By Marcello Cherchi, MD PhD
For patients
Fibromyalgia (FM) is a rheumatologic disease that causes pain in the muscles and joints. Some FM patients also notice problems with hearing and balance. In a patient already diagnosed with FM who also has complaints regarding hearing and balance, a doctor may consider checking several tests to look for other common causes, but unless a better explanation is found, continued management of FM (by a rheumatologist) is appropriate. In patients with hearing problems, consultation with an audiologist is reasonable. In patients with disequilibrium, a trial of vestibular rehabilitation therapy is reasonable.
For clinicians
Overview
Fibromyalgia (FM) is a rheumatologic disorder of unknown etiology that manifests with diffuse musculoskeletal pains and a variety of other somatic, constitutional and cognitive/psychiatric symptoms. A substantial percentage of FM patients endorse auditory complaints (hearing loss, tinnitus) and vestibular complaints (disequilibrium and falls). From an otoneurological perspective, physical examination is normal. FM patients tend to have high frequency (4 – 8 kHz) hearing loss beyond age-matched controls. Instrumented ocular motor testing of smooth pursuit may show reduced gain. Posturography shows poorer performance in all sensory organization testing conditions compared to healthy controls. Since these features do not distinguish whether otovestibular symptoms are due to FM or some other pathology, it is medically reasonable to undertake a screening otovestibular workup. Unless an alternative diagnosis is found, referral to audiology (regarding complaints of hearing loss and/or tinnitus) and a trial of vestibular rehabilitation therapy are reasonable. Of course, the FM itself should be managed by rheumatology.
Introduction
Fibromyalgia (FM), sometimes referred to as fibrositis in older literature, is a controversial clinical entity that manifests with widespread musculoskeletal pain and is often accompanied by other somatic symptoms, constitutional symptoms (such as fatigue) and cognitive/psychiatric symptoms (Arnold et al. 2019). Despite the prominent symptom of musculoskeletal pain and tenderness, there is no evidence of inflammation in the affected tissues, so more recent research has explored the possibility that FM is a form of central sensitization — in other words, a disorder of central pain regulation.
Problems with hearing and balance are among the many symptoms endorsed by FM patients, and some literature suggests that in some patients, otovestibular symptoms may be due to FM itself.
Epidemiology
Among rheumatological diseases, FM is relatively common. Queiroz (Queiroz 2013) reviewed a large number of epidemiological studies on FM and reported that the global mean prevalence was 2.7%, ranging from a low of 0.4% in Greece to a high of 9.3% in Tunisia. Queiroz found that few studies explore the incidence of FM; of those that do, one study found an incidence rate of 5.83 new cases per 1,000 person years among females; another study found an incidence rate of 6.88 new cases per 1,000 person-years among males, and 11.28 new cases per 1,000 person-years for females. Globally, females are affected more than males by a ratio of 3:1.
Genetics
Study of the genetics of FM is still in a fairly preliminary phase (D’Agnelli et al. 2019). Whether there are any specific genetic factors driving otovestibular symptoms related to FM has not been studied.
Pathophysiological mechanism of disease
Even after acknowledging that FM is incompletely understood, it should be added that the mechanism by which FM might cause otovestibular symptoms is even more poorly understood. Rusy and colleagues (Rusy et al. 1999) studied 12 children with FM using electronystagmography and rotatory chair testing and found no abnormalities. They concluded that, “These findings suggest that central (brainstem) and peripheral vestibular (inner ear) mechanisms do not account for the complaints of dizziness in the pediatric patient with fibromyalgia. The common musculoskeletal abnormalities of fibromyalgia may affect their proprioceptive orientation, therefore giving them a sense of imbalance.”
Clinical presentation: overall
Bayazit and colleagues (Bayazit et al. 2002) studied 24 female FM patients by history, physical examination, audiologic testing (audiometry, brainstem auditory evoked responses) and vestibular testing (bithermal caloric testing) and reported that, “Almost 50% of the patients had some sort of otologic symptoms” despite fairly normal otovestibular test results, and concluded that, “FM patients can complain otologic symptoms even though they do not have any clinically or audiologically detectable ear disease.”
Clinical presentation: auditory symptoms
Bayazit and colleagues (Bayazit et al. 2002) studied 24 female FM patients and reported that 3 (13%) complained of hearing loss, and 4