By Marcello Cherchi, MD PhD
For patients
Benign paroxysmal positional vertigo (BPPV) is treated by moving a person’s head through several positions. Some researchers believe that this kind of treatment can be done using special mechanical chairs, and that it may be better than regular physical therapy treatment.
For clinicians
Practical summary
Several mechanical chairs have been developed for the treatment of benign paroxysmal positional vertigo (BPPV). The literature on this topic is emerging; some of it suggests that these mechanical chairs facilitate greater accuracy, others emphasize greater treatment efficacy, compared to standard manual therapy for BPPV.
Introduction
Benign paroxysmal positional vertigo (BPPV) is fundamentally a mechanical problem, and its treatment is also mechanical — canalith repositioning maneuvers. Depending on the canal (or canals) affected by BPPV, different treatment maneuvers may be warranted. Some of these maneuvers are relatively easy to perform, while others are harder. Patient-specific factors (e.g., obesity, arthritis and other motion-limiting disorders) may make execution of a maneuver more difficult. These limitations were partly what drove development of mechanical chairs for treatment of BPPV.
Several custom-built chairs were described in research settings:
- Furman and colleagues (Furman, Cass, Briggs 1998) custom-built a chair for this purpose, and reported it to be “extremely efficacious” in treating patients with BPPV.
- Shan and colleagues (Shan, Peng, Wang 2015) also engineered a custom chair.
As of this writing, two mechanical chairs have received FDA approval:
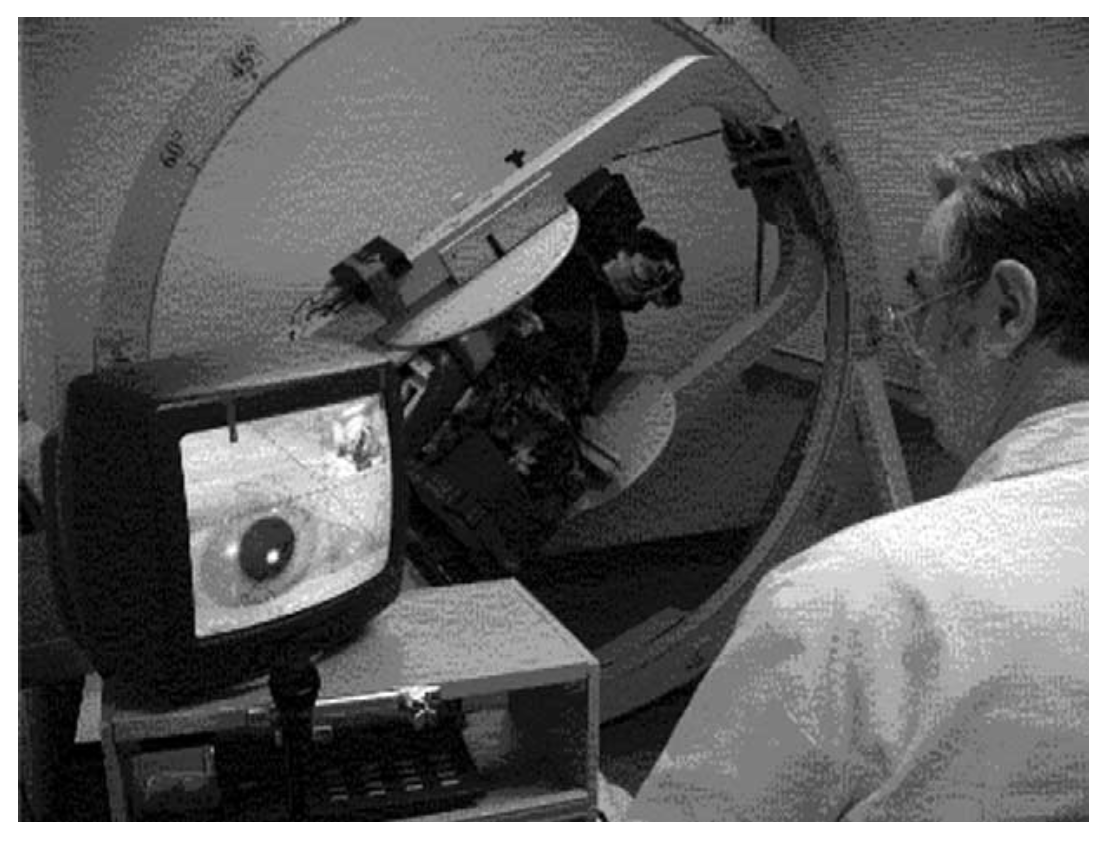
- The first commercially available mechanical chair in the US was the Epley Omniax® (Nakayama and Epley 2005), which received FDA approval on 6/20/2008 (device K071973), and was manufactured by Vesticon (Portland, Oregon). This device is no longer produced.
