By Marcello Cherchi, MD PhD
For patients
Oculopalatal tremor (OPT) usually occurs several months after an acute lesion (typically a stroke) in the brainstem or cerebellum. Symptoms can consist of a rhythmic clicking sound in one or both ears (due to a continuous involuntary tremor of the soft palate), and a disturbance of vision or equilibrium (due to a continuous involuntary movement of the eyes). Brain MRI shows abnormal signal in a brainstem structure called the inferior olive. Treatment with gabapentin is usually well tolerated and sometimes helpful.
For clinicians
Overview
Oculopalatal tremor (OPT) usually begins several months after suffering an acute insult (typically an ischemic or hemorrhagic stroke) in the brainstem or cerebellum interrupting a circuit known as the triangle of Guillain-Mollaret. Symptoms include chronic rhythmic clicking tinnitus (from the palatal tremor) and a disturbance of vision or equilibrium (from the pendular nystagmus). Examination shows a 2 – 3 Hz palatal tremor with synchronous pendular nystagmus (with some combination of vertical, torsional and horizontal components) that can be conjugate or dissociated. Brain MRI shows T2/FLAIR signal abnormality in the inferior olives that reflects hypertrophic degeneration. Small trials of several drugs find some efficacy of gabapentin and memantine, with gabapentin being the better tolerated medication.
Introduction
“Palatal myoclonus” was the term originally given to a 2 – 3 Hz oscillatory rising and lowering of the soft palate that persists during sleep. Since the movement has a sinusoidal pattern rather than a “spike” pattern, this phenomenon was eventually instead designated “palatal tremor.” Dr. Adam Politzer is usually credited with having published the first description (Politzer 1878). With few exceptions (Diaz et al. 2024; Tatum et al. 1991), palatal myoclonus usually results from a brainstem lesion interrupting the triangle of Guillian-Mollaret (to be discussed below).
The movement of the soft palate is often synchronous with an oculomotor abnormality, and in such cases it is designated “oculopalatal tremor” (OPT). Spencer (Oppenheim 1887) is usually credited with having published the first description of this. OPT is an, “acquired pendular nystagmus synchronous with a tremor of the soft palate/pharynx” (Jun 2016), with the abnormal pharyngeal muscular activity “affecting muscles derived from branchial arches including muscles of the palate, pharynx,” and sometimes “head, neck and diaphragm” (Borruat 2013).
Demographics
Oculopalatal tremor is rare but the precise prevalence and incidence are unknown. A study of 82 patients by Jang and Borruat (Jang and Borruat 2014) reported that the average age of onset was 54 years with a male predominance.
Clinical presentation
Most cases of OPT occur after an acute lesion of the brainstem or cerebellum, typically an ischemic or hemorrhagic stroke. A patient’s original symptoms may improve, but within several months they develop rhythmic clicking tinnitus (from the palatal tremor) and a disturbance of vision or equilibrium (from the pendular nystagmus). These symptoms are chronic.
Pathophysiology
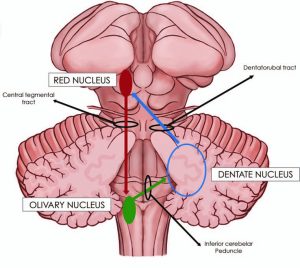
OPT “result[s] from the interruption of the dentato-rubro-olivary pathway” (Jun 2016) which runs from (1) the red nucleus in the midbrain, via the central tegmental tract to (2) the inferior olivary nucleus in the medulla, via the inferior cerebellar peduncle to (3) the dentate nucleus in the cerebellum, via the dentatorubral tract back up to the red nucleus. This pathway was originally described by Dr. George Charles Guillain and Dr. Pierre Mollaret (Giuillain and Mollaret 1931), and is thus usually referred to as the triangle of Guillain-Mollaret.
Anatomically OPT is associated with hypertrophy of the inferior olive (Jun 2016), originally described by Oppenheim (Oppenheim 1887). The histopathological change is one of “trans-synaptic degeneration” in the inferior olive, and is “attributed to increased water content and gliosis. Pathologically, hypertrophy of the olive corresponds to enlargement of both neurons and astrocytes and the neurons become vacuolated” (Jun 2016).
Control systems analysis has led to models of specific cellular mechanisms likely responsible for the oscillatory activity (Hong, Leigh et al. 2008), though some studies suggest that more than one mechanism may be at play (Shaikh, Hong et al. 2010). Oddly, an FDG-PET scan study of six patients with unilateral OPT “had hypometabolism in ipsilesional pontine tegmentum and hypermetabolism in contralesional thalamus” (Moon, Cho et al. 2008).
