By Marcello Cherchi, MD PhD
For patients
Some patients with allergic symptoms also notice ear symptoms (hearing loss, tinnitus, ear fullness) and disequilibrium. The relationship between allergies and these hearing/balance symptoms is unclear. In some cases your doctor may check several tests of hearing and balance function, and if these results do not show evidence for some other disease, you may consider a trial of over-the-counter allergy medications. If that fails, then it is reasonable to consult with an allergist for more formal allergy testing and possible treatment.
For clinicians
Overview
Otoneurologists and neuro-otologists sometimes encounter patients with both allergic symptoms and otovestibular symptoms whose examinations and workups are unrevealing, but the relationship between these symptoms is unclear. Studies report that, for example, patients diagnosed with allergic rhinitis report aural pruritis, subjective hearing loss and tinnitus, and vertigo more frequently than healthy control subjects, and audiologic testing also shows a greater frequency of abnormal results compared to healthy control subjects. This area has not been studied well, and there are no guidelines on how to proceed. Practically, when we encounter patients with both allergic symptoms and otovestibular symptoms whose otovestibular workups are normal, we will often suggest a trial of over-the-counter allergy medication. If that fails, we will refer for a formal allergy consultation, with the goal of identifying whether there is a specific allergy whose treatment may be more targeted.
Introduction
The connection between allergic diatheses and otovestibular symptoms is poorly understood.
The older literature on this topic (McLaurin 1946, Floberg and Koch 1954, Strandbygaard 1955, Pisani 1958, Powers and House 1969, Wilson and Powers 1971, Clemis 1972) is characterized by limited diagnostic techniques and treatments available at that time.
Allergy is common, and otovestibular symptoms are common, so these groups of symptoms will coincide simply by chance. Whether there is a greater-than-chance overlap of these two groups of symptoms is unclear, though some literature (reviewed below) suggests that there is.
