By Marcello Cherchi, MD PhD
For patients
In simple terms, the phrase “cervicogenic tinnitus” refers to tinnitus (perception of a sound) supposedly originating from the neck, occurring in a patient who also has neck symptoms. A reasonable approach to this is to start by checking basic tests of hearing. If those hearing tests do not reveal an “ear” source of tinnitus, then a trial of manual physical therapy for the neck is reasonable. If neck physical therapy fails, then consultation with audiology for tinnitus masking is a reasonable next step.
For clinicians
Overview
In a patient with non-pulsatile tinnitus and neck complaints it is medically reasonable to check screening audiometric testing, including audiometry (with tinnitus matching), otoacoustic emissions and brainstem auditory evoked responses. If these screening tests do not provide evidence for a primary otologic source of tinnitus, then a trial of manual physical therapy for the neck is reasonable. We do not generally recommend neck imaging as there is no evidence (yet) that results of imaging change management. If a reasonable trial of manual physical therapy for the neck is unsuccessful, then referral to a tinnitus audiologist (to be evaluated for tinnitus masking) is reasonable.
Introduction
The phrase “cervicogenic tinnitus” refers to a form of somatic tinnitus purportedly originating from neck pathology.
Association of tinnitus with cervical spine problems
The preliminary evidence for a connection between tinnitus and neck symptoms comes from studies noting an association between the two. For example, a meta-analysis of 22 studies commented that, “patients with tinnitus more frequently reported CSD [cervical spine disease] than subjects without tinnitus. The odds ratio was 2.6 (95% CI [1.1, 6.4]),” though the meta-analysis also cautioned that, “Methodological quality was generally limited by a lack of blinding, comparability of groups, and nonvalidated instruments for assessing CSD” (Bousema, Koops et al. 2018). While association does not prove causality, it is a reasonable starting point for studying this phenomenon.
What is the mechanism of cervicogenic tinnitus?
The topic of cervicogenic tinnitus is controversial for several reasons.
The first difficulty is that many studies of this topic do not clearly define what kind of cervical spine pathology is in question. One research group has contended that cervical spine pathology for this purpose can be adequately assessed by physical examination (Michiels, Van de Heyning et al. 2015), and on that basis, some of those same investigators conducted a study (Michiels, De Hertogh et al. 2015) that compared patients who carried a diagnosis of “cervicogenic somatic tinnitus” (CST) to patients with chronic non-pulsatile tinnitus not believed to be of cervical origin, and tried to identify specific cervical abnormalities on physical examination; the study concluded that the patients had a “positive manual rotation test, 47% a positive AST, 49% a positive score on both, and 81% had positive trigger points,” whereas in patients with non-CST, “these percentages were 36, 18, 10, and 50%, respectively.” Each group was also surveyed using the Neck Bournemouth Questionnaire (Bolton and Breen 1999, Bolton and Humphreys 2002), and the study found that, “79% of the CST group had a positive NBQ versus 40% in the non-CST group.”
The second difficulty is that the mechanism is by which a cervical problem could lead to tinnitus is unclear. There are various theoretical discussions of this (Gelb, Gelb et al. 1997), which often make the observation that, “neural connections and integration of the auditory and somatosensory systems of the upper cervical region and head have been confirmed by many studies” (Oostendorp, Bakker et al. 2016), but this alone does not explain the mechanism.
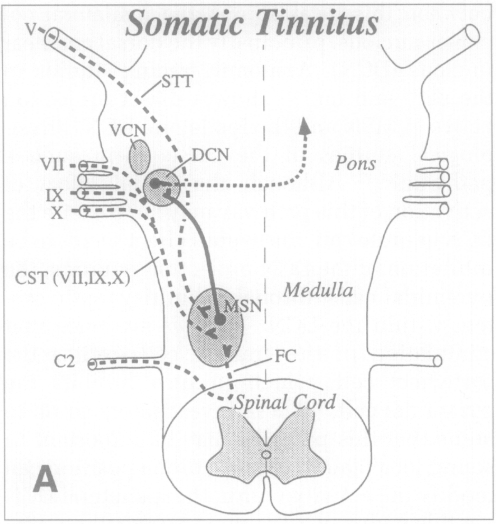
One of the more coherent explanations of a potential mechanism comes from Dr. Robert Levine (Levine 1999). Based on detailed neuroanatomical studies, human cases and animal studies, Levine hypothesizes, “that craniocervical somatic tinnitus occurs through modulation of the pathway from MSN [medullary somatosensory nuclei] to the ipsilateral DCN [dorsal cochlear nucleus],” with the relevant anatomy as illustrated in the figure below.
How is cervicogenic tinnitus diagnosed?
