By Marcello Cherchi, MD PhD
For patients
Here are answers to some of the most common questions about tilt table testing (TTT).
|
What is this test? |
Tilt table testing (TTT) assesses how the body regulates blood pressure and heart rate in response to changes in the body’s position. |
|
What is this test looking for? |
This test measures blood pressure and heart rate while the body is supine (lying down) and tilted almost upright. |
|
Is this test experimental or investigational? |
This test is approved by the Food and Drug Administration. It is neither experimental nor investigational. |
|
What happens during this test? |
During this test the technician secures you to a table and attaches devices for measuring blood pressure and heart rate. For several minutes you will be lying down. For several minutes you will be tilted partially upright. |
|
Is this test uncomfortable? |
Occasionally patients faint during this test, but they are safe because they are secured to the table. |
|
How long does this test take? |
The test takes about 30 – 45 minutes. |
|
Do I have to prepare for this test? |
Make sure you tell the technicians the medications you are currently taking. There are otherwise no specific preparations for this test. |
|
Are there any special instructions for what to do after the test? |
There are no special instructions for what to do after this test. |
For clinicians
Overview
Tilt table testing (TTT) systematically tracks blood pressure and cardiac pulse rate every minute while a patient is supine for several minutes, then tilted upright (usually at 70 degrees) for several minutes. This test can be helpful in recognizing several diagnoses, including orthostatic hypotension (immediate and delayed) and postural orthostatic tachycardia.
Introduction
Humans spend more time in an upright position (seated, standing, walking) than in a supine, prone or recumbent position. Gravity imposes different hydraulic parameters in these positions. The cardiovascular system must recognize when these parameters change, and make adjustments to accommodate them.
Dr. Rose Anne Kennny, Dr. John Bayliss, Dr. Ann Inram and Dr. Richard Sutton (Kenny et al. 1986) originally proposed the tilt table test (TTT) as a method for investigating unexplained syncope. Since its introduction some investigators have embraced its diagnostic utility (Cheshire and Goldstein 2019), others have been more cautious (Grubb and Kosinski 1997), and others have suggested that it be completely omitted from the repertoire of clinical testing (Kulkarni et al. 2020).
