By Marcello Cherchi, MD PhD
For patients
A cochlear implant (CI) is a tiny machine that a surgeon installs beneath the skin just behind the ear, which has wires that send electrical signals to the hearing part of the inner ear, and can restore hearing in people with certain kinds of deafness. In some patients, cochlear implants can cause disequilibrium, so if you are having this symptom, let your doctor know. Sometimes they will want to check some tests of inner ear balance function or suggest that you try vestibular rehabilitation therapy.
For clinicians
Overview
A cochlear implant (CI) transduces sound into electrical signals that are delivered directly to the spiral ganglion cells in the cochlea, bypassing any malfunctioning structures or cells in the external ear, middle ear and most of the inner ear. The invasive nature of this device appears to increase the risk of vestibular dysfunction, probably through several distinct mechanisms. Such complications overall seem to be lower in children than in adults. Undertaking a screening otovestibular workup is medically reasonable in a CI patient complaining of disequilibrium. Depending on the underlying mechanism of this symptom, vestibular rehabilitation therapy may be appropriate.
Introduction
In 1961 Dr. William House and Dr. John Doyle successfully placed the first single-channel electrode cochlear implant into a human patient that transduced sound waves into an electrical signal delivered by an electrode through the round window directly to the cochlea (Mudry and Mills 2013). At the time this was an astounding prosthetic accomplishment, and over the next decades there were significant advances in this technology (Hainarosie et al. 2014). In the United States, the Food and Drug Administration approved cochlear implants for adults in 1984 and for children in 1990.
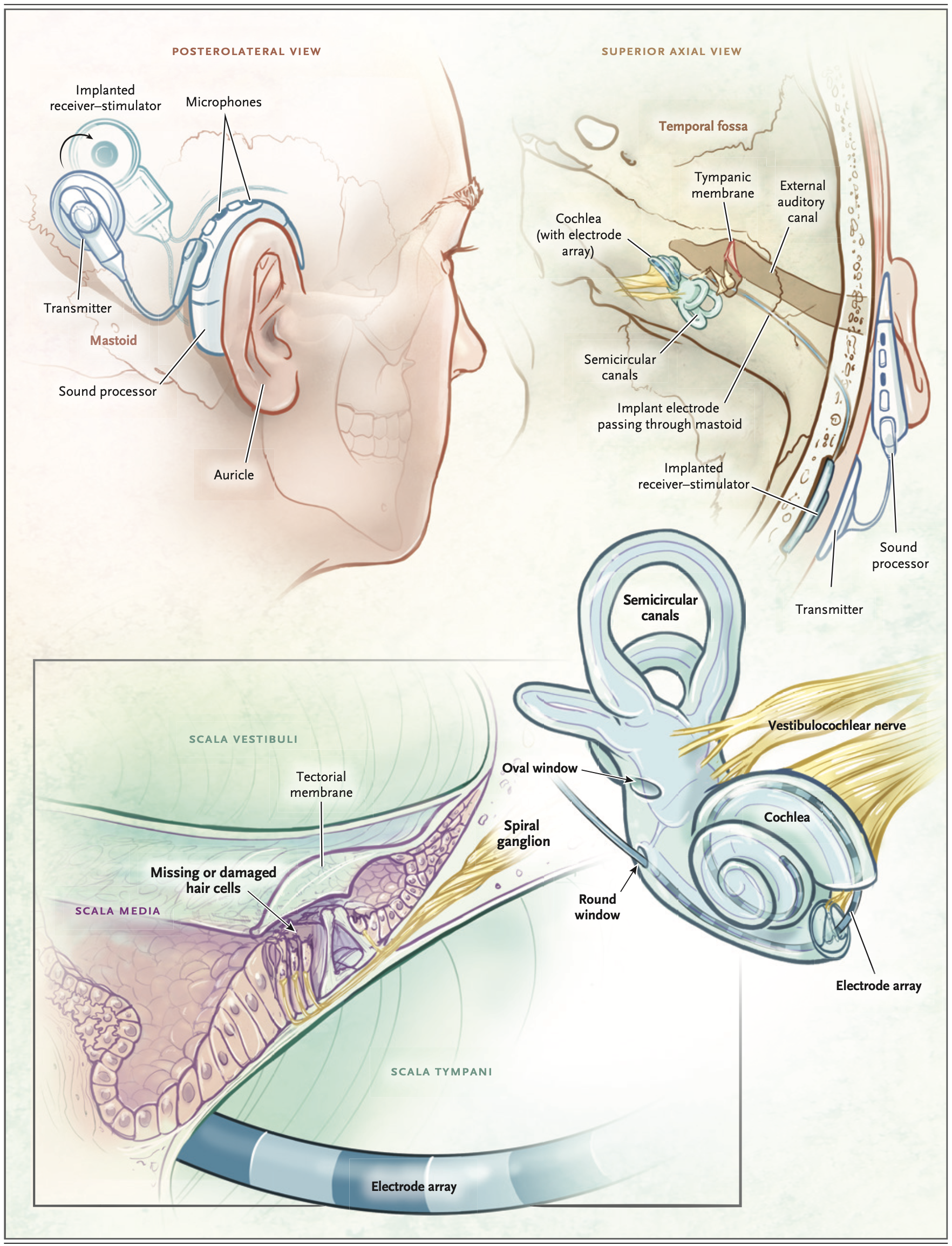
Of cochlear implants today, “virtually all commercially available devices share a similar design: the external component contains a microphone, battery, sound processor, and transmitting coil, and the internal component includes a radiofrequency receiver coil, microprocessor-based stimulator, and multichannel electrode” (Carlson 2020).
