By Marcello Cherchi, MD PhD
For patients
Convergence-retraction nystagmus (CRN) is an eye movement abnormality in which, when a patient attempts to look upwards, the eyes instead point inward (converge) or move backwards slightly. This usually begins abruptly in adulthood; less commonly it comes on gradually or begins in childhood. There are several potential underlying causes. A patient with CRN will usually get brain imaging (typically an MRI). The treatment and prognosis depend on the underlying cause.
For clinicians
Overview
Convergence-retraction nystagmus (CRN) is a relatively rare, acquired pattern of usually intermittent abnormal eye movements in which an attempt at upward gaze instead elicits either convergence (bilateral adduction) or retraction (simultaneous co-contraction of the medial and lateral recti of each eye, pulling the globe posteriorly into the orbit) or both. This ocular motor finding localizes to the midbrain. It can occur in isolation, but often is found in conjunction with other ocular motor abnormalities, depending on the etiology and extent of the lesion. Presenting symptoms may include difficulty reading, diplopia, disequilibrium and others. Etiologies include compressive lesions (such as a pineal mass), ischemic or hemorrhagic infarcts, hydrocephalus and seizures; consequently imaging (preferably brain MRI) is appropriate. Treatment and prognosis depend on the underlying etiology.
Introduction
Convergence-retraction nystagmus (CRN) is a relatively rare, acquired pattern of usually intermittent abnormal eye movements in which an attempt at upward gaze instead elicits either convergence (bilateral adduction) or retraction (simultaneous co-contraction of the medial and lateral recti of each eye, pulling the globe posteriorly into the orbit) or both. This ocular motor finding localizes to the midbrain. It can occur in isolation, but often is found in conjunction with other ocular motor abnormalities, depending on the etiology and extent of the lesion.
Epidemiology
Convergence-retraction nystagmus (CRN) is relatively rare. It occurs in a subset of cases of destructive lesions (tumor, stroke) that affect the midbrain, and less commonly in seizures with periodic lateralizing epileptiform discharges.
Pathophysiological mechanism of disease