While TTT is not a vestibular test in the traditional sense, we view it as playing a role in evaluating several potential cardiovascular etiologies of symptoms that drive patient referrals.
Physiology
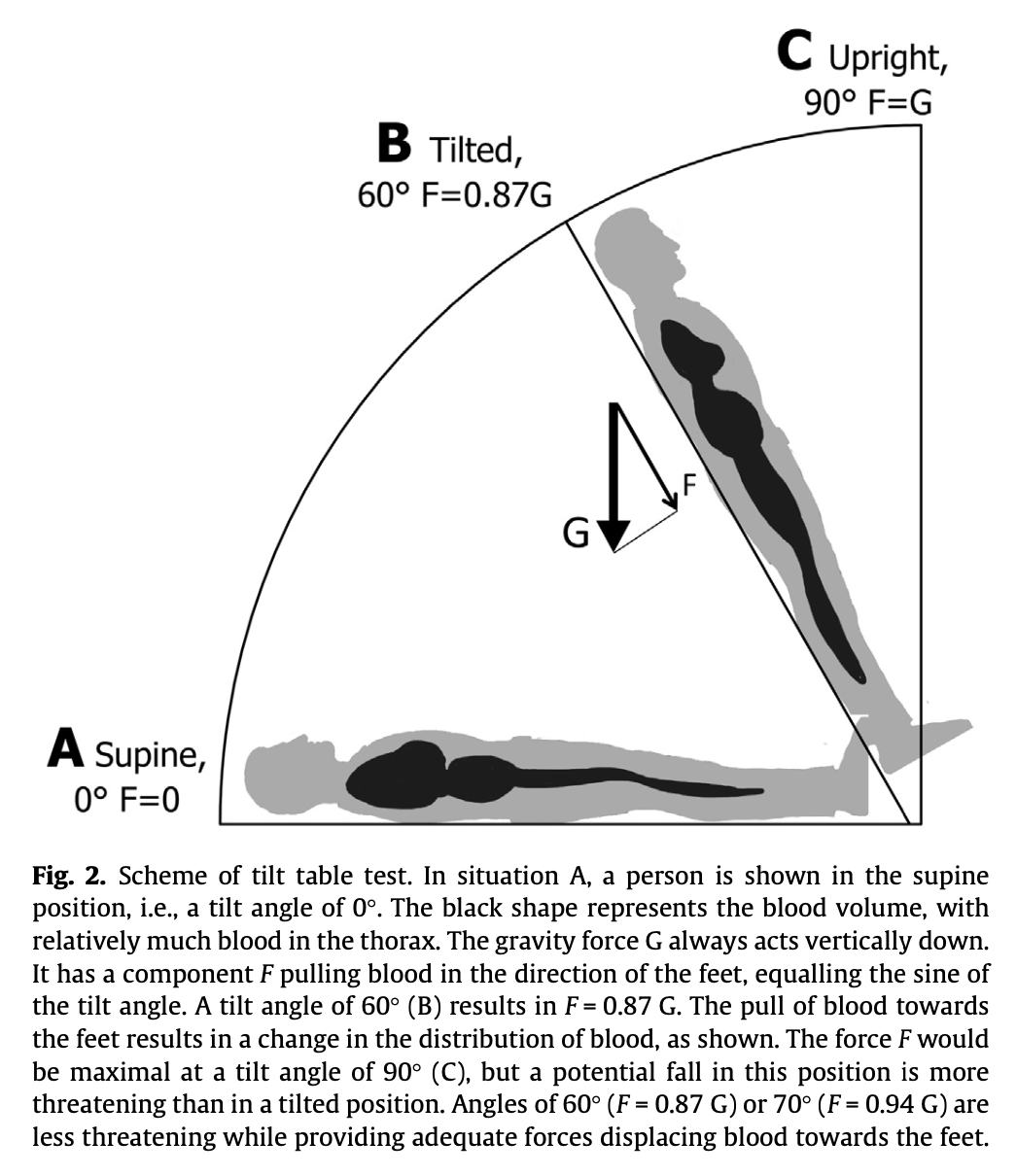
When a person goes from a supine to a standing position, gravity pulls blood downwards; if there are no compensatory adjustments, then blood will tend to pool in the venous system of the lower extremities, and that much less blood will be available higher up in the body — and in particular, there will be the risk of cerebral hypoperfusion.
The Figure below, from Saal and colleagues (Saal et al. 2016), illustrates the redistribution of blood as a function of gravity during tilt table testing.
The cardiovascular system can sense this hydraulic change through several mechanisms. One of the more important mechanisms are the stretch receptors in the carotid sinus. When blood pressure is elevated, the carotid sinus stretch receptors are stimulated, and this triggers the cardiovascular system to lower blood pressure. When blood pressure is low, the carotid sinus stretch receptors are not stimulated, and this triggers the cardiovascular system to raise blood pressure.
The vestibular system, and specifically the otolith system which senses the direction of the linear acceleration of gravity, likely also has input in the cardiovascular system’s regulation of blood pressure and cardiac pulse rate (Aoki et al. 2012; Serrador et al. 2009; Yates 1998), though this has not been studied as thoroughly.
The cardiovascular system has several mechanisms at its disposal to change blood pressure on a moment-to-moment basis. The main ones are:
- Adjusting heart rate.
- Adjusting vasodilation/vasoconstriction.
- Adjusting cardiac ejection fraction.
In a healthy individual, when going from a supine to an upright position, gravity will begin to bring about a drop in blood pressure. In order to offset this impending drop in blood pressure, the cardiovascular system responds with the mechanisms mentioned earlier (increasing the heart rate, constricting blood vessels, increasing the cardiac ejection fraction). The result of these responses is that blood pressure does not drop excessively.