The Figure below, from Carlson (Carlson 2020), displays a schematic of cochlear implant disposition.
A cochlear implant is usually activated (“turned on”) 2 – 4 weeks after implantation (Carlson 2020).
Epidemiology
As of 2020 it was estimated that about 1.2 million adults in the United States suffered from severe to profound hearing loss (Carlson 2020) and may be candidates for cochlear implantation, yet it has also been estimated that fewer than 6% of these individuals receive this treatment (Sorkin 2013).
Pathophysiological mechanism of disease
A cochlear implant delivers electrical stimulation directly to spiral ganglion cells of the distal cochlear nerve, thereby bypassing dysfunctional or dead type 1 cochlear hair cells (Carlson 2020). However, in order for an electrode to reach this location it must pierce the round window and thus violate the labyrinth. One can imagine that such disruption could result in unintended dysfunction in other areas of the labyrinth, such as the end organelles that mediate vestibular function.
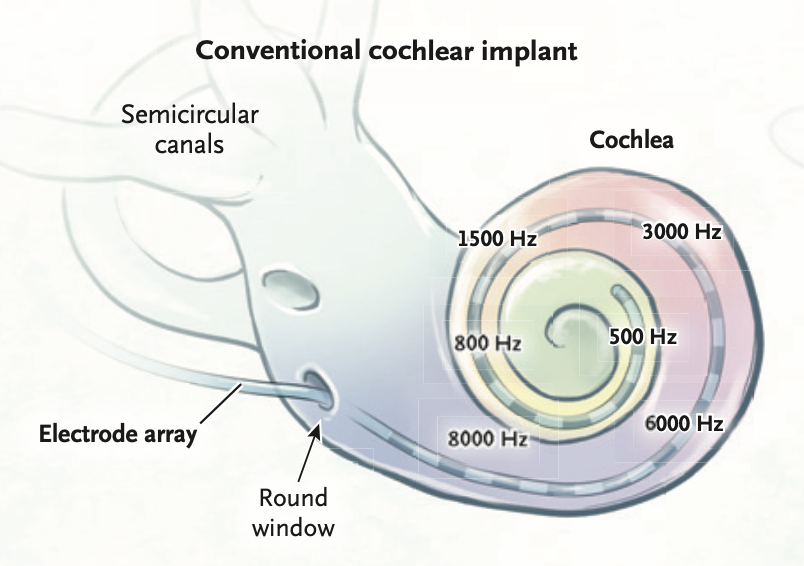
The Figure below, from Carlson (Carlson 2020), is a schematic of a cochlear implant’s multichannel electrode passing through the round window, and its disposition within the cochlea.
Some individuals experience disequilibrium at some interval after cochlear implantation, and these patients may be referred to otoneurology with the implicit clinical query of assessing whether there is vestibular dysfunction and, if so, whether that dysfunction is the result of cochlear implantation itself.
There are several potential mechanisms by which cochlear implantation may induce vestibular dysfunction.
Occasionally CI patients are diagnosed with benign paroxysmal positional vertigo (BPPV) (Di Girolamo et al. 1999; Rah et al. 2016; Viccaro et al. 2007). This usually occurs ipsilateral to the cochlear implant, but occasionally occurs contralaterally (Viccaro et al. 2007); since BPPV is common, it is possible that chance occurrence of BPPV happens to overlap with cochlear implantation — in other words, this may be coincidental rather than causal; however, the fact that BPPV occurs much more commonly ipsilateral to the CI implicates a causal relationship.
Another potential mechanism is that the electrode (intended to stimulate the acoustic component of the vestibulocochlear nerve) unintentionally stimulates a vestibular end-organ (Coordes et al. 2012), or the presence of the electrode predisposes to ephaptic transmission from auditory to vestibular axons. Some authors conclude that unintentional stimulation of vestibular end-organs is rare (Bance et al. 1998).
