By Marcello Cherchi, MD PhD
For patients
Rebound nystagmus (RN) is a pattern of eye movements that can happen in some brain diseases. If your doctor sees rebound nystagmus during your physical examination, they may want to check several tests.
For clinicians
Overview
Rebound nystagmus (RN) is an ocular motor finding in which, after a patient has maintained prolonged horizontal eccentric gaze and then returns to primary position of gaze, there is transient jerk nystagmus whose slow phase is in the direction of the previous horizontal eccentric gaze, and the fast phase is back towards primary position. RN often occurs in association with horizontal gaze evoked nystagmus. The mechanism of RN is unknown, but it is thought to reflect a deficit in the neural integrator required for gaze holding. RN can occur in the context of many diseases affecting the cerebellum and brainstem. Treatment and prognosis depends on the underlying cause.
Introduction
Rebound nystagmus (RN) is “a transient nystagmus that occurs when the eyes return to straight ahead position following a period of prolonged eccentric gaze holding” (Otero-Millan et al. 2019) in which “Quick phases of the nystagmus are away from the direction of a previously attempted eccentric gaze” (Lin and Young 1999), and thus the “slow phases of rebound nystagmus are in the direction of prior eccentric gaze” (Otero-Millan et al. 2019).
Epidemiology
Over the course of 7 years (1991 – 1998), Lin and Young (Lin and Young 1999) studied 9156 patients who presented to a single hospital “with vertigo or tinnitus,” and reported that 10 (0.1%) “showed rebound nystagmus by ENG” (electronystagmography). This sample is somewhat odd in that patients with “vertigo or tinnitus” were included — so presumably some patients had only auditory symptoms and no vestibular symptoms. Nevertheless, Lin and Young are suggesting that rebound nystagmus is uncommon.
Pathophysiological mechanism of disease
Rebound nystagmus “is thought to be related to the function of the oculomotor neural integrator — the circuit that ensures accurate gaze holding after any eye movement — but the exact mechanism of rebound nystagmus is unknown” (Otero-Millan et al. 2019).
Shallo-Hoffman and colleagues (Shallo-Hoffmann et al. 1990) comment that:
“End-point nystagmus (EPN) [their term for horizontal gaze-evoked nystagmus] is evoked by far lateral gaze… Rebound nystagmus (RN) consists of a reversal of nystagmus that is evoked by a gaze shift to the primary position (PP) after a period of lateral gaze. The direction of RN is always the reverse of the EPN” (Shallo-Hoffmann et al. 1990).
In other words, horizontal gaze-evoked nystagmus and rebound nystagmus co-occur.
Bogli and colleagues (Bogli et al. 2021) hypothesize that both gaze-evoked nystagmus and rebound nystagmus reflect similar underlying “cerebellar loss of function.” Specifically:
“A brain stem/cerebellar neural integrator enables stable eccentric gaze. Cerebellar loss-of-function can cause an inability to maintain gaze eccentrically (gaze-evoked nystagmus). Moreover, after returning gaze to straight ahead, the eyes may drift toward the prior eye position (rebound nystagmus). Typically, gaze-evoked nystagmus decays during continuously held eccentric gaze. We hypothesized this adaptive behavior to be prerequisite for rebound nystagmus and thus predicted a correlation between the velocity decay of gaze-evoked nystagmus and the initial velocity of rebound nystagmus” (Bogli et al. 2021).
Bogli and colleagues studied 11 patients with cerebellar degeneration and reported a correlation, concluding that, “Rebound nystagmus can be explained as gaze-evoked nystagmus relative to a set point (position with least eye drift) away from straight-ahead eye position” (Bogli et al. 2021).
Shallo-Hoffmann and colleagues state that, “The cause of RN [rebound nystagmus] is a velocity bias of the neural integrator evolved during long eccentric gaze” (Shallo-Hoffmann et al. 1990).