The relevance in otoneurology and neuro-otology is that it is not rare for clinicians to encounter patients with allergic symptoms and otovestibular symptoms whose examinations and workups appear entirely normal. In this circumstance it is reasonable to wonder whether there is a causative relationship (specifically, whether allergies can cause otovestibular symptoms), and whether treating for allergies might also alleviate otovestibular symptoms.
Pathophysiological mechanism of disease
Even if a greater-than-chance association can be demonstrated between allergic symptoms and otovestibular symptoms, this in itself does not explain whether there is a mechanistic relationship, much less what that relationship would be.
Dr. Jennifer Derebery and others (Derebery and Valenzuela 1992, Derebery 1997, Di Berardino, Barozzi et al. 2005, Derebery and Berliner 2007, Derebery and Berliner 2010, Banks, McGinness et al. 2012, Weinreich and Agrawal 2014) have advocated for the idea that Ménière’s disease has an allergic basis. Even if this idea proves to be correct, it would still leave open the question of the broader relationship between allergy and otovestibular disease.
Clinical presentation
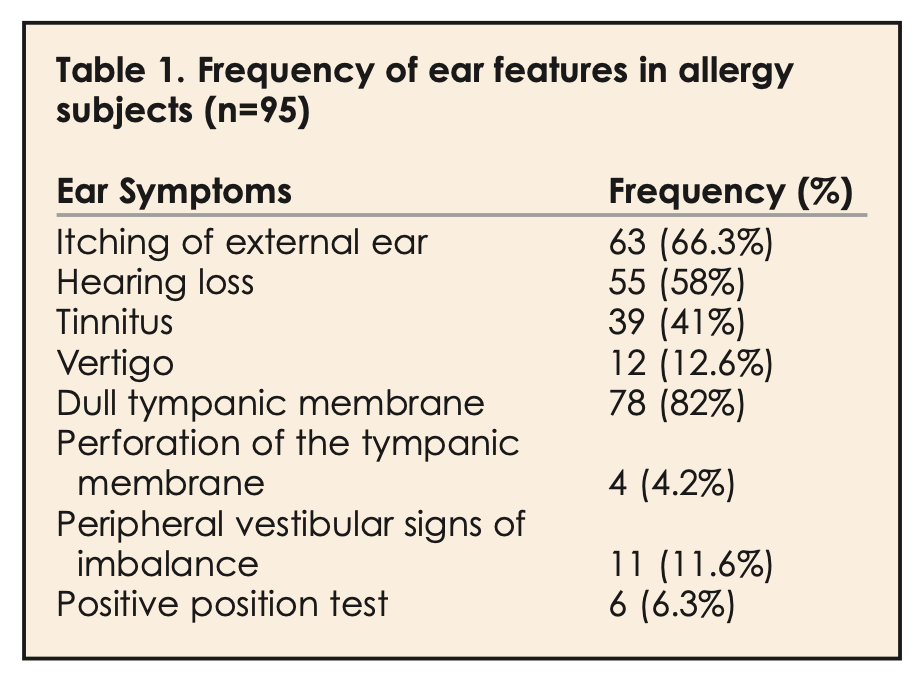
Lasisi and Abdullahi (Lasisi and Abdullahi 2008) retrospectively reviewed records of 144 patients, consisting of 71 males and 73 females, mean age of 32 years (range 2 – 80 years), all diagnosed with nasal allergy. Of these 144 patients they found that 95 (66%) complained of otovestibular symptoms. Of these 95 patients, 63 (66%) had itching of the external auditory canal, 55 (58%) complained of hearing loss, 39 (41%) complained of tinnitus and 12 (13%) complained of vertigo, as shown in the Table below.
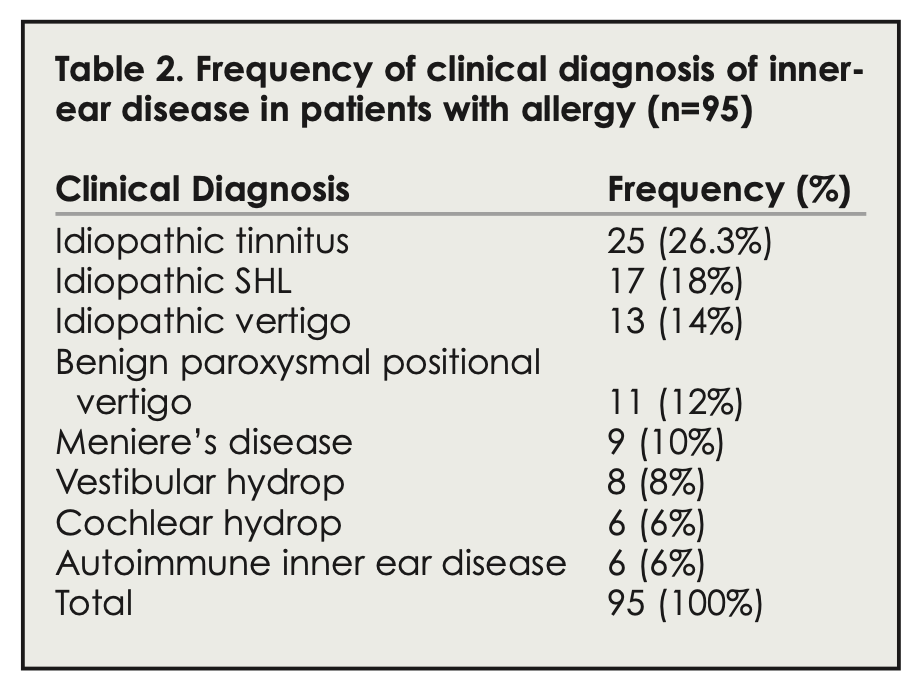
Of the 95 patients with otovestibular symptoms, the final diagnoses were as shown in the Table below.
Testing: audiologic
Lasisi and Abdullahi (Lasisi and Abdullahi 2008) reported that of 75 nasal allergy patients whose audiometry had been documented, 43 (59%) were normal (0 – 25 dB), 17 (23%) had some sensorineural hearing loss, and 13 (18%) had conductive hearing loss. Of the 17 with sensorineural hearing loss, it was mild (26 – 45 dB) in 6 (35%), moderate (46 – 60 dB) in 7 (41%) and moderate-to-severe (61 – 70 dB) in 4 (24%).