There are reports of impaired vestibular function (such as caloric weakness) both ipsilateral and contralateral to a cochlear implant (Bonucci et al. 2008). Since CI necessarily violates the labyrinth (and thus makes labyrinthine proteins accessible to the immune system), it is conceivable that the contralateral deterioration of vestibular function is due to sympathetic ear disease.
Clinical presentation: disequilibrium
The onset of disequilibrium in CI patients may occur between implantation and activation, or may occur only following activation (Filipo et al. 2006). The latency from cochlear implantation to onset of disequilibrium is variable, ranging from as short as “directly post-operatively” (Krause et al. 2009b) or “soon after surgery” (Kubo et al. 2001) or within 2 days (Filipo et al. 2006), to as long as 377 days (Fina et al. 2003).
Reported rates of disequilibrium following CI are quite variable.
- Carlson (Carlson 2020) reviewed several studies and reported that 102/4664 (2.2%) of CI patients experience “persistent vestibular symptoms.”
- Farinetti and colleagues (Farinetti et al. 2014) studied 168 adult CI patients and 235 pediatric CI patients and reported that 13/168 (7.7%) of adults and 2/235 (0.8%) of children experienced disequilibrium post-implantation, amounting to a pooled rate of 15/403 (3.7%).
- Rah and colleagues (Rah et al. 2016) studied 62 CI patients and reported that 18 (27%) experienced postoperative disequilibrium.
- Fina and colleagues (Fina et al. 2003) report disequilibrium in 29/75 (39%) of CI patients. They noted that 4 patients experienced a vertiginous attack less than 24 hours after implantation surgery, whereas “the majority, 25 patients, experienced delayed, episodic onset of vertigo,” and that “the median (interquartile range) time of delayed onset was 74 (26 – 377) days after implantation.”
- Krause and colleagues (Krause et al. 2009a; Krause et al. 2009b) reported on 47 adult CI patients and found that 21 (45%) experienced disequilibrium after CI.
- Zawawi and colleagues (Zawawi et al. 2014) studied 122 patients and reported that 27% complained of disequilibrium preoperatively, and 45.9% complained of disequilibrium postoperatively.
- Kubo and colleagues (Kubo et al. 2001) reported on 94 consecutive adult CI patients and found that 46 (49%) experienced disequilibrium after implantation.
- Steenerson and colleagues (Steenerson et al. 2001) reported that 35/47 (74%) of adult CI patients experienced “vertigo or imbalance.”
