By Marcello Cherchi, MD PhD
For patients
Carbon monoxide is a gas that you cannot see or smell. It can hurt many parts of the body, and sometimes cause hearing loss and disequilibrium. There are many ways for carbon monoxide poisoning to happen, but a common cause is a broken heating system in your home. If you think you may have carbon monoxide poisoning, then you should go to an emergency room.
For clinicians
Overview
Carbon monoxide (CO) is a colorless, odorless gas that binds to hemoglobin more avidly than oxygen, which impairs tissue oxygenation. CO intoxication is the most common cause of intentional and unintentional poisoning. CO intoxication, whether acute or chronic, can manifest with a variety of symptoms, including otovestibular ones such as hearing loss and/or disequilibrium. The hearing loss is sensorineural and can be unilateral, bilateral or asymmetrical; this hearing loss is reversible in some cases. In the acute setting (typically an emergency department) treatment is with high-flow 100% oxygen.
Introduction
Carbon monoxide intoxication can manifest with a variety of symptoms. Neurologists are generally familiar with the selective vulnerability of the globus pallidus to carbon monoxide intoxication (Sharma et al. 2009), but it can also manifest with otovestibular symptoms such as hearing loss and/or disequilibrium.
Epidemiology
Carbon monoxide intoxication is the leading cause of intentional and unintentional poisoning in the United States (Thom and Keim 1989), accounting for 50,000 cases annually (Shin et al. 2023). The fact that carbon monoxide is both colorless and odorless increases the risk of accidental intoxication.
Pathophysiological mechanism of disease
Carbon monoxide binds to hemoglobin more avidly than does oxygen, thereby diminishing the blood’s capacity to deliver oxygen to tissues and resulting in ischemia. Other potentially contributory mechanisms include reoxygenation injury and direct toxic effects of carbon monoxide (Zhu et al. 2014).
Clinical presentation
Carbon monoxide intoxication can manifest with a variety of symptoms. Otoneurologically it can manifest with sensorineural hearing loss and disequilibrium. “Dizziness” is among the most common symptoms of carbon monoxide intoxication, reported in 12.4% of cases (Shin et al. 2023). Hearing loss is a less common manifestation of carbon monoxide intoxication, but is important to recognize because the hearing loss is reversible in some cases (Shahbaz Hassan et al. 2003).
Symptoms of carbon monoxide intoxication may become manifest after either acute or chronic exposure. The resulting sensorineural hearing loss can be unilateral or bilateral (Mehrparvar et al. 2013), and when bilateral it can be asymmetrical (Pillion 2012). The hearing loss may fluctuate (Seale et al. 2018), resembling Ménière’s disease. The hearing loss may be reversible or irreversible (Mehrparvar et al. 2013). Carbon monoxide intoxication can also present with isolated disequilibrium (Lakhani and Bleach 2010), or the auditory and vestibular symptoms may occur in combination (Seale et al. 2018).
Ocular motor examination
An experimental study by Tibbling (Tibbling 1969) reported no effect of carbon monoxide on “vestibular nystagmus.” Fielding and colleagues (Fielding et al. 2010) reported that a victim of carbon monoxide intoxication with bilateral globus pallidus lesions exhibited a variety of saccadic abnormalities, including reduced gain in visually-guided saccades, increased errors on antisaccades, higher anticipatory errors in memory-guided saccades and endogenously cued saccades, and shorter intersaccadic intervals in self-paced saccades. There are various reports of cerebellar lesions in carbon monoxide intoxication (Fan et al. 2009; Mascalchi et al. 1996; Velioglu et al. 2013; Zhu et al. 2014), though no clear descriptions of corresponding ocular motor correlates.