Note that not all rebound nystagmus is pathological; “After eccentric gaze, healthy subjects also show rebound nystagmus when fixation is removed” (Otero-Millan et al. 2019).
Clinical presentation
The clinical presentation depends on the underlying disease with which rebound nystagmus is associated.
Physical examination
Rebound nystagmus can occur in association with diseases of the cerebellum and brainstem. In some cases there will be corresponding signs on physical examination (such as appendicular cerebellar dysmetria), while in other cases the general neurological examination may be unrevealing.
Ocular motor examination
Rebound nystagmus is usually difficult to observe on face-to-face ocular motor examination.
Testing: instrumented ocular motor examination
Rebound nystagmus can be subtle, so examination under infrared video oculography is often revealing.
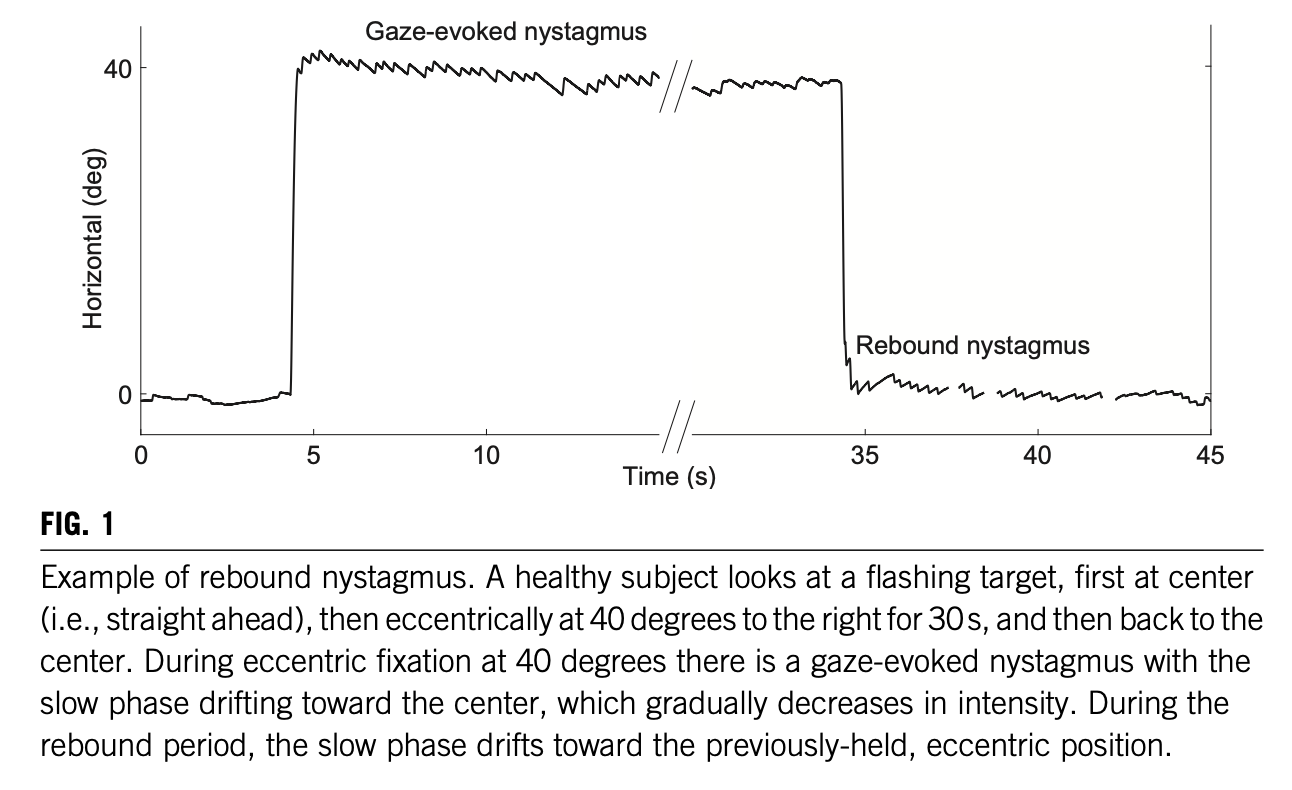
The Figure below, from Otero-Millan and colleagues (Otero-Millan et al. 2019), illustrates rebound nystagmus.