Patients who complain of tinnitus and who also complain of neck discomfort or who have suffered a neck injury may be suspected of having cervicogenic tinnitus, though this is merely an observation of association, not proof of a causal relationship. Some investigators suggest that if neck movements can modulate (increase or decrease) the tinnitus, then that supports the idea of a cervical mechanism of tinnitus (Ralli, Altissimi et al. 2016).
How is cervicogenic tinnitus treated?
Despite the poor understanding of the mechanism of cervicogenic tinnitus, and despite the lack of clear evidence for a causal relationship, numerous attempts at neck therapy have been undertaken.
Some “data” regarding treatment outcomes is simply in the form of case reports. For example, Bechter and colleagues report a case of an individual with cervicogenic tinnitus that remitted after treatment with a cervical collar (Bechter, Wieland et al. 2016).
Some studies suffer from patient selection problems. For example, the study by Delgado de la Serna and colleagues explored “cervico-mandibular therapies” in patients with either temporomandibular joint dysfunction or cervical problems (Delgado de la Serna, Plaza-Manzano et al. 2020), rather than isolating each group.
One study of cervicogenic tinnitus patients randomized subjects to receive “multimodal cervical physical therapy” immediately or in a delayed fashion, found symptomatic improvements to parallel the timing of the therapy, and concluded that “Cervical physical therapy can have a positive effect on subjective tinnitus complaints in patients with a combination of tinnitus and neck complaints” (Michiels, Van de Heyning et al. 2016). In effect, a study of this structure has no control group, and thus no way to exclude a placebo effect.
References
Bechter, K., M. Wieland and G. F. Hamann (2016). “Chronic Cervicogenic Tinnitus Rapidly Resolved by Intermittent Use of Cervical Collar.” Front Psychiatry 7: 43.
Bolton, J. E. and A. C. Breen (1999). “The Bournemouth Questionnaire: a short-form comprehensive outcome measure. I. Psychometric properties in back pain patients.” J Manipulative Physiol Ther 22(8): 503-510.
Bolton, J. E. and B. K. Humphreys (2002). “The Bournemouth Questionnaire: a short-form comprehensive outcome measure. II. Psychometric properties in neck pain patients.” J Manipulative Physiol Ther 25(3): 141-148.
Bousema, E. J., E. A. Koops, P. van Dijk and P. U. Dijkstra (2018). “Association Between Subjective Tinnitus and Cervical Spine or Temporomandibular Disorders: A Systematic Review.” Trends Hear 22: 2331216518800640.
Delgado de la Serna, P., G. Plaza-Manzano, J. Cleland, C. Fernandez-de-Las-Penas, P. Martin-Casas and M. J. Diaz-Arribas (2020). “Effects of Cervico-Mandibular Manual Therapy in Patients with Temporomandibular Pain Disorders and Associated Somatic Tinnitus: A Randomized Clinical Trial.” Pain Med 21(3): 613-624.
Gelb, H., M. L. Gelb and M. L. Wagner (1997). “The relationship of tinnitus to craniocervical mandibular disorders.” Cranio 15(2): 136-143.
Levine, R. A. (1999). “Somatic (craniocervical) tinnitus and the dorsal cochlear nucleus hypothesis.” Am J Otolaryngol 20(6): 351-362.
Michiels, S., W. De Hertogh, S. Truijen and P. Van de Heyning (2015). “Cervical spine dysfunctions in patients with chronic subjective tinnitus.” Otol Neurotol 36(4): 741-745.
Michiels, S., P. Van de Heyning, S. Truijen and W. De Hertogh (2015). “Diagnostic Value of Clinical Cervical Spine Tests in Patients With Cervicogenic Somatic Tinnitus.” Phys Ther 95(11): 1529-1535.
Michiels, S., P. Van de Heyning, S. Truijen, A. Hallemans and W. De Hertogh (2016). “Does multi-modal cervical physical therapy improve tinnitus in patients with cervicogenic somatic tinnitus?” Man Ther 26: 125-131.
Oostendorp, R. A., I. Bakker, H. Elvers, E. Mikolajewska, S. Michiels, W. De Hertogh and H. Samwel (2016). “Cervicogenic somatosensory tinnitus: An indication for manual therapy? Part 1: Theoretical concept.” Man Ther 23: 120-123.
Ralli, M., G. Altissimi, R. Turchetta, F. Mazzei, M. Salviati, F. Cianfrone, M. P. Orlando, V. Testugini and G. Cianfrone (2016). “Somatosensory Tinnitus: Correlation between Cranio-Cervico-Mandibular Disorder History and Somatic Modulation.” Audiol Neurootol 21(6): 372-382.
![]()