In short, reported rates of disequilibrium overall following CI vary by over an order of magnitude.
As far as the symptom of disequilibrium following cochlear implantation is concerned, it is notable that the data from Farinetti and colleagues (Farinetti et al. 2014) suggest that this complication is more common in adults (7.7%) than in children (0.8%) by almost an order of magnitude.
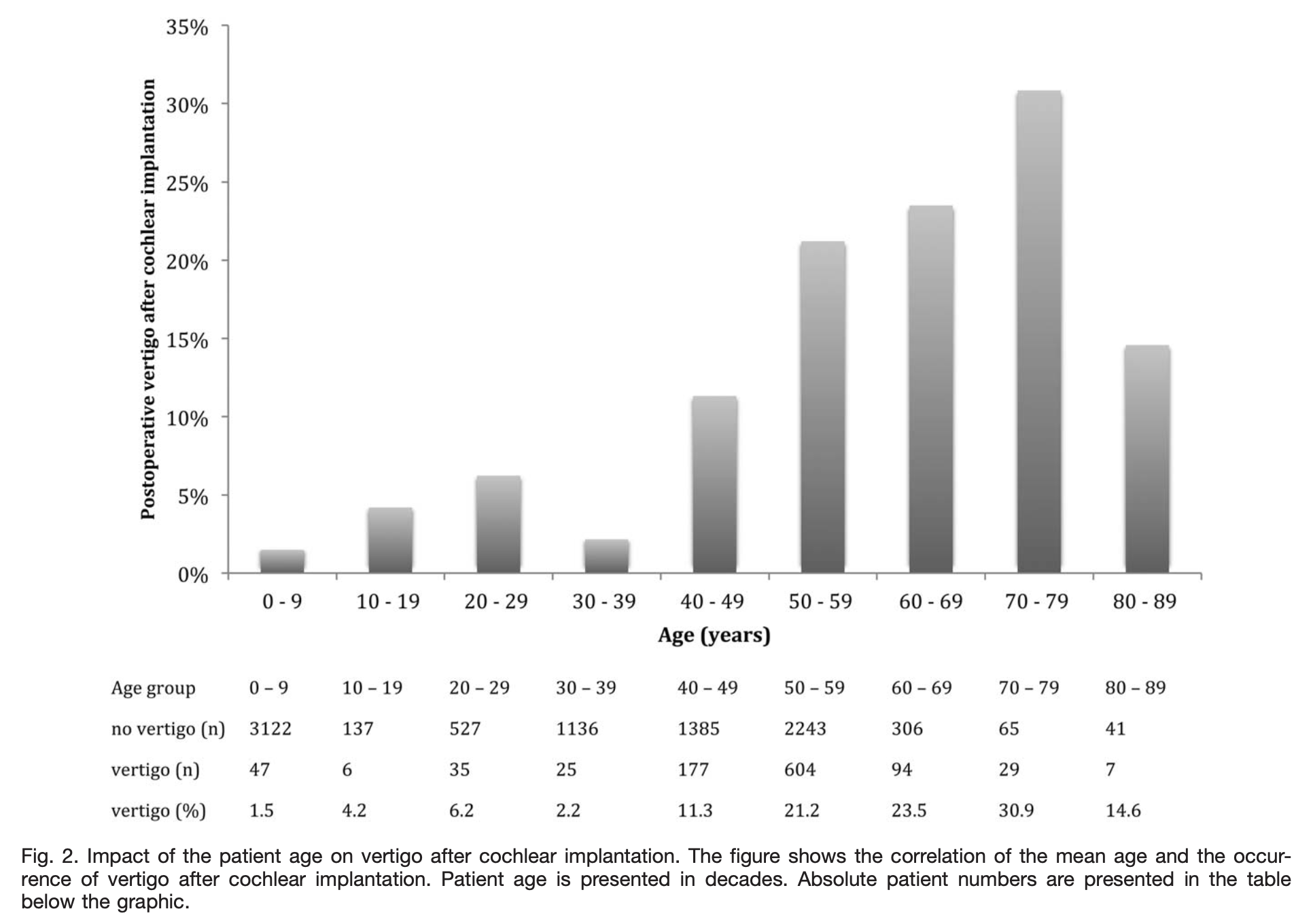
A more granular analysis of post-implantation disequilibrium by age may be found in a meta-analysis of CI studies that reported a clear relationship between patient age at the time of implantation and the occurrence of disequilibrium, with a peak in the 8th decade. The Figure below, from Hansel and colleagues (Hansel et al. 2018), demonstrates this.
The duration of vestibular symptoms following cochlear implantation is similarly variable, ranging from brief to “permanent.” Katsiari and colleagues (Katsiari et al. 2013) studied 20 unilateral CI patients and concluded that, “permanent vertigo was rare.” Kubo and colleagues (Kubo et al. 2001) reported on 94 consecutive adult CI patients and found that, “Dizziness of the continuous type, lasting more than 6 months, was a complaint in only two patients” (2%).
Clinical presentation: tinnitus
Farinetti and colleagues (Farinetti et al. 2014) note that some CI patients with pre-implantation tinnitus experience worsening of that tinnitus post-implantation, while others who had no tinnitus pre-implantation develop new tinnitus post-implantation. Tinnitus, similar to vestibular symptoms, appears to be more frequent post-implantation complication in adults than in children; Farinetti and colleagues reported that 14/168 (8.3%) adults and 2/235 (0.9%) children experienced new or worsening of tinnitus following cochlear implantation.
Ocular motor examination
Hempel and colleagues (Hempel et al. 2004) described a CI patient with postoperative pneumolabyrinth who under Frenzel glasses had spontaneous and inducible nystagmus.
Testing: vestibular
Some literature reviews conclude that CI overall has a deleterious effect on the results of instrumented vestibular testing (Hansel et al. 2018), while other reviews emphasize significant variability in the literature (Gerdsen et al. 2022).
Some literature has reported measurable vestibular dysfunction in all vestibular end organelles following CI (Kwok et al. 2022; Vaz et al. 2022).