Testing: Auditory
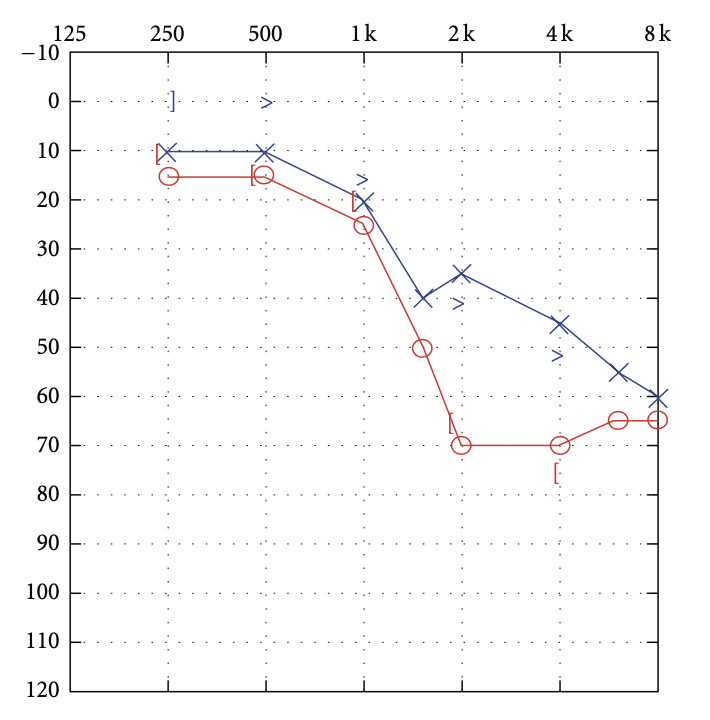
The hearing loss associated with carbon monoxide intoxication is sensorineural. In some cases the hearing loss is asymmetrical.
The Figure below, from Pillon (Pillion 2012), shows right greater than left sided high frequency sensorineural hearing loss.
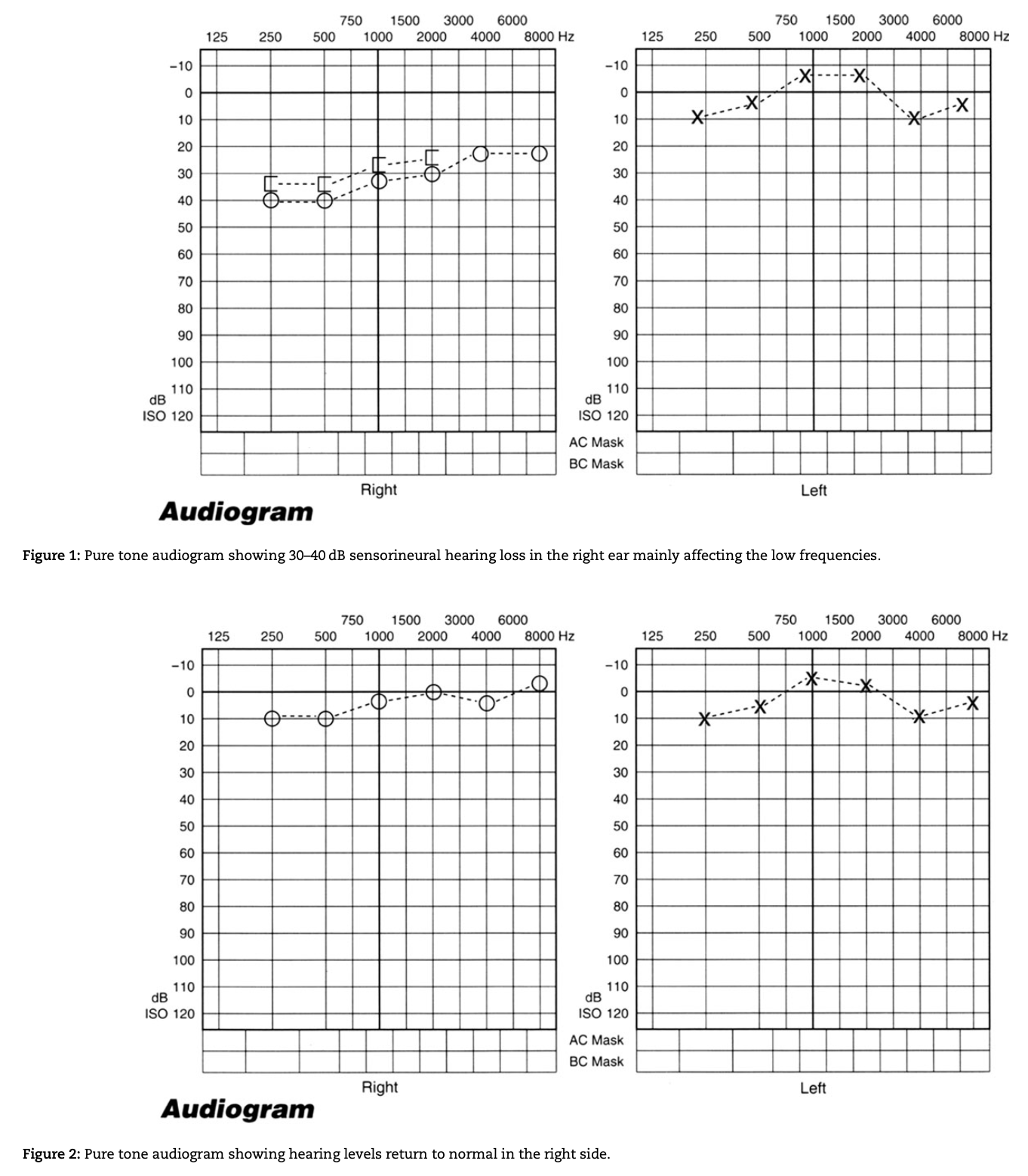
The hearing loss in carbon monoxide intoxication can affect predominantly the low frequencies.
The Figure below, from Seale and colleagues (Seale et al. 2018), shows right sided, predominantly low frequency sensorineural hearing loss, which improved on a subsequent audiogram. This fluctuation in low frequency sensorineural hearing loss can resemble Ménière’s disease.
Testing: other
Carbon monoxide binds to hemoglobin and forms carboxyhemoglobin, measurement of which can support a diagnosis of carbon monoxide intoxication. However, carboxyhemoglobin is not sensitive, as it can appear normal, especially in cases of chronic carbon monoxide exposure. Note that pulse oximetry does not distinguish oxyhemoglobin from carboxyhemoglobin, and thus cannot detect carbon monoxide intoxication.
Imaging
Carbon monoxide intoxication is often described as causing selective damage to the globus pallidus (Jiang et al. 2020), but any distribution of supratentorial and infratentorial lesions is possible (Jeon et al. 2018; Kim et al. 2017).
Histopathology
Histopathological findings in the brain from carbon monoxide intoxication include necrosis in the globus pallidus, and demyelination (Lapresle and Fardeau 1967; Mascalchi et al. 1996; Zhu et al. 2014). Specific findings in the labyrinth and vestibulocochlear nerve have not been described.
Differential diagnosis
Since carbon monoxide intoxication can present with fluctuating low frequency sensorineural hearing loss (Seale et al. 2018), Ménière’s disease is on the differential diagnosis.
Treatment
Acute carbon monoxide intoxication is usually diagnosed in an emergency department, and in this setting patients are treated with high-flow 100% oxygen. Toxicology consultation is reasonable. In some circumstances, hyperbaric oxygen therapy may also be appropriate, though this treatment modality is not widely available.
Prognosis
Carbon monoxide intoxication is a potentially reversible cause of sensorineural hearing loss (Shahbaz Hassan et al. 2003), though there are no clear predictors of this.