- The TRV Chair® was developed by Dr. Thomas Richard-Vitton (Richard-Vitton et al. 2005) and received FDA approval on 5/27/2020 (device K192652). It is distributed in the US by Interacoustics, which took over manufacturing of the device in 2016.
The Figures below show the Epley Omniax and TRV Chair.
 |
 |
Several mechanical chairs have not yet received FDA approval, including:
- The Rotundum® positioning chair (Prolim Engineering, Küsnacht, Switzerland) (Bech, Staffe, Hougaard 2023; Hougaard et al. 2022; Pedersen et al. 2020). This device is currently being studied in a clinical trial, suggesting that the manufacturer will eventually seek FDA approval.
- The Automated Mechanical Repositioning Treatment® (Byrons Medical Science and Technique, Jinan, China) (Liu et al. 2017; Zhang and Zhu 2023).
Relevance in otoneurology
The literature on the topic of mechanical chairs in the diagnosis and management of BPPV is still emerging. Some of it pertains to the diagnostic capabilities, more pertains to treatment outcomes.
Diagnostic value of mechanical chairs
Some research has explored the diagnostic accuracy of mechanical chairs.
Lechner and colleagues (Lechner et al. 2014) reported the Epley Omniax to be effective at detecting nystagmus associated with horizontal canal BPPV.
Bech and colleagues (Bech, Staffe, Hougaard 2023) found mechanical chairs (coupled with video Frenzel oculography) are more sensitive in the diagnosis of BPPV.
One rationale offered for the superior diagnostic accuracy is that during the treatment of BPPV it can be informative to observe the patient’s eye movements during each of the positions of a maneuver. While it is true that such observations are helpful, we would argue that this superior observation capability is attributable to the infrared video oculography with which the mechanical chairs are equipped, not to the mechanical chairs themselves.
Treatment by mechanical chairs is similar to manual therapy
Shan and colleagues (Shan, Peng, Wang 2015) used a custom-engineered mechanical chair with computer-controlled maneuvers and reported that, “Computer-controlled CRP [canalith repositioning maneuver] is effective for the treatment of posterior canal BPPV, with a success rate similar to those treated with the Epley maneuver, and is safe and easy to perform on patients.”
Schuricht and Hougaard (Schuricht and Hougaard 2022) compared treatment of BPPV by manual maneuvers versus the TRV Chair in a prospective trial and found no statistically significant differences in treatment outcome. In other words, treatment with the TRV Chair is not inferior to manual therapy for treatment of BPPV.
Treatment by mechanical chairs may be superior to manual therapy
West and colleagues (West et al. 2016) conducted a retrospective chart review of 150 consecutive cases of patients with “refractory vertigo” and concluded that, “The EO [Epley Omniax] and TRV [Chair] are highly valuable assets in diagnosis and management of BPPV of particularly complex and refractory cases. However, further validation is anticipated through controlled clinical trials.”
A systematic review noted that mechanical chairs may be more effective for the less common forms of BPPV (Abdulovski and Klokker 2021).