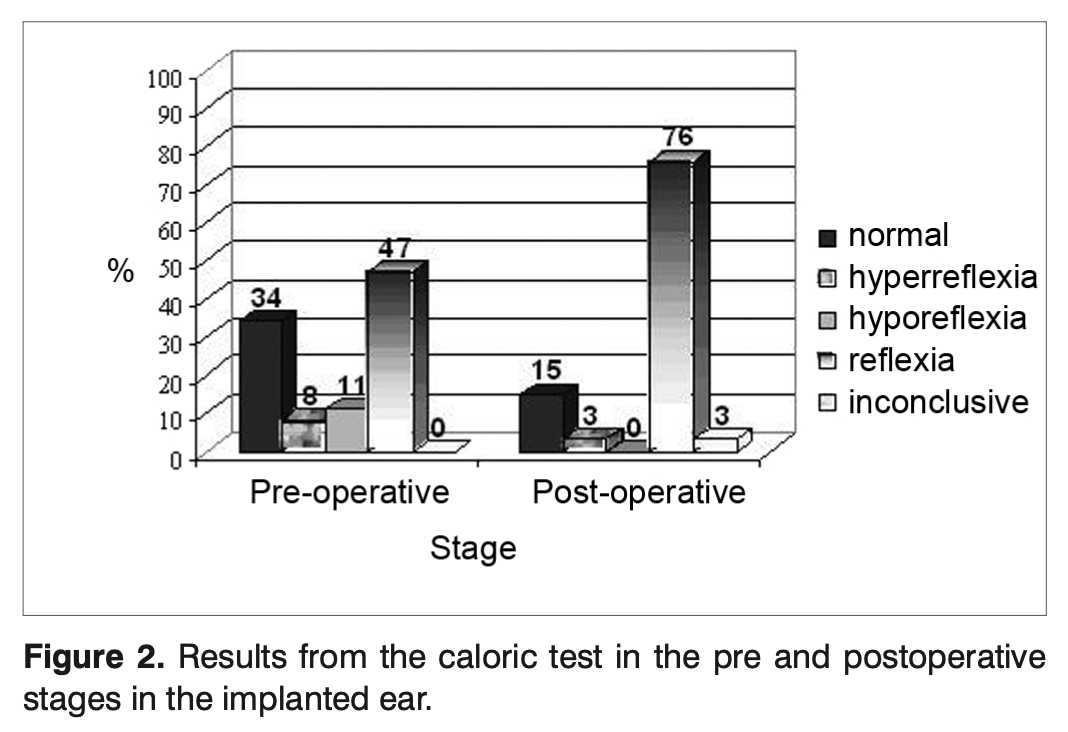
Bonucci and colleagues studied 31 CI patients and reported caloric weakness not only ipsilateral, but also contralateral to a cochlear implant (Bonucci et al. 2008).
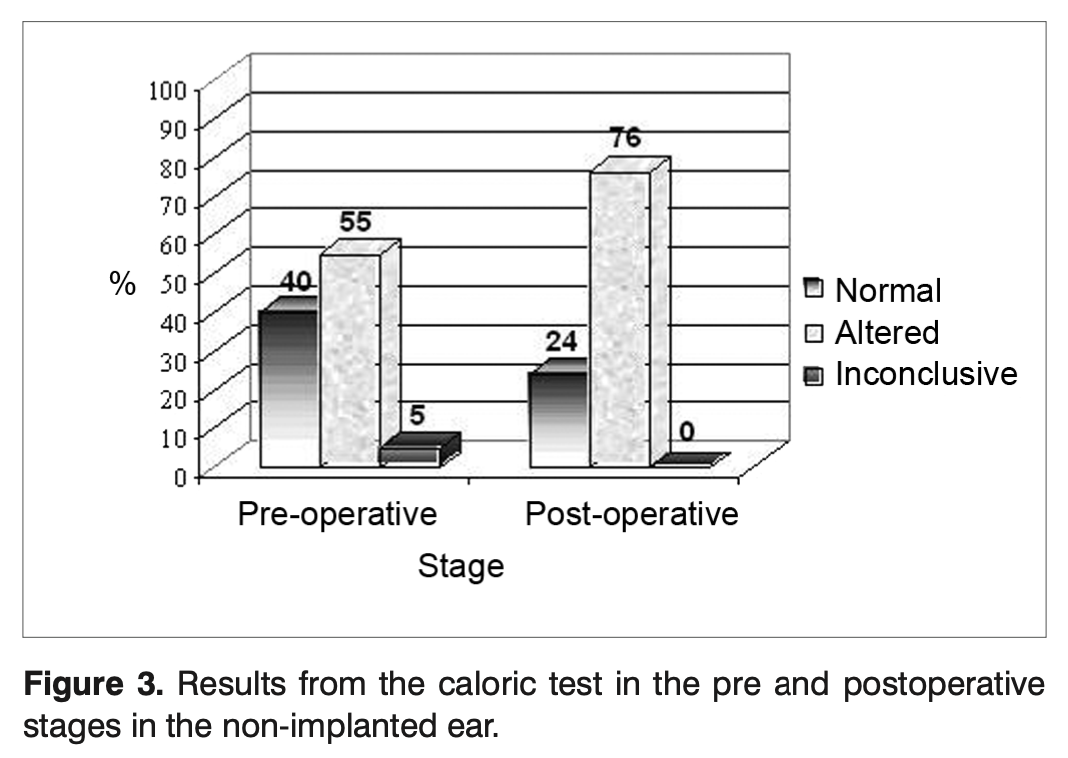
The Figures below from Bonucci and colleagues (Bonucci et al. 2008) show caloric status preoperatively and postoperatively in implanted and unimplanted ears. In implanted ears there was preoperative caloric weakness in 58% (11% hyporeflexic, 47% areflexic) and postoperative caloric weakness in 76% (76% areflexic). In unimplanted ears there was preoperative caloric weakness in 55% (5% hyporeflexic, 50% areflexic) and postoperative caloric weakness in 73% (73% areflexic).
 |
 |
Krause and Louza (Krause et al. 2009a) prospectively studied 47 adult CI patients and reported that, “Thirty-two percent of patients had a substantially reduced hSCC [horizontal semicircular canal] function after CI. Responses of caloric irrigation showed a significant worsening postoperatively in the CI ears.”