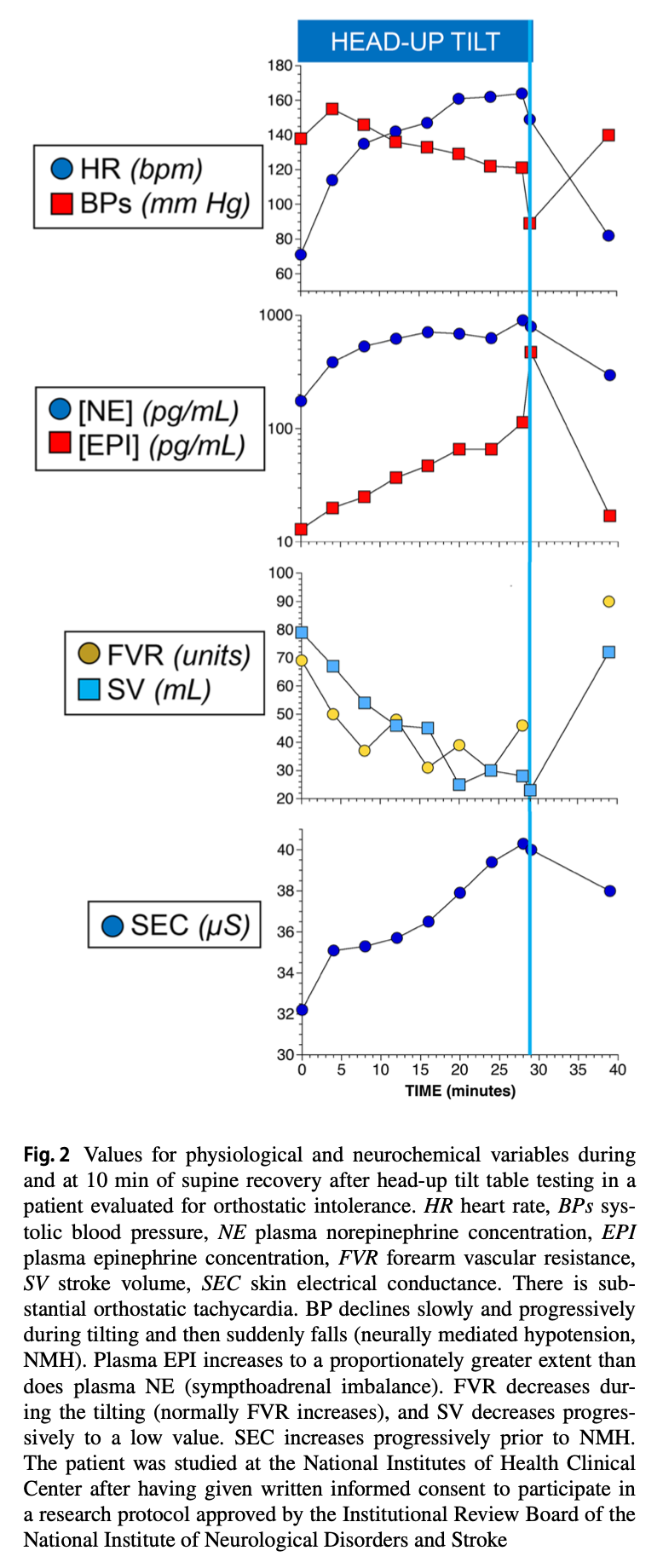
The Figure below, from Cheshire and Goldstein (Cheshire and Goldstein 2019), provides idealized graphs of several physiologic variables during tilt table testing.
Equipment needed
A variety of tilt tables is available for clinical purposes. What they have in common is the ability to change a patient’s position from supine to upright (generally 70 degrees head upright tilt). During the test, once per minute the patient’s cardiac pulse rate is measured (often by pulse oximetry) and blood pressure is measured (by an automated blood pressure cuff). Results are logged. In some cases the technologist will also record syncope, or symptoms reported by the patient.