Tan and colleagues (Tan et al. 2014) studied 165 patients with unilateral posterior canal BPPV and randomly assigned them to manual therapy or treatment in the TRV Chair. They reported that, “Treatment efficacy of patients in the TRV group was significantly better than that of patients in the CRP group 1 week after the first treatment. The number of treatment sessions needed for successful repositioning was significantly lower in the TRV group than in the CRP group at 4 weeks and 3 months after the first treatment.”
Wang and colleagues (Wang et al. 2014) studied 208 BPPV patients treated in the TRV Chair and reported, “No one appeared to have otolithic debris relocated into another canal in the repositioning maneuvers” (in other words, no canal conversions occurred), and rather grandly concluded that “The results of repositioning are perfect using mechanical assistance maneuvers.”
West and colleagues (West et al. 2019) conducted a prospective observational cohort study of questionnaire-based outcome measures in BPPV patients treated in the TRV Chair and concluded that, “Patients with refractory BPPV improved significantly by reposition chair management according to all subjective outcomes. Thus, the reposition device could significantly reduce disease burden in the group of patients with BPPV who failed to respond to conventional management.”
Papers regarding both diagnosis and treatment
Power and colleagues (Power, Murray, Szmulewicz 2019) retrospectively studied 216 BPPV patients treated with the Epley Omniax. They report this method to have diagnostic and therapeutic advantages.
Pedersen and colleagues studied 81 BPPV patients treated with the TRV Chair. They reported this treatment to be “very successful in the diagnostics and treatment of patients with retractable [probably sic for ‘intractable’] and atypical BPPV” (Pedersen et al. 2020).
Overall
Some literature emphasizes the superior accuracy of mechanical chairs in the diagnosis of BPPV, but most of the literature focuses more on treatment outcomes. Most, though not all, of the literature suggests that treatment outcomes using mechanical chairs are superior to manual therapy. Some of that literature emphasizes the greater utility in cases of BPPV affecting canals other than the posterior canal, or in cases that have been refractory to standard treatment by manual therapy.
We see several plausible physical advantages to the use of mechanical chairs.
- The mechanical chairs enable a patient to maintain a neutral position, as if seated. This avoids uncomfortable positions of the head with respect to the shoulders.
- The mechanical chairs may make it easier to treat patients with obesity or limitations of motion (arthritis, spasticity, etc.).
- The mechanical chairs enable positioning of the head with respect to gravity in ways that for some patients would otherwise be difficult to achieve (such as being truly upside-down).
- Because of the relative ease in positioning the patient, mechanical chairs may enable greater consistency in performance of the maneuvers, avoiding reported variability in regular bedside canalith repositioning techniques (Bhandari et al. 2023), though whether this would have any substantial effect on the efficacy of maneuvers is unclear (Chowsilpa et al. 2025).
As far as treatment outcomes are concerned, we agree with the a systematic review that concluded while mechanical chairs seem to be promising, more randomized controlled trials are needed (Abdulovski and Klokker 2021).
References
Abdulovski S, Klokker M (2021) Repositioning Chairs in the Diagnosis and Treatment of Benign Paroxysmal Positional Vertigo – A Systematic Review. J Int Adv Otol 17: 353-360. doi: 10.5152/iao.2021.9434
Bhandari R, Bhandari A, Kingma H, Berg RV (2023) Large Variability of Head Angulation During the Epley Maneuver: Use of a Head-Mounted Guidance System with Visual Feedback to Improve Outcomes. J Int Adv Otol 19: 234-241. doi: 10.5152/iao.2023.22969