Chen and colleagues (Chen et al. 2016) studied 34 patients before and after cochlear implantation; all 34 had pre- and postoperative cervical vestibular evoked myogenic potentials and ocular vestibular evoked myogenic potentials, and 29 of the patients also had caloric testing. They concluded that, “Cochlear implantation can damage the function of the horizontal semicircular canal and utricle, as well as the function of the saccule.”
Krause and Louza (Krause et al. 2010) prospectively studied 32 unilateral CI patients aged 15 – 83 years and found that, “Cochlear implantation represents a significant risk factor for horizontal semicircular canal impairment (p<0.001) and sacculus impairment (p=0.047) in the implanted ear.”
Katsiari and colleagues (Katsiari et al. 2013) studied 20 unilateral CI patients and reported that a “statistically significant difference was found in the percentages of canal paresis (p=0.01) and the percentages of [c]VEMP waveform absence (p=0.002) between the repeated measurements in the implanted side.”
Vibert and colleagues (Vibert et al. 2001) assessed utricular function using the OVAR (off vertical axis rotation) protocol rotatory chair and found no effect of CI on this aspect of otolith function.
Regarding video head impulse testing (vHIT), several studies failed to find any effect of CI on the results (Ajalloueyan et al. 2017; Guan et al. 2021), while others reported that CI adversely affects vHIT results (Kwok et al. 2022).
Batuk and colleagues (Batuk et al. 2025) compared performance on computerized dynamic posturography (CDP) in 26 cochlear implant patients against 26 age-matched controls, and reported that on sensory organization testing, cochlear implant patients had statistically significantly worse composite scores, and worse performance on conditions 2- 6.
Several research groups who studied CI patients observed a poor correlation between vestibular symptoms and vestibular test results (Colin et al. 2018; Krause et al. 2009a; Stultiens et al. 2020).
Imaging
Imaging of vestibularly-relevant structures is difficult in CI patients because the implants and their electrodes contain metal, and thus will introduce significant artifact into CT and MRI images.
Histopathology
Tien and Linthicum (Tien and Linthicum 2002) studied 11 pairs of temporal bones from patients with unilateral CI and reported that, “In the vestibular end organs of the 6 implanted ears that we believe may have shown damage from implantation, no exclusive or dominant findings could be identified. However, the saccule is more susceptible to damage than the utricle or semicircular canals because of its proximity to the pathway of the inserted electrodes, regardless of whether the round window or cochleostomy approach is used.”
Handzel and colleagues (Handzel et al. 2006) studied 19 temporal bones of CI patients and reported that, “Cochlear implantation does not cause deafferentation of the peripheral vestibular system. Cochlear hydrops accompanied by saccular collapse is common.”
Differential diagnosis
Cochlear implantation is still relatively uncommonly performed, so when an auditory or vestibular symptom appears post-implantation, it is reasonable to undertake a screening assessment for common causes of such symptoms that may be occurring independently of implantation, rather than simply assuming that those symptoms are attributable to the cochlear implant.
As far as workup of vestibular symptoms is concerned, we generally start with bedside infrared video oculography (to assess, for example, for benign paroxysmal positional vertigo). Thereafter, we agree with the view that, “Ideally, all the five vestibular sensors should be tested” (Abouzayd et al. 2017), and thus we will usually also consider checking vestibular tests that can detect lateralizing abnormalities, such as cervical vestibular evoked myogenic potentials, ocular vestibular evoked myogenic potentials, video head impulse testing and videonystagmography with caloric testing. As discussed earlier, it is unsurprising to find vestibular deficits on an implanted ear, but finding such deficits in an unimplanted ear raises suspicion for an independently occurring pathology (such as vestibular neuritis).
Failure of cochlear implantation
“Failure” of cochlear implantation is defined in different ways by different studies. Layfield and colleagues (Layfield et al. 2021) conducted a literature review and concluded that the overall CI failure rate was 5.5%.
Liu and colleagues (Liu et al. 2023) conducted a meta-analysis of 144 articles covering 85,851 initial cochlear implantations and 4,276 cochlear reimplantations, and calculated a pooled rate of cochlear reimplantation of 4.7%.
Treatment and prognosis
Regarding vestibular symptoms thought to be attributable to a cochlear implant, Steenerson and colleagues (Steenerson et al. 2001) reported that post-CI disequilibrium responds favorably to vestibular rehabilitation therapy.
In patients experiencing disequilibrium after CI, some surgeons advocate checking whether the electrode needs to be resealed (Karimi et al. 2017).