The inferior olivary hypertrophic degeneration is generally unilateral, and it is “ipsilateral to the [causative] lesion if the lesion is in the brain stem or contralateral to the lesion if the lesion is in the cerebellum” (Jun 2016).
Rare cases of bilateral involvement have been documented (Behzadi, Fiester et al. 2021).
Etiology
OPT is the delayed result of a discrete lesion anywhere along the pathways of the Guillain-Mollaret triangle, typically in the brainstem or cerebellum (Borruat 2013). Most cases of OPT are the delayed result of an acute lesion; it has been estimated that about 80% of cases are due to a brainstem vascular lesion (Jang and Borruat 2014), such as ischemic or hemorrhagic infarction (Alstadhaug 2007).
Less commonly, OPT occurs in the context of neoplasm. Spencer’s original description was a case of a neoplasm in a young girl (Oppenheim 1887). Occurrence with medulloblastoma has also been described (Behzadi, Fiester et al. 2021).
OPT can occur in multiple sclerosis, though its behavior appears distinct from that of other brainstem lesions in some respects (Tilikete, Jasse et al. 2011). In cases of OPT occurring in multiple sclerosis (MS) it is believed that an MS lesion has caused “instability of the neural integrator, which normally ensures steady gaze” (Shaikh, Thurtell et al. 2011).
Even less common are cases that appear to occur spontaneously (Oliveira, Negreiros Junior et al. 2003), without any detectable discrete event or lesion.
Physical examination
In a patient with OPT, examination of the oropharynx should show a fairly regular 2 – 3 Hz oscillation of the soft palate. Oculomotor examination in about 90% of cases shows prominent pendular nystagmus with vertical and torsional components (Jang and Borruat 2014) synchronous with the palatal tremor. The oropharyngeal and oculomotor components may be present to a greater or lesser degree.
The following Video from Jang and Borruat (Jang and Borruat 2013) shows these findings.
VIDEO
The nystagmus can be conjugate or dissociated. Jang and Borruat (Jang and Borruat 2014) studied 12 cases and reported that dissociated nystagmus tended to occur in unilateral lesions (with the oculomotor finding contralateral to the lesion), whereas conjugate nystagmus tended to occur with bilateral lesions. Similar patterns of conjugate versus dissociated nystagmus were described in a series of 22 patients reported by Kim and Moon (Kim, Moon et al. 2007).
The binocular oculomotor tracing in the Figure below from a patient with OPT shows pendular nystagmus that is divergent; the right eye exhibits a prominent vertical component with subtle horizontal and torsional components; in contrast the left eye shows prominent vertical and horizontal components, and a moderate torsional component (Tilikete and Desestret 2017).

The Figure below from East and Hazell (East and Hazell 1987) shows impedance tympanometry in a patient with palatal myoclonus, with spikes occurring at a frequency of about 80 per minute.
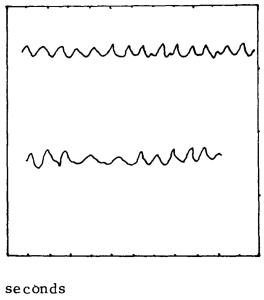
Figure : Immittance tympanometry in a patient with palatal myoclonus showing spikes occurring at a frequency of about 80 per minute (from East and Hazell 1987).
Testing
It is desirable to perform binocular oculographic studies in order to document that the eye movements are compatible with OPT. Taking a video of, or at least documenting, palatal tremor is also important.
Imaging
The inferior olivary hypertrophic degeneration of OPT is reflected radiographically on MRI by an enlarged inferior olive with abnormal T2 and FLAIR signal hyperintensity. This imaging finding “appears as early as 3 weeks after a causal event but usually 6 – 8 months and disappears by 4 years” (Jun 2016).