How to perform the test
There are several protocols for tilt table testing. A common protocol is to have the patient lie supine for 7 minutes, then engage the 70 degree head upright tilt position for 20 minutes, then resume the supine position for several minutes.
The Figure below, from Cheshire and Goldstein (Cheshire and Goldstein 2019), provides a schematic of the two positions from a typical tilt table test protocol.
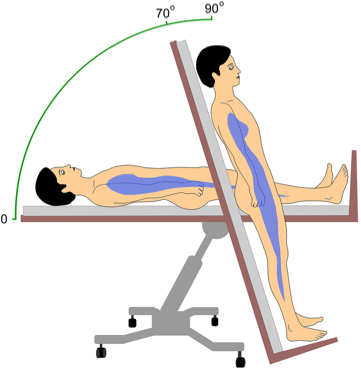
Figure : Schematic of the two positions from a common tilt table test protocol. From Cheshire and Goldstein (2019).
When tilt table testing is conducted by cardiologists, it may also be performed after administering sublingual nitroglycerine (Aerts 2003), which is a pure vasodilator (at low doses it causes more venous dilation than arterial dilation), and does not directly affect cardiac rhythm. Cardiologists do this in order to assess the response of cardiac rhythm when the pharmacologically-induced drop in blood pressure occurs. In an otoneurology clinic, the nitroglycerine component of tilt table testing is usually not performed.
What this test assesses
In tilt table testing (TTT) the independent variable is the vector of gravity (controlled by the degree to which the table is tilted), and the dependent variables are the cardiac pulse rate and the systolic and diastolic blood pressures.
Tilt table testing (TTT) checks cardiac pulse rate and blood pressure every minute for several minutes while a patient lies supine, then for several minutes when the patient is partially upright.
How to interpret the test results
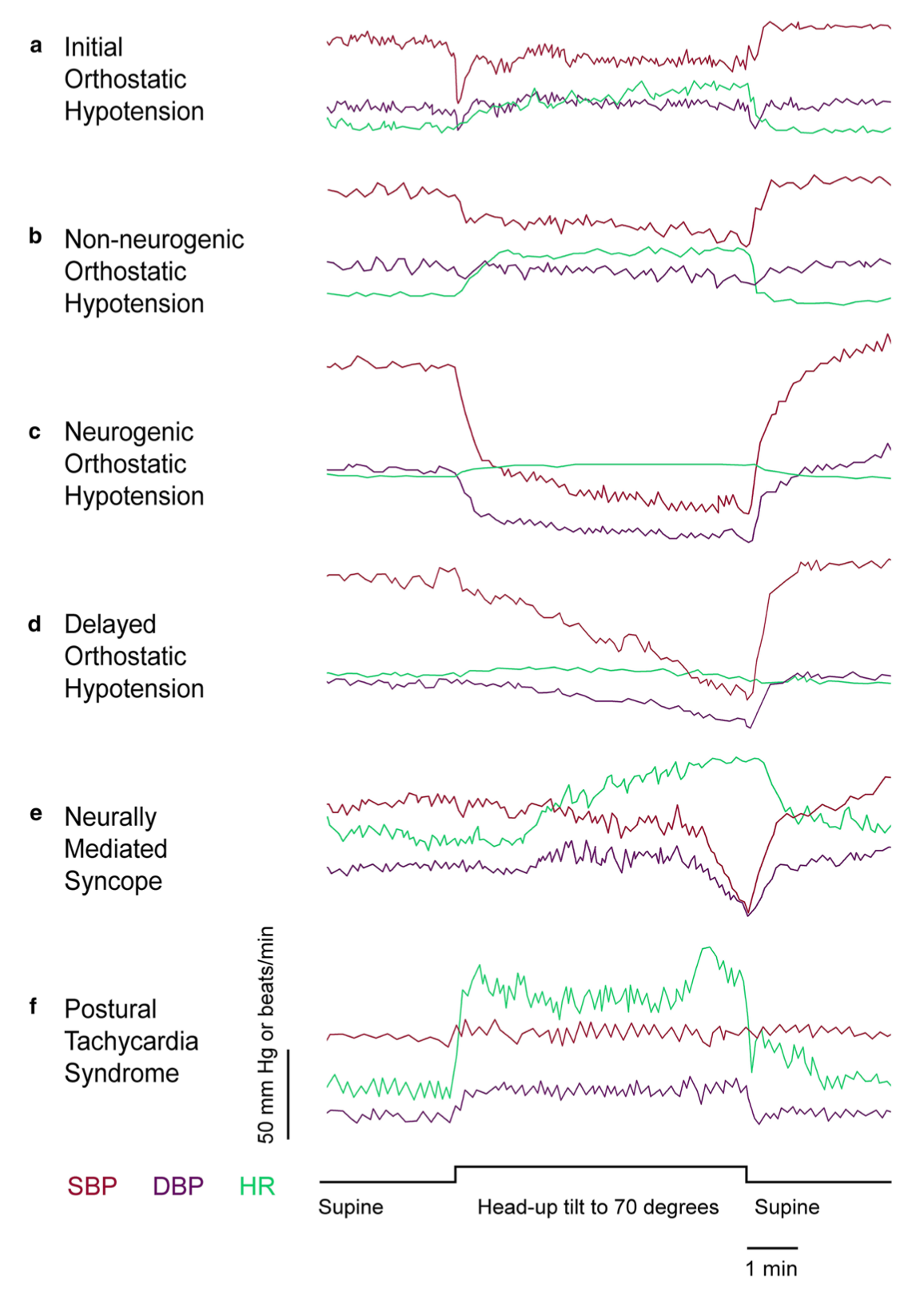
The Figure below, from Cheshire and Goldstein (Cheshire and Goldstein 2019), illustrates examples of several patterns of results from tilt table testing associated with various diagnoses.
The particular criteria for each diagnosis have been debated. For example, there have been several consensus statements regarding the criteria for orthostatic hypotension ([No authors] 1996a, b, c; Kaufmann 1996).