References
Abouzayd M, Smith PF, Moreau S, Hitier M (2017) What vestibular tests to choose in symptomatic patients after a cochlear implant? A systematic review and meta-analysis. Eur Arch Otorhinolaryngol 274: 53-63. doi: 10.1007/s00405-016-4007-4
Ajalloueyan M, Saeedi M, Sadeghi M, Zamiri Abdollahi F (2017) The effects of cochlear implantation on vestibular function in 1-4 years old children. Int J Pediatr Otorhinolaryngol 94: 100-103. doi: 10.1016/j.ijporl.2017.01.019
Bance ML, O’Driscoll M, Giles E, Ramsden RT (1998) Vestibular stimulation by multichannel cochlear implants. Laryngoscope 108: 291-4. doi: 10.1097/00005537-199802000-00025
Batuk IT, Orhan E, Batuk MO, Aksoy S (2025) Vestibular function and balance stability in adult cochlear implant users: a comparative study of sensory organization, visual acuity, and gaze stabilization. Eur Arch Otorhinolaryngol 282: 5201-5207. doi: 10.1007/s00405-025-09576-6
Bonucci AS, Costa Filho OA, Mariotto LD, Amantini RC, Alvarenga Kde F (2008) Vestibular function in cochlear implant users. Braz J Otorhinolaryngol 74: 273-8.
Carlson ML (2020) Cochlear Implantation in Adults. N Engl J Med 382: 1531-1542. doi: 10.1056/NEJMra1904407
Chen X, Chen X, Zhang F, Qin Z (2016) Influence of cochlear implantation on vestibular function. Acta Otolaryngol 136: 655-9. doi: 10.3109/00016489.2016.1154186
Colin V, Bertholon P, Roy S, Karkas A (2018) Impact of cochlear implantation on peripheral vestibular function in adults. Eur Ann Otorhinolaryngol Head Neck Dis 135: 417-420. doi: 10.1016/j.anorl.2018.10.007
Coordes A, Basta D, Gotze R, Scholz S, Seidl RO, Ernst A, Todt I (2012) Sound-induced vertigo after cochlear implantation. Otol Neurotol 33: 335-42. doi: 10.1097/MAO.0b013e318245cee3
Di Girolamo S, Fetoni AR, Di Nardo W, Paludetti G (1999) An unusual complication of cochlear implant: benign paroxysmal positional vertigo. J Laryngol Otol 113: 922-3. doi: 10.1017/s0022215100145608
Farinetti A, Ben Gharbia D, Mancini J, Roman S, Nicollas R, Triglia JM (2014) Cochlear implant complications in 403 patients: comparative study of adults and children and review of the literature. Eur Ann Otorhinolaryngol Head Neck Dis 131: 177-82. doi: 10.1016/j.anorl.2013.05.005
Filipo R, Patrizi M, La Gamma R, D’Elia C, La Rosa G, Barbara M (2006) Vestibular impairment and cochlear implantation. Acta Otolaryngol 126: 1266-74. doi: 10.1080/00016480600678789
Fina M, Skinner M, Goebel JA, Piccirillo JF, Neely JG, Black O (2003) Vestibular dysfunction after cochlear implantation. Otol Neurotol 24: 234-42; discussion 242.
Gerdsen M, Jorissen C, Pustjens D, Hof J, Rompaey V, Berg R, Widdershoven J (2022) Effect of cochlear implantation on vestibular function in children: A scoping review. Frontiers in Pediatrics 10: 949730. doi: 10.3389/fped.2022.949730
Guan R, Wang Y, Wu S, Zhang B, Sun J, Guo X, Sun J (2021) Vestibular Function in Children and Adults Before and After Unilateral or Sequential Bilateral Cochlear Implantation. Front Neurol 12: 675502. doi: 10.3389/fneur.2021.675502
Hainarosie M, Zainea V, Hainarosie R (2014) The evolution of cochlear implant technology and its clinical relevance. J Med Life 7 Spec No. 2: 1-4.