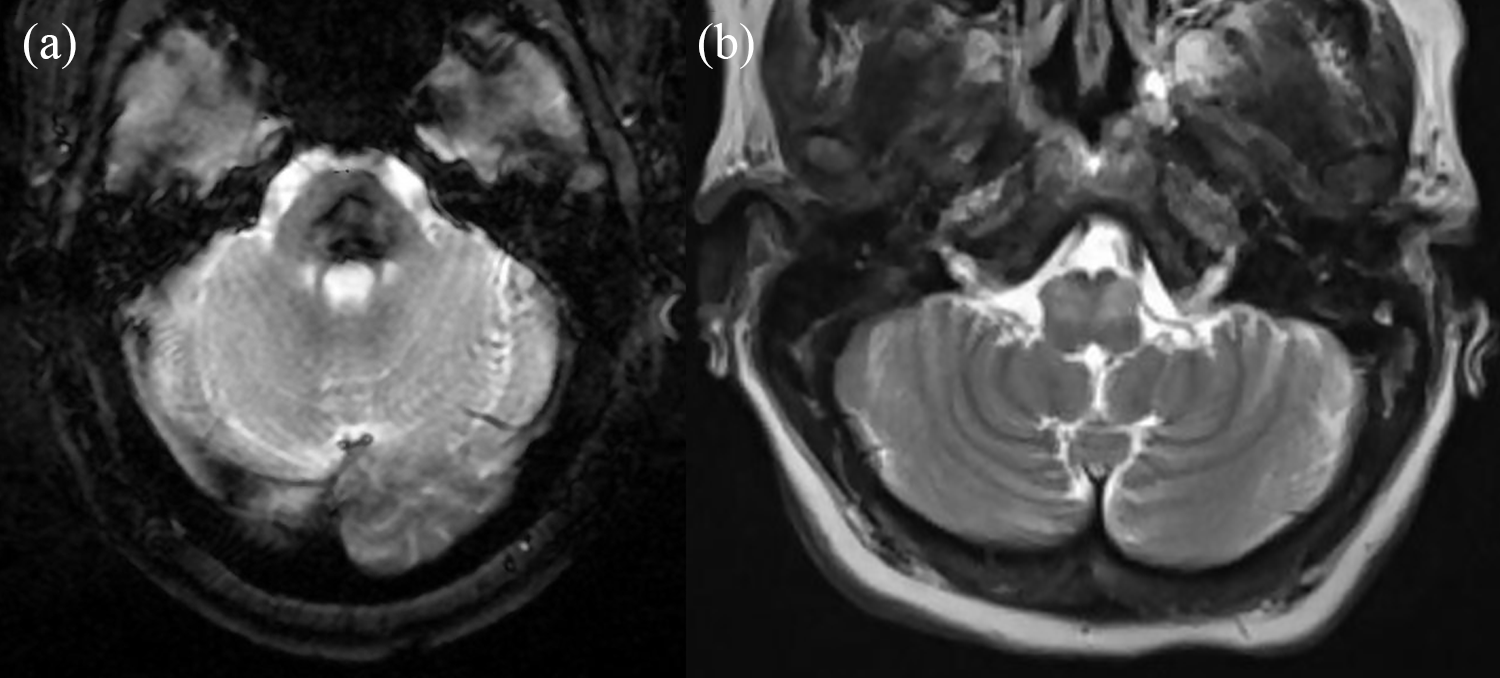
The Figure below from Jang and Borruat (Jang and Borruat 2013) shows a normal medulla in (B) compared with a medulla exhibiting left inferior olivary hypertrophy.
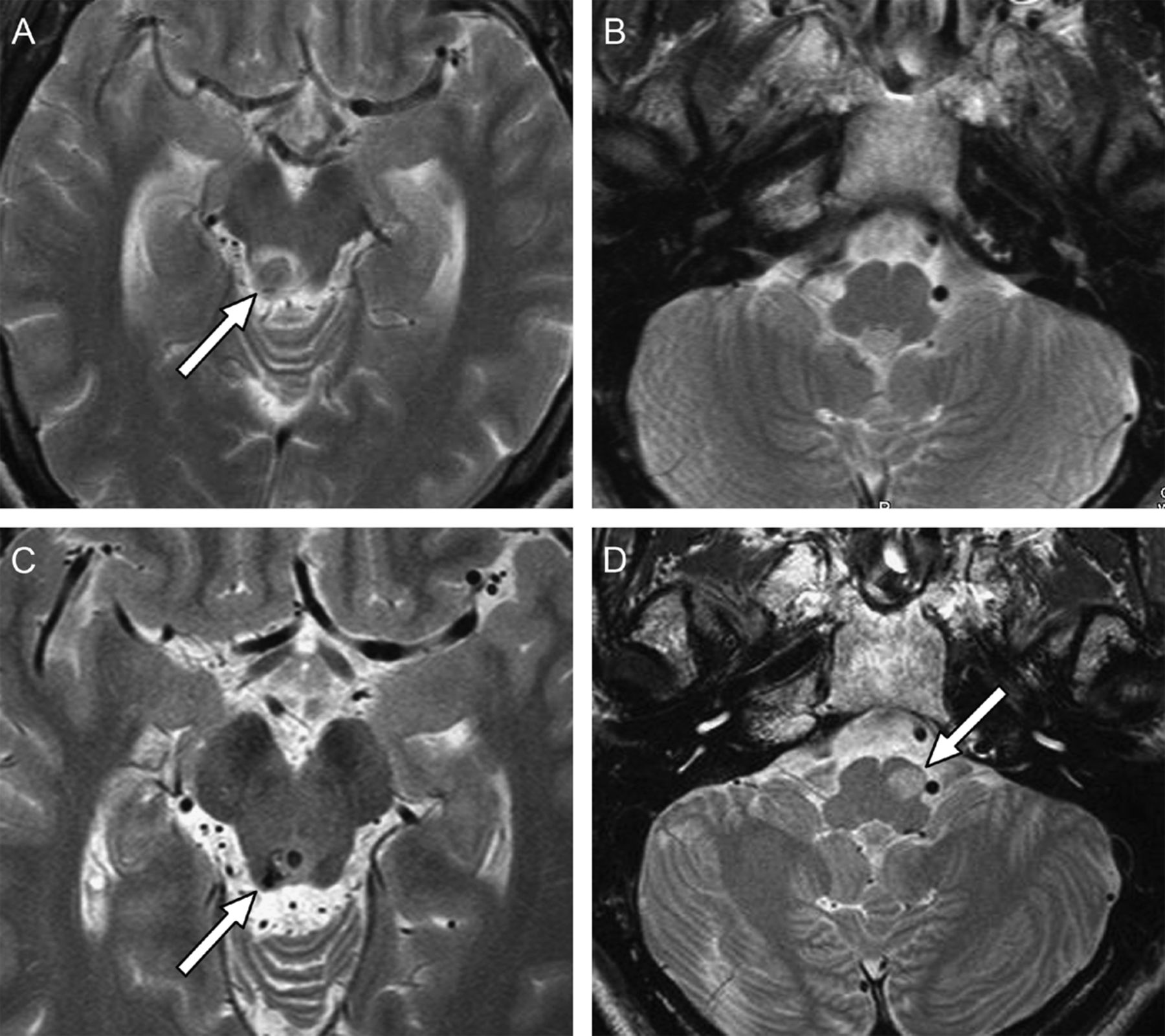
The Figure below is a rare case of bilateral inferior olivary hypertrophy reported by Behzadi et al. (Behzadi, Fiester et al. 2021)
Treatment
A study comparing the use of gabapentin and baclofen in the treatment of 21 patients with “acquired nystagmus” (including 2 patients with OPM) reported better results with gabapentin (Averbuch-Heller, Tusa et al. 1997).
One study of comparing the use of gabapentin, baclofen and memantine reported that the magnitude of the pendular nystagmus diminished with gabapentin and memantine but not with baclofen (Shaikh, Thurtell et al. 2011).
A crossover trial of gabapentin and memantine of 12 patients with acquired pendular nystagmus, including four patients with OPT following brainstem, reported improvement in nystagmus with each drug, though gabapentin was better tolerated than memantine (Thurtell, Joshi et al. 2010).