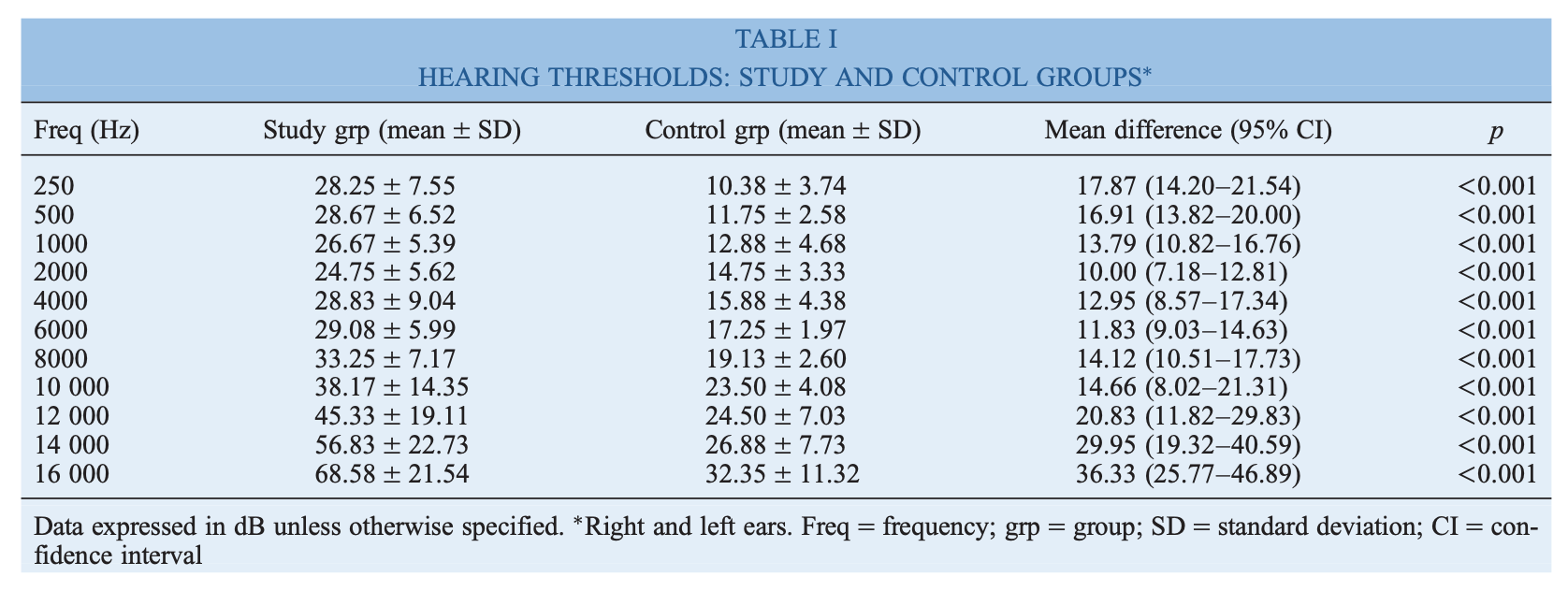
Singh and colleagues (Singh, Nagarkar et al. 2011) studied 30 patients diagnosed with allergic rhinitis, including 16 women (53%) and 14 men, with a mean age of 31 years (range 17 – 45 years), compared to 20 healthy controls. They studied pure tone audiometry, distortion product otoacoustic emissions, transient evoked otoacoustic emissions, and brainstem auditory evoked responses in all subjects.
They reported that the allergic rhinitis patients had statistically significant hearing loss at all frequencies compared to controls, as shown in the Table below.