Handzel O, Burgess BJ, Nadol JB, Jr. (2006) Histopathology of the peripheral vestibular system after cochlear implantation in the human. Otol Neurotol 27: 57-64. doi: 10.1097/01.mao.0000188658.36327.8f
Hansel T, Gauger U, Bernhard N, Behzadi N, Romo Ventura ME, Hofmann V, Olze H, Knopke S, Todt I, Coordes A (2018) Meta-analysis of subjective complaints of vertigo and vestibular tests after cochlear implantation. Laryngoscope. doi: 10.1002/lary.27071
Hempel JM, Jager L, Baumann U, Krause E, Rasp G (2004) Labyrinth dysfunction 8 months after cochlear implantation: a case report. Otol Neurotol 25: 727-9. doi: 10.1097/00129492-200409000-00014
Karimi D, Mittmann P, Ernst A, Todt I (2017) Surgical treatment of vertigo in cochlear implantees by electrode resealing. Acta Otolaryngol 137: 1031-1034. doi: 10.1080/00016489.2017.1331045
Katsiari E, Balatsouras DG, Sengas J, Riga M, Korres GS, Xenelis J (2013) Influence of cochlear implantation on the vestibular function. Eur Arch Otorhinolaryngol 270: 489-95. doi: 10.1007/s00405-012-1950-6
Krause E, Louza JP, Hempel JM, Wechtenbruch J, Rader T, Gurkov R (2009a) Effect of cochlear implantation on horizontal semicircular canal function. Eur Arch Otorhinolaryngol 266: 811-7. doi: 10.1007/s00405-008-0815-5
Krause E, Louza JP, Wechtenbruch J, Gurkov R (2010) Influence of cochlear implantation on peripheral vestibular receptor function. Otolaryngol Head Neck Surg 142: 809-13. doi: 10.1016/j.otohns.2010.01.017
Krause E, Louza JP, Wechtenbruch J, Hempel JM, Rader T, Gurkov R (2009b) Incidence and quality of vertigo symptoms after cochlear implantation. J Laryngol Otol 123: 278-82. doi: 10.1017/S002221510800296X
Kubo T, Yamamoto K, Iwaki T, Doi K, Tamura M (2001) Different forms of dizziness occurring after cochlear implant. Eur Arch Otorhinolaryngol 258: 9-12.
Kwok BYC, Rosengren SM, Kong JHK, Birman CS, Hoskisson E, Young AS, Argaet EC, Fratturo L, Rivas C, Greenberg SL, Saxby AJ, Welgampola MS (2022) Impact of Cochlear Implantation on Canal and Otolith Function. Otol Neurotol 43: 304-312. doi: 10.1097/MAO.0000000000003459
Layfield E, Hwa TP, Naples J, Maina I, Brant JA, Eliades SJ, Bigelow DC, Ruckenstein MJ (2021) Failure and Revision Surgery After Cochlear Implantation in the Adult Population: A 10-year Single-institution Retrospective and Systematic Review of the Literature. Otol Neurotol 42: 408-413. doi: 10.1097/MAO.0000000000002940
Liu H, Yao X, Kong W, Zhang L, Si J, Ding X, Zheng Y, Zhao Y (2023) Cochlear Reimplantation Rate and Cause: a 22-Year, Single-Center Experience, and a Meta-Analysis and Systematic Review. Ear Hear 44: 43-52. doi: 10.1097/AUD.0000000000001266
Mudry A, Mills M (2013) The early history of the cochlear implant: a retrospective. JAMA Otolaryngol Head Neck Surg 139: 446-53. doi: 10.1001/jamaoto.2013.293
Rah YC, Park JH, Park JH, Choi BY, Koo JW (2016) Dizziness and vestibular function before and after cochlear implantation. Eur Arch Otorhinolaryngol 273: 3615-3621. doi: 10.1007/s00405-016-3988-3
Sorkin DL (2013) Cochlear implantation in the world’s largest medical device market: utilization and awareness of cochlear implants in the United States. Cochlear Implants Int 14 Suppl 1: S4-12. doi: 10.1179/1467010013z.00000000076
Steenerson RL, Cronin GW, Gary LB (2001) Vertigo after cochlear implantation. Otol Neurotol 22: 842-3.
Stultiens JJA, Kieft HW, Mylanus EAM, Pennings RJE, Terwoert L, Beynon AJ (2020) Impact of cochlear implantation on the function of the three semicircular canals. Int J Audiol 59: 843-849. doi: 10.1080/14992027.2020.1768310
Tien HC, Linthicum FH, Jr. (2002) Histopathologic changes in the vestibule after cochlear implantation. Otolaryngol Head Neck Surg 127: 260-4. doi: 10.1067/mhn.2002.128555
Vaz FC, Petrus L, Martins WR, Silva IMC, Lima JAO, Santos N, Turri-Silva N, Bahmad F, Jr. (2022) The effect of cochlear implant surgery on vestibular function in adults: A meta-analysis study. Front Neurol 13: 947589. doi: 10.3389/fneur.2022.947589
Vibert D, Hausler R, Kompis M, Vischer M (2001) Vestibular function in patients with cochlear implantation. Acta Otolaryngol Suppl 545: 29-34.
Viccaro M, Mancini P, La Gamma R, De Seta E, Covelli E, Filipo R (2007) Positional vertigo and cochlear implantation. Otol Neurotol 28: 764-7. doi: 10.1097/MAO.0b013e318064e8d4
Zawawi F, Alobaid F, Leroux T, Zeitouni AG (2014) Patients reported outcome post-cochlear implantation: how severe is their dizziness? J Otolaryngol Head Neck Surg 43: 49. doi: 10.1186/s40463-014-0049-z
![]()