References
Fan HC, Wang AC, Lo CP, Chang KP, Chen SJ (2009) Damage of cerebellar white matter due to carbon monoxide poisoning: a case report. Am J Emerg Med 27: 757 e5-7. doi: 10.1016/j.ajem.2008.10.021
Fielding J, Lang W, White OB (2010) Carbon monoxide poisoning: impact on ocular motility. Cogn Behav Neurol 23: 256-61. doi: 10.1097/WNN.0b013e3181c5e2c1
Jeon SB, Sohn CH, Seo DW, Oh BJ, Lim KS, Kang DW, Kim WY (2018) Acute Brain Lesions on Magnetic Resonance Imaging and Delayed Neurological Sequelae in Carbon Monoxide Poisoning. JAMA Neurol 75: 436-443. doi: 10.1001/jamaneurol.2017.4618
Jiang W, Wu Q, Zhou C, Zhao Z, Tan Y (2020) Gray matter nuclei damage in acute carbon monoxide intoxication assessed in vivo using diffusion tensor MR imaging. Radiol Med 125: 80-86. doi: 10.1007/s11547-019-01078-w
Kim DM, Lee IH, Park JY, Hwang SB, Yoo DS, Song CJ (2017) Acute carbon monoxide poisoning: MR imaging findings with clinical correlation. Diagn Interv Imaging 98: 299-306. doi: 10.1016/j.diii.2016.10.004
Lakhani R, Bleach N (2010) Carbon monoxide poisoning: an unusual cause of dizziness. J Laryngol Otol 124: 1103-5. doi: 10.1017/S0022215110000800
Lapresle J, Fardeau M (1967) The central nervous system and carbon monoxide poisoning. II. Anatomical study of brain lesions following intoxication with carbon monixide (22 cases). Prog Brain Res 24: 31-74. doi: 10.1016/s0079-6123(08)60181-8
Mascalchi M, Petruzzi P, Zampa V (1996) MRI of cerebellar white matter damage due to carbon monoxide poisoning: case report. Neuroradiology 38 Suppl 1: S73-4. doi: 10.1007/BF02278124
Mehrparvar AH, Davari MH, Mollasadeghi A, Vahidi MR, Mostaghaci M, Bahaloo M, Shokouh P (2013) Hearing Loss due to Carbon Monoxide Poisoning. Case Rep Otolaryngol 2013: 940187. doi: 10.1155/2013/940187
Pillion JP (2012) Sensorineural Hearing Loss following Carbon Monoxide Poisoning. Case Rep Pediatr 2012: 231230. doi: 10.1155/2012/231230
Seale B, Ahanger S, Hari C (2018) Subacute carbon monoxide poisoning presenting as vertigo and fluctuating low frequency hearing loss. J Surg Case Rep 2018: rjy205. doi: 10.1093/jscr/rjy205
Shahbaz Hassan M, Ray J, Wilson F (2003) Carbon monoxide poisoning and sensorineural hearing loss. J Laryngol Otol 117: 134-7. doi: 10.1258/002221503762624602
Sharma S, Gupta R, Paul BS, Puri S, Garg S (2009) Accidental carbon monoxide poisoning in our homes. Indian J Crit Care Med 13: 169-70. doi: 10.4103/0972-5229.58546
Shin M, Bronstein AC, Glidden E, Malone M, Chang A, Law R, Boehmer TK, Strosnider H, Yip F (2023) Morbidity and Mortality of Unintentional Carbon Monoxide Poisoning: United States 2005 to 2018. Ann Emerg Med 81: 309-317. doi: 10.1016/j.annemergmed.2022.10.011
Thom SR, Keim LW (1989) Carbon monoxide poisoning: a review epidemiology, pathophysiology, clinical findings, and treatment options including hyperbaric oxygen therapy. J Toxicol Clin Toxicol 27: 141-56. doi: 10.3109/15563658909038578
Tibbling L (1969) The influence of tobacco smoking, nicotine, CO and CO2 on vestibular nystagmus. Acta Otolaryngol 68: 118-26. doi: 10.3109/00016486909121549
Velioglu M, Gumus T, Husmen G (2013) Cerebellar lesions in the acute setting of carbon monoxide poisoning. Emerg Radiol 20: 255-7. doi: 10.1007/s10140-013-1108-x
Zhu L, Zhou C, Wu J, Fang S (2014) Rare cerebellar lesions in a carbon monoxide poisoning case. Neurol Sci 35: 117-9. doi: 10.1007/s10072-013-1506-6
![]()