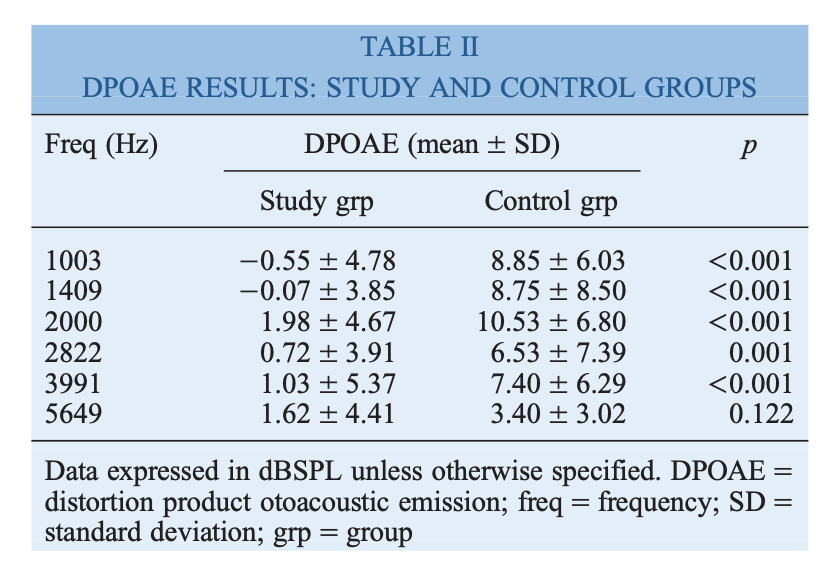
They reported that allergic rhinitis patients were statistically significantly worse than controls on distortion product otoacoustic emissions, referring at all frequencies except the highest, as shown in the Table below.
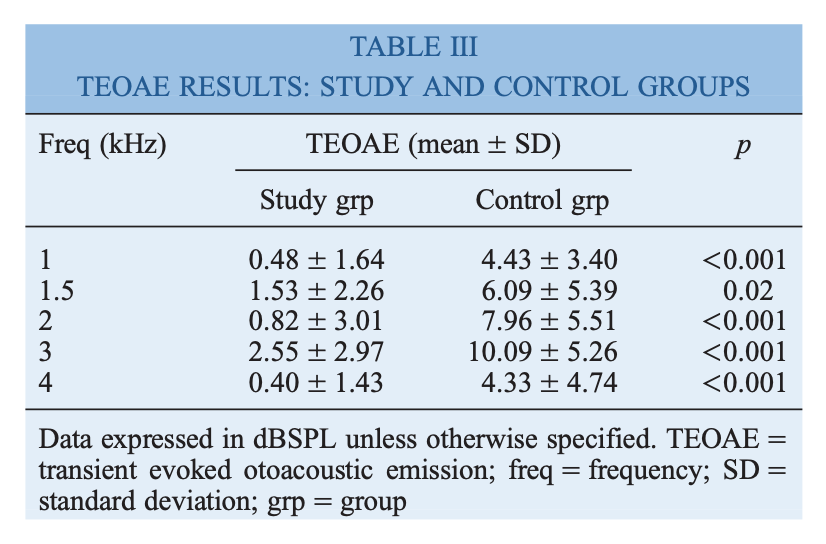
They reported that allergic rhinitis patients were statistically significantly worse than controls on transient evoked otoacoustic emissions, referring at all frequencies, as shown in the Table below.
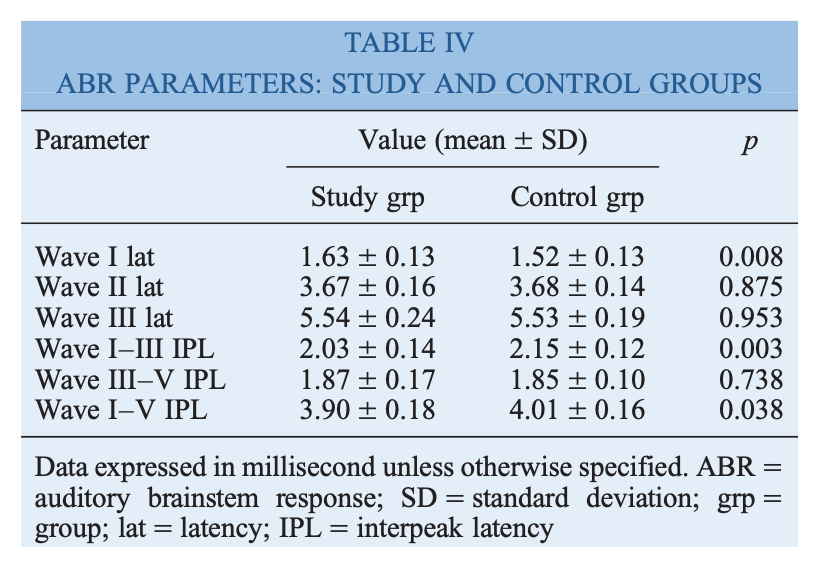
They reported that allergic rhinitis patients were statistically significantly worse than controls on brainstem auditory evoked responses in Wave I latency, Wave I‑III interpeak latency and Wave I‑V interpeak latency, as shown in the Table below.