The mechanism of convergence-retraction nystagmus (CRN) is incompletely understood, in part because of the different ocular motor abnormalities that comprise this phenomenon (Leigh and Rucker 2005; Ortiz et al. 2021). Some investigators maintain that CRN is fundamentally a disorder of saccades (Ochs et al. 1979), while others maintain that it is a disorder of vergence movements (Rambold et al. 2001).
Rambold and colleagues state that, “Lesions associated with CRN are thought to be localized in the midbrain, lateral and anterior to the oculomotor nucleus” (Rambold et al. 2001).
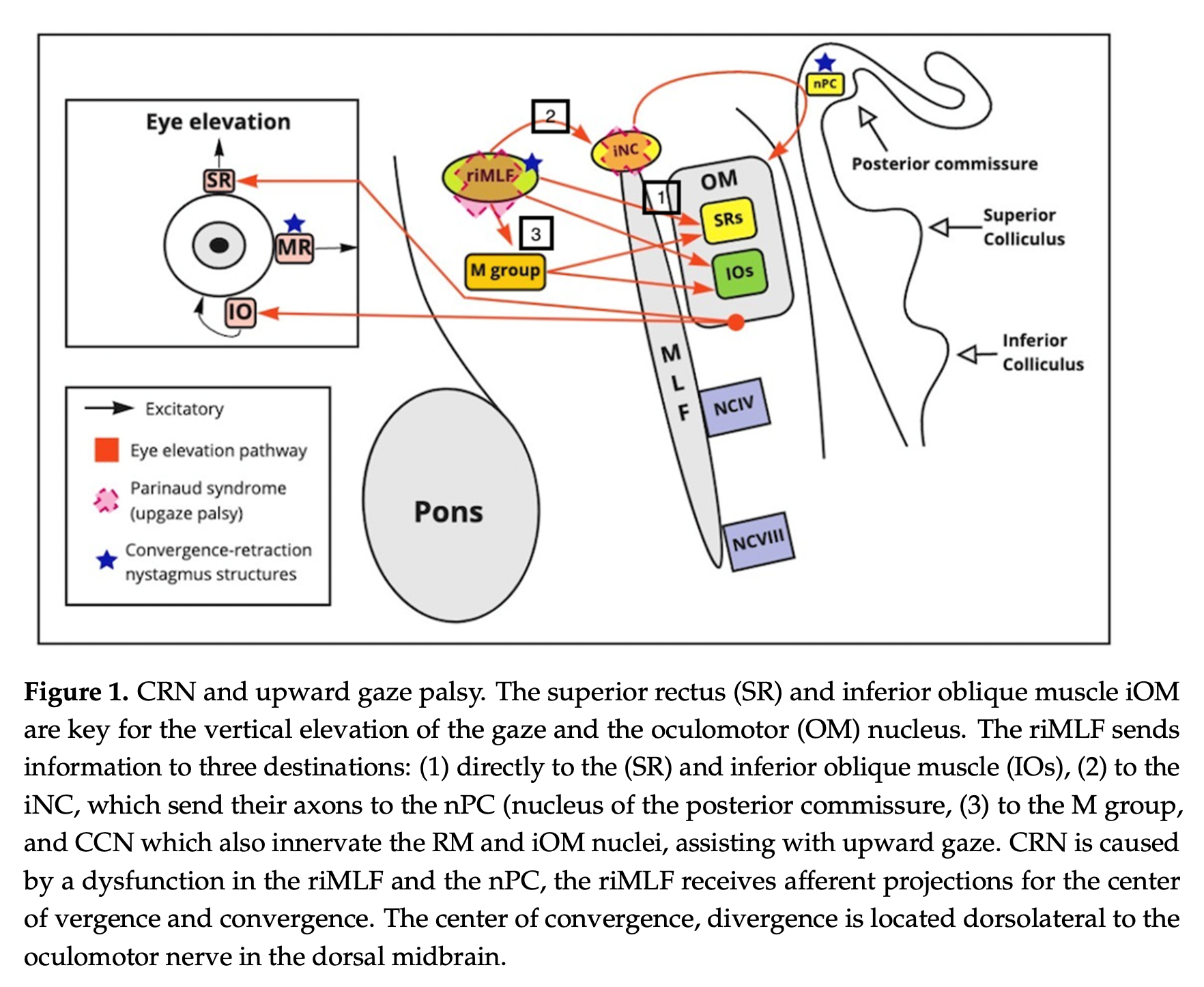
The Figure below, from a discussion of Parinaud’s syndrome, Ortiz and colleagues (Ortiz et al. 2021) show several pathologies, but as far as convergence-retraction nystagmus is concerned, they state that, “CRN arises from a dysfunction in the riMLF [rostral interstitial nucleus of the median longitudinal fasciculus] and PC [posterior commissure].”
Clinical presentation
Although speaking of the broader pretectal syndrome (and not only of convergence-retraction nystagmus), Keane’s review of 206 patients (Keane 1990) concluded that, “Symptoms varied with the etiology, which in many patients had a rapid or catastrophic onset.” Most published cases describe abrupt-onset of symptoms, typically from infarction (Brenner and Carlow 1979; Luda et al. 1992; Man and Fu 2014).
Gradual onset over months is less common and usually occurs in the context of a degenerative etiology (Chen et al. 2022), or a gradually developing compressive etiology such as a tumor (Margolin and Emami 2020) or hydrocephalus (Ochs et al. 1979; Sato et al. 1983).
Presenting symptoms can include:
- Difficulty reading (Ochs et al. 1979).
- Diplopia (Chen et al. 2022; Margolin and Emami 2020; Ochs et al. 1979; Rambold et al. 2001; Sato et al. 1983; Woodward et al. 2020).
- “Dizziness” (Rambold et al. 2001)
- “Droopy eyelids” (Chen et al. 2022).
- Convulsions if occurring in the context of seizures (Brenner and Carlow 1979).
- Coma (Scheitler et al. 2021).
Physical examination
In a patient with isolated convergence-retraction nystagmus (CRN), general physical examination may be normal (Woodward et al. 2020). Depending on the extent and location of the underlying lesion, other physical examination findings may be present (Keane 1990).