Imaging
If the clinical scenario merits imaging, the area in question (posterior fossa) is usually best visualized by MRI.
Differential diagnosis
Lin and Young suggest that, “Rebound nystagmus implies a lesion in the cerebellum or brainstem for which MRI examination is 100% sensitive” (Lin and Young 1999).
Rebound nystagmus has been reported in association with a range of posterior fossa lesions.
Hood and colleagues (Hood et al. 1973) studied 25 patients exhibiting rebound nystagmus and reported the following pathologies:
- Cerebellar degeneration or atrophy
- Cerebellar lesion, unspecified
- Demyelinating disease (location unspecified)
- Foramen magnum lesions
- Posterior fossa tumors
- Vascular lesions of the posterior fossa
- Drug intoxication
- Undetermined posterior fossa lesion with familial history
Lin and Young (Lin and Young 1999) studied 10 patients exhibiting rebound nystagmus and reported the following pathologies:
- Cerebellopontine angle schwannoma (three cases)
- Cerebellopontine angle meningioma
- Cerebellar anaplastic astrocytoma
- Brainstem astrocytoma
- Brainstem lymphoma
- Cerebellar hemorrhage
- Dissecting aneurysm of vertebral artery
- Dolichoectasia of vertebrobasilar artery
Scattered case reports also describe rebound nystagmus occurring in various additional diseases, often involving cerebellar pathways. For example, Bondar and colleagues report rebound nystagmus in a patient with olivopontocerebellar atrophy (Bondar et al. 1984).
Lin and Young state that rebound nystagmus, “has a certain lateralizing value, with its direction away from the lesioned side” (Lin and Young 1999). Similarly, Morales-Garcia and colleagues report, “In three out of four patients with unilateral lesions rebound nystagmus was ipsilateral with respect to the side of the lesion” (Morales-Garcia et al. 1978). This differs from our own experience, in which rebound nystagmus does not reliably lateralize the lesion.
Treatment and prognosis
Treatment and prognosis of a patient exhibiting rebound nystagmus will depend on the underlying disease.
References
Bogli SY, Straumann D, Schuknecht B, Bertolini G, Tarnutzer AA (2021) Cerebellar Rebound Nystagmus Explained as Gaze-Evoked Nystagmus Relative to an Eccentric Set Point: Implications for the Clinical Examination. Cerebellum 20: 751-759. doi: 10.1007/s12311-020-01118-6
Bondar RL, Sharpe JA, Lewis AJ (1984) Rebound nystagmus in olivocerebellar atrophy: a clinicopathological correlation. Ann Neurol 15: 474-7. doi: 10.1002/ana.410150512
Hood JD, Kayan A, Leech J (1973) Rebound nystagmus. Brain 96: 507-26. doi: 10.1093/brain/96.3.507
Lin CY, Young YH (1999) Clinical significance of rebound nystagmus. Laryngoscope 109: 1803-5. doi: 10.1097/00005537-199911000-00015
Morales-Garcia C, Cardenas JL, Arriagada C, Otte J (1978) Clinical significance of rebound nystagmus in neuro-otological diagnosis. Ann Otol Rhinol Laryngol 87: 238-42. doi: 10.1177/000348947808700216
Otero-Millan J, Colpak AI, Kheradmand A, Zee DS (2019) Rebound nystagmus, a window into the oculomotor integrator. Prog Brain Res 249: 197-209. doi: 10.1016/bs.pbr.2019.04.040
Shallo-Hoffmann J, Schwarze H, Simonsz HJ, Muhlendyck H (1990) A reexamination of end-point and rebound nystagmus in normals. Invest Ophthalmol Vis Sci 31: 388-92.
![]()