screening test (CALFRAST). Neurology 72: 1595-600. doi: 10.1212/WNL.0b013e3181a41280
Weber EH (1834) De pulsu, resorptione, auditu et tactu. Annotationes anatomicae et physiologicae, auctore. prostat apud C.F. Koehler, Leipzig
![]()