Ocular motor examination
Convergence-retraction nystagmus (CRN) can occur in isolation (Woodward et al. 2020), but often it occurs in conjunction with other ocular motor disorders, such as in the context of the pretectal syndrome (Keane 1990). It occurs in about 34% of cases of pretectal syndrome (Pullicino et al. 2000).
When the patient tries to execute an upward saccade (attempted voluntarily or in response to downward-moving optokinetic stimuli; see below) there is either retraction or convergence or some combination thereof. The convergence is, of course, bilateral adduction, brought about by simultaneous contraction of the medial recti and relaxation of the lateral recti. The retraction— posterior movement of the globes within the orbits — is probably about by simultaneous co-contraction of the medial and lateral recti, though some investigators state that there is co-contraction of all extraocular muscles (Luda et al. 1992).
Convergence-retraction nystagmus can be elicited by instructing a patient to execute an upward saccade. Another method is to use an optokinetic drum with stripes oriented horizontally and moving downwards; this elicits expected slow phase downward (pursuit) eye movements, but instead of these being followed by a fast phase upward “resetting” saccade, there is a rapid (saccadic) movement that is either convergence, or retraction, or some combination thereof (Leigh and Rucker 2005).
In those patients with only convergence nystagmus (and no retraction nystagmus), the convergence is brought about by a fast phase (saccadic) movement, while the divergence back to primary position of gaze is brought about by a slow phase movement (Ortiz et al. 2021). Pullicino and colleagues comment that, “Convergence-retraction nystagmus (CNR) is not a true form of nystagmus but consists of closely spaced, alternating, adducting saccades” (Pullicino et al. 2000).
The Video below, from Margolin and Emami (Margolin and Emami 2020), demonstrates convergence nystagmus on face-to-face examination. This patient had a primary intracranial germinoma originating in the pineal gland compressing the quadrigeminal plate.
Imaging
Given the potential etiologies and differential diagnosis (see below), brain imaging (usually an MRI) is appropriate for patients with convergence-retraction nystagmus.
The Figure below, from Margolin and Emami (Margolin and Emami 2020), is a mid-sagittal MRI demonstrating a pineal mass (primary germinoma) compressing the quadrigeminal plate.

The Figure below, from Scheitler and colleagues (Scheitler et al. 2021), is a mid-sagittal MRI demonstrating intraparenchymal hemorrhage involving the right thalamus extending into the dorsal mesencephalon.

Differential diagnosis
Convergence-retraction nystagmus is one of several possible ocular motor findings in the pretectal syndrome (Keane 1990), variously referred to as Parinaud’s syndrome, Sylvian aqueduct syndrome, and dorsal midbrain syndrome.
Convergence-retraction nystagmus has been reported in:
- Pineal mass (Woodward et al. 2020).
- Lesions that damage the posterior commissure, such as pineal tumors (Daroff and Hoyt 1971; Ochs et al. 1979; Pullicino et al. 2000).
- Leigh syndrome (subacute necrotizing encephalopathy), reported in a 6-year-old boy (Chen et al. 2022).
- Infarctions (ischemic or hemorrhagic) involving the pretectal area, posterior commissure and dorsomedial thalamic nuclei (Luda et al. 1992) thalamomesencephalic region (Man and Fu 2014; Scheitler et al. 2021).
- Chiari malformation.
- Hydrocephalus (Sato et al. 1983).
- Seizures. Examples of reported cases include a 65-year-old man (Brenner and Carlow 1979) and a 57-year-old woman (Young et al. 1977). In these cases the patients had complex focal seizures that initially presented with lateralizing motor symptoms and impaired consciousness, but those ceased and were replaced by periodic lateralizing epileptiform discharges synchronous with convergence-retraction nystagmus.
Treatment
Treatment of convergence-retraction nystagmus depends on the underlying etiology.
Prognosis
Prognosis of convergence-retraction nystagmus depends on the underlying etiology.