Limitations
Keep in mind that in patients with cardiac pacemakers, the heart rate will not fall below the preset “floor” level (usually 60 beats per minute) of the pacemaker.
Contraindications
Benditt and colleagues (Benditt et al. 1996) list the following contraindications to tilt table testing:
- Syncope with clinically severe left ventricular outflow obstruction.
- Syncope in the presence of critical mitral stenosis.
- Syncope in the setting of known critical proximal coronary artery stenoses.
- Syncope in conjunction with known critical cerebrovascular stenoses.
Pitfalls
Autonomic control of blood pressure and cardiac pulse rate can be manipulated by a variety of medications. The interpretation of results from tilt table testing should take into account a patient’s current medications.
When is the test indicated
It is medically reasonable to consider tilt table testing in patients who complain of episodes of lightheadedness when upright.
Diseases that may be diagnosed by this test
Tilt table testing (TTT) was originally designed to assess for drops in blood pressure that culminated in syncope (Kenny et al. 1986).
The Figure below, from Grubb and Kosinski (Grubb and Kosinski 1997), shows potential results from TTT.

Patients are generally not referred to an otoneurology clinic for a complaint of syncope. They are more commonly referred for disequilibrium, and in some patients, lightheadedness (presyncope) falls within this category.
The cardiovascular phenomena that can manifest with presyncopal lightheadedness are those that cause cerebral hypoperfusion from a drop in systemic blood pressure. These include:
- Orthostatic hypotension.
- Postural orthostatic tachycardia. The tachycardic response may compensate for what would otherwise have been a drop in blood pressure, but sometimes this compensation is incomplete.
- Cardiac arrhythmia.