Another trial of gabapentin and memantine of 16 patients with acquired pendular nystagmus, including six patients with OPT, found that both gabapentin and memantine improved visual outcomes, but that gabapentin was better tolerated than memantine (Nerrant, Abouaf et al. 2020).
References
Averbuch-Heller L, Tusa RJ, Fuhry L, Rottach KG, Ganser GL, Heide W, Buttner U, Leigh RJ (1997) A double-blind controlled study of gabapentin and baclofen as treatment for acquired nystagmus. Ann Neurol 41: 818-25. doi: 10.1002/ana.410410620
Behzadi F, Fiester PJ, Rao D (2021) Bilateral Hypertrophic Olivary Degeneration Following Brainstem Insult: A Retrospective Review and Examination of Causative Pathology. Neurosci Insights 16: 26331055211007445. doi: 10.1177/26331055211007445
Borruat FX (2013) Oculopalatal tremor: current concepts and new observations. Curr Opin Neurol 26: 67-73. doi: 10.1097/WCO.0b013e32835c60e6
Diaz PG, Zolin AR, Tsiouris AJ, Mir S (2024) Palatal Myoclonus Due to Cortical Cavernous Malformation. Neurology 102: e209278. doi: 10.1212/WNL.0000000000209278
East CA, Hazell JW (1987) The suppression of palatal (or intra-tympanic) myoclonus by tinnitus masking devices. A preliminary report. J Laryngol Otol 101: 1230-4.