References
Brenner RP, Carlow TJ (1979) PLEDs and nystagmus retractorius. Ann Neurol 5: 403. doi: 10.1002/ana.410050420
Chen W, Feny C, Chu S, Zhao G, Sun X, Li Z, Chen Q, Tian G (2022) Convergence-Retraction Nystagmus and Ophthalmoplegia as the Presenting Sign of Leigh Syndrome in a Young Boy. J Neuroophthalmol. doi: 10.1097/WNO.0000000000001730
Daroff RB, Hoyt WF (1971) Supranuclear disorders of ocular control systems in man: Clinical, anatomical and physiological correlations. In: Bach-y-Rita P, Collins CC, Hyde JE (eds) The control of eye movements. Academic Press, New York, pp 175-235
Keane JR (1990) The pretectal syndrome: 206 patients. Neurology 40: 684-90. doi: 10.1212/wnl.40.4.684
Leigh JR, Rucker JC (2005) Nystagmus and related ocular motility disorders. In: Miller NR, Newman NJ (eds) Walsh & Hoyt’s Clinical Neuro-Ophthalmology, 6th edition edn, vol 1. Lippincott Williams & Wilkins, 530 Walnut Street, Philadelphia, Pennsylvania 19106 USA; 351 West Camden Street, Baltimore, Maryland 21201-2436 USA, pp 1133-1173
Luda E, Sicuro L, Albera R, Roberto C, De Lucchi R (1992) Retraction-convergence nystagmus: clinical and radiological study of 4 cases of vascular origin. Ital J Neurol Sci 13: 119-24. doi: 10.1007/BF02226959
Man BL, Fu YP (2014) See-saw nystagmus, convergence-retraction nystagmus and contraversive ocular tilt reaction from a paramedian thalamomesencephalic infarct. BMJ Case Rep 2014. doi: 10.1136/bcr-2014-206851
Margolin E, Emami S (2020) Teaching Video NeuroImages: Convergence retraction nystagmus due to compressive lesion of the dorsal midbrain. Neurology 94: e2285-e2286. doi: 10.1212/WNL.0000000000009481
Ochs AL, Stark L, Hoyt WF, D’Amico D (1979) Opposed adducting saccades in convergence-retraction nystagmus: a patient with sylvian aqueduct syndrome. Brain 102: 497-508. doi: 10.1093/brain/102.3.497
Ortiz JF, Eissa-Garces A, Ruxmohan S, Cuenca V, Kaur M, Fabara SP, Khurana M, Parwani J, Paez M, Anwar F, Tamton H, Cueva W (2021) Understanding Parinaud’s Syndrome. Brain Sci 11. doi: 10.3390/brainsci11111469
Pullicino P, Lincoff N, Truax BT (2000) Abnormal vergence with upper brainstem infarcts: pseudoabducens palsy. Neurology 55: 352-8. doi: 10.1212/wnl.55.3.352
Rambold H, Kompf D, Helmchen C (2001) Convergence retraction nystagmus: a disorder of vergence? Ann Neurol 50: 677-81. doi: 10.1002/ana.1263
Sato Y, Maehara F, Utsunomiya H, Hayashi T, Moritaka K, Kaji M (1983) Convergence and retraction nystagmus in hydrocephalus due to shunt malfunction. Kurume Med J 30: 125-8. doi: 10.2739/kurumemedj.30.125
Scheitler KM, Mustafa R, Wijdicks EFM (2021) Lid and Convergence Retraction Nystagmus in Thalamic-Midbrain Hematoma. Neurocrit Care 34: 691-692. doi: 10.1007/s12028-020-01024-z
Woodward K, Sitaram A, Peters S (2020) Isolated convergence-retraction nystagmus secondary to intralesional haemorrhage of a pineal cyst: an easily missed neurological finding with potentially life-threatening consequences. BMJ Case Rep 13. doi: 10.1136/bcr-2019-233469
Young GB, Brown JD, Bolton CF, Sibbald WM (1977) Periodic lateralized epileptiform discharges (PLED’s) and nystagmus retractorius. Ann Neurol 2: 61-2. doi: 10.1002/ana.410020110
![]()