The mechanism by which allergic rhinitis would provoke these otologic test results is unclear.
Testing: vestibular
As of this writing there were no recent publications that systematically studied vestibular tests in diagnosed allergy patients.
Testing: other
Cisi and colleagues (Cisi, Moreira et al. 2011), and Domingues and colleagues (Cisi, Moreira et al. 2010) studied 75 patients with “imbalance due to peripheral origin” using skin prick testing for 13 inhalants and for 5 foods. They observed that 25 (33%) of patients exhibited positive skin prick tests and at least one food allergen. Of these patients four had positive skin prick tests even without any traditional allergic symptoms. They concluded that, “The prevalence of Type I hypersensitivity reactions to inhalants and food in the [studied] population was greater than in the general population.”
Treatment
Since the relationship between allergy and otovestibular symptoms is unclear, it is unsurprising that there are no treatment trials.
Practically, when we encounter patients with both allergic symptoms and otovestibular symptoms whose otovestibular workups are normal, we will often suggest a trial of over-the-counter allergy medication. If that fails, we will refer for a formal allergy consultation, with the goal of identifying whether there is a specific allergy whose treatment may be more targeted.
References
Cisi ED, Moreira BRS, Ferreira de Mello J, Jr. (2010) Hypersensitivity to inhalants and food in balance disturbances. Rev Laryngol Otol Rhinol (Bord) 131: 243-6.
Cisi ED, Moreira BRS, Ferreira de Mello J, Jr. (2011) Hypersensitivity to inhalants and food in balance disturbances. Rev Laryngol Otol Rhinol (Bord) 132: 81-4.
Clemis JD (1972) Allergic cochleovestibular disturbances. Trans Am Acad Ophthalmol Otolaryngol 76: 1451-7.
Derebery MJ (1997) The role of allergy in Meniere’s disease. Otolaryngol Clin North Am 30: 1007-16.
Derebery MJ, Berliner KI (2007) Allergy and Meniere’s disease. Curr Allergy Asthma Rep 7: 451-6. doi: 10.1007/s11882-007-0069-0
Derebery MJ, Berliner KI (2010) Allergy and its relation to Meniere’s disease. Otolaryngol Clin North Am 43: 1047-58. doi: 10.1016/j.otc.2010.05.004
Derebery MJ, Valenzuela S (1992) Meniere’s syndrome and allergy. Otolaryngol Clin North Am 25: 213-24.
Di Berardino F, Barozzi S, Cesarani A (2005) Allergy and Meniere’s disease: a review. Eur Ann Allergy Clin Immunol 37: 299-300.
Floberg LE, Koch H (1954) Vestibular symptoms elicited through allergy. Acta Otolaryngol Suppl 116: 94-9.
Lasisi AO, Abdullahi M (2008) The inner ear in patients with nasal allergy. J Natl Med Assoc 100: 903-5.
McLaurin JW (1946) Desensitization by histamine (histamine azoprotein) in vertigo, periodic headaches and vasomotor (allergic) rhinitis; review of the literature and report of 102 personal cases. Laryngoscope 56: 253-81.
Pisani S (1958) [Allergic etiology of vertiginous syndromes]. Sem Med 112: 831-8.
Powers WH, House WF (1969) The dizzy patient–allergic aspect. Laryngoscope 79: 1330-8. doi: 10.1288/00005537-196907000-00010
Singh S, Nagarkar AN, Bansal S, Vir D, Gupta AK (2011) Audiological manifestations of allergic rhinitis. J Laryngol Otol 125: 906-10. doi: 10.1017/S0022215111001137
Strandbygaard E (1955) [Vertigo attacks caused by allergy]. Z Laryngol Rhinol Otol 34: 371-6.
Weinreich HM, Agrawal Y (2014) The link between allergy and Meniere’s disease. Curr Opin Otolaryngol Head Neck Surg 22: 227-30. doi: 10.1097/MOO.0000000000000041
Wilson WH, Powers WH (1971) Metabolic and allergic aspects of inner ear problems. J Otolaryngol Soc Aust 3: 181-6.
![]()