Giuillain GC, Mollaret P (1931) Deux cas de myoclonies synchrones et rythmees velo-pharyngo-laryngo-oculo-diaphragmatiques: Le probleme anatomique et phsiologique [Two cases of synchronous and rhythmical velo-pharyngo-laryngo-oculo-diaphragmatic myoclonus]. Rev Neurol 2: 545-566.
Hong S, Leigh RJ, Zee DS, Optican LM (2008) Inferior olive hypertrophy and cerebellar learning are both needed to explain ocular oscillations in oculopalatal tremor. Prog Brain Res 171: 219-26. doi: 10.1016/S0079-6123(08)00631-6
Jang L, Borruat FX (2013) Micronystagmus of oculopalatal tremor. Neurology 80: e27. doi: 10.1212/WNL.0b013e31827debc3
Jang L, Borruat FX (2014) Oculopalatal tremor: variations on a theme by Guillain and Mollaret. Eur Neurol 72: 144-9. doi: 10.1159/000360531
Jun B (2016) The Development of Hypertrophic Inferior Olivary Nucleus in Oculopalatal Tremor. Neuroophthalmology 40: 297-299. doi: 10.1080/01658107.2016.1226903
Kim JS, Moon SY, Choi KD, Kim JH, Sharpe JA (2007) Patterns of ocular oscillation in oculopalatal tremor: imaging correlations. Neurology 68: 1128-35. doi: 10.1212/01.wnl.0000258665.37827.f6
Moon SY, Cho SS, Kim YK, Kim SE, Kim JH, Kim JS (2008) Cerebral glucose metabolism in oculopalatal tremor. Eur J Neurol 15: 42-9. doi: 10.1111/j.1468-1331.2007.01997.x
Nerrant E, Abouaf L, Pollet-Villard F, Vie AL, Vukusic S, Berthiller J, Colombet B, Vighetto A, Tilikete C (2020) Gabapentin and Memantine for Treatment of Acquired Pendular Nystagmus: Effects on Visual Outcomes. J Neuroophthalmol 40: 198-206. doi: 10.1097/WNO.0000000000000807
Oliveira CA, Negreiros Junior J, Cavalcante IC, Bahmad F, Jr., Venosa AR (2003) Palatal and middle-ear myoclonus: a cause for objective tinnitus. Int Tinnitus J 9: 37-41.
Oppenheim H (1887) Über Olivendegeneration bei Atheromatose der basalen Hirnarterien. Berl Klin Wochenschr 34: 638-639.
Politzer A (1878) Lehrbuch der Ohrenheilkunde für praktische Ärtze und Studeierende. Verlag von Ferdinand Enke, Stuttgart
Shaikh AG, Hong S, Liao K, Tian J, Solomon D, Zee DS, Leigh RJ, Optican LM (2010) Oculopalatal tremor explained by a model of inferior olivary hypertrophy and cerebellar plasticity. Brain 133: 923-40. doi: 10.1093/brain/awp323
Shaikh AG, Thurtell MJ, Optican LM, Leigh RJ (2011) Pharmacological tests of hypotheses for acquired pendular nystagmus. Ann N Y Acad Sci 1233: 320-6. doi: 10.1111/j.1749-6632.2011.06118.x
Tatum WO, Sperling MR, Jacobstein JG (1991) Epileptic palatal myoclonus. Neurology 41: 1305-6. doi: 10.1212/wnl.41.8.1305
Thurtell MJ, Joshi AC, Leone AC, Tomsak RL, Kosmorsky GS, Stahl JS, Leigh RJ (2010) Crossover trial of gabapentin and memantine as treatment for acquired nystagmus. Ann Neurol 67: 676-80. doi: 10.1002/ana.21991
Tilikete C, Desestret V (2017) Hypertrophic Olivary Degeneration and Palatal or Oculopalatal Tremor. Front Neurol 8: 302. doi: 10.3389/fneur.2017.00302
Tilikete C, Jasse L, Pelisson D, Vukusic S, Durand-Dubief F, Urquizar C, Vighetto A (2011) Acquired pendular nystagmus in multiple sclerosis and oculopalatal tremor. Neurology 76: 1650-7. doi: 10.1212/WNL.0b013e318219fa9c
![]()