The first two (orthostatic hypotension, postural orthostatic tachycardia) can be diagnosed on tilt table testing. The last (cardiac arrhythmia) is usually diagnosed by cardiac monitoring.
Checking orthostatic blood pressure and cardiac pulse rate on bedside physical examination can sometimes catch immediate orthostatic changes. However, this will miss changes that occur minutes after a positional change, such as delayed orthostatic hypotension (Gibbons and Freeman 2020).
Additional notes
Tilt table testing is one of a number of tools that can be used for evaluating the function of the autonomic nervous system. Other autonomic tests include:
- Pupillometry
- Quantitative sudomotor axon reflex test
- Thermoregulatory sweat test
- Heart rate variability
- Valsalva ratio
- Plasma norepinephrine levels
- Cardiac meta-iodobenzylguanidine (MIBG)
An otoneurology clinic may identify autonomic dysfunction on tilt table testing, but after that, referral to an autonomic specialist is often necessary to characterize the disorder in greater detail, with the goal of reaching a diagnosis and instituting treatment.
References
[No authors] (1996a) Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. J Neurol Sci 144: 218-9.
[No authors] (1996b) Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. The Consensus Committee of the American Autonomic Society and the American Academy of Neurology. Neurology 46: 1470.
[No authors] (1996c) The definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. J Auton Nerv Syst 58: 123-4.
Aerts AJ (2003) Nitrate stimulated tilt table testing: a review of the literature. Pacing Clin Electrophysiol 26: 1528-37. doi: 10.1046/j.1460-9592.2003.t01-1-00222.x
Aoki M, Sakaida Y, Tanaka K, Mizuta K, Ito Y (2012) Evidence for vestibular dysfunction in orthostatic hypotension. Exp Brain Res 217: 251-9. doi: 10.1007/s00221-011-2989-0
Benditt DG, Ferguson DW, Grubb BP, Kapoor WN, Kugler J, Lerman BB, Maloney JD, Raviele A, Ross B, Sutton R, Wolk MJ, Wood DL (1996) Tilt table testing for assessing syncope. American College of Cardiology. J Am Coll Cardiol 28: 263-75. doi: 10.1016/0735-1097(96)00236-7
Cheshire WP, Jr., Goldstein DS (2019) Autonomic uprising: the tilt table test in autonomic medicine. Clin Auton Res 29: 215-230. doi: 10.1007/s10286-019-00598-9
Gibbons CH, Freeman R (2020) Delayed orthostatic hypotension. Auton Neurosci 229: 102724. doi: 10.1016/j.autneu.2020.102724
Grubb BP, Kosinski D (1997) Tilt table testing: concepts and limitations. Pacing Clin Electrophysiol 20: 781-7. doi: 10.1111/j.1540-8159.1997.tb03904.x
Kaufmann H (1996) Consensus statement on the definition of orthostatic hypotension, pure autonomic failure and multiple system atrophy. Clin Auton Res 6: 125-6.
Kenny RA, Ingram A, Bayliss J, Sutton R (1986) Head-up tilt: a useful test for investigating unexplained syncope. Lancet 1: 1352-5. doi: 10.1016/s0140-6736(86)91665-x
Kulkarni N, Mody P, Levine BD (2020) Abolish the Tilt Table Test for the Workup of Syncope! Circulation 141: 335-337. doi: 10.1161/CIRCULATIONAHA.119.043259
Saal DP, Thijs RD, van Dijk JG (2016) Tilt table testing in neurology and clinical neurophysiology. Clin Neurophysiol 127: 1022-1030. doi: 10.1016/j.clinph.2015.07.037
Serrador JM, Schlegel TT, Black FO, Wood SJ (2009) Vestibular effects on cerebral blood flow. BMC Neurosci 10: 119. doi: 10.1186/1471-2202-10-119
Yates BJ (1998) Autonomic reaction to vestibular damage. Otolaryngol Head Neck Surg 119: 106-12. doi: 10.1016/S0194-5998(98)70179-2
![]()