Bech MW, Staffe AT, Hougaard DD (2023) A mechanical rotation chair provides superior diagnostics of benign paroxysmal positional vertigo. Front Neurol 14: 1040701. doi: 10.3389/fneur.2023.1040701
Chowsilpa S, Chawachat J, Hansudewechakul N, Isaradisaikul SK, Hanprasertpong C (2025) Comparative Effectiveness of the Exact versus Estimated Angle of Head Position in the Epley Maneuver: A Randomized Controlled Trial. Audiol Neurootol 30: 272-281. doi: 10.1159/000543528
Furman JM, Cass SP, Briggs BC (1998) Treatment of benign positional vertigo using heels-over-head rotation. Ann Otol Rhinol Laryngol 107: 1046-53. doi: 10.1177/000348949810701209
Hougaard DD, Valsted SH, Bruun NH, Bech MW, Talebnasab MH (2022) Seven years of experience with treatment of benign paroxysmal positional vertigo with a mechanical rotational chair. Front Neurol 13: 981216. doi: 10.3389/fneur.2022.981216
Lechner C, Taylor RL, Todd C, Macdougall H, Yavor R, Halmagyi GM, Welgampola MS (2014) Causes and characteristics of horizontal positional nystagmus. J Neurol 261: 1009-17. doi: 10.1007/s00415-013-7223-5
Liu X, Treister R, Yan Y, Wang H, Li X (2017) Automated Mechanical Repositioning Treatment for Posterior Canal Benign Paroxysmal Positional Vertigo: A Single-Center Experience and Literature Review. Eur Neurol 78: 240-246. doi: 10.1159/000480429
Nakayama M, Epley JM (2005) BPPV and variants: improved treatment results with automated, nystagmus-based repositioning. Otolaryngol Head Neck Surg 133: 107-12. doi: 10.1016/j.otohns.2005.03.027
Pedersen MF, Eriksen HH, Kjaersgaard JB, Abrahamsen ER, Hougaard DD (2020) Treatment of Benign Paroxysmal Positional Vertigo with the TRV Reposition Chair. J Int Adv Otol 16: 176-182. doi: 10.5152/iao.2020.6320
Power L, Murray K, Szmulewicz D (2019) Early experience with a multi-axial, whole body positioning system in the treatment of Benign Paroxysmal Positional Vertigo (BPPV). J Clin Neurosci 61: 186-188. doi: 10.1016/j.jocn.2018.10.039
Richard-Vitton T, Seidermann L, Fraget P, Mouillet J, Astier P, Chays A (2005) [Benign positional vertigo, an armchair for diagnosis and for treatment: description and significance]. Rev Laryngol Otol Rhinol (Bord) 126: 249-51.
Schuricht A, Hougaard DD (2022) Is a Mechanical Rotational Chair Superior to Manual Treatment Maneuvers on an Examination Bed in the Treatment of Benign Paroxysmal Positional Vertigo? Otol Neurotol 43: e235-e242. doi: 10.1097/MAO.0000000000003380
Shan X, Peng X, Wang E (2015) Efficacy of computer-controlled repositioning procedure for benign paroxysmal positional vertigo. Laryngoscope 125: 715-9. doi: 10.1002/lary.24961
Tan J, Yu D, Feng Y, Song Q, You J, Shi H, Yin S (2014) Comparative study of the efficacy of the canalith repositioning procedure versus the vertigo treatment and rehabilitation chair. Acta Otolaryngol 134: 704-8. doi: 10.3109/00016489.2014.899711
Wang J, Chi FL, Jia XH, Tian L, Richard-Vitton T (2014) Does benign paroxysmal positional vertigo explain age and gender variation in patients with vertigo by mechanical assistance maneuvers? Neurol Sci 35: 1731-6. doi: 10.1007/s10072-014-1822-5
West N, Bloch SL, Moller MN, Hansen S, Klokker M (2019) Reposition Chair Treatment Improves Subjective Outcomes in Refractory Benign Paroxysmal Positional Vertigo. J Int Adv Otol 15: 146-150. doi: 10.5152/iao.2019.5659
West N, Hansen S, Moller MN, Bloch SL, Klokker M (2016) Repositioning chairs in benign paroxysmal positional vertigo: implications and clinical outcome. Eur Arch Otorhinolaryngol 273: 573-80. doi: 10.1007/s00405-015-3583-z
Zhang H, Zhu M (2023) Mechanical rotational chair-assisted multiple canalith repositioning procedures for benign paroxysmal positional vertigo: enhanced vertigo relief, comparable adverse effects, and decreased incidence of residual dizziness. Front Neurol 14: 1226138. doi: 10.3389/fneur.2023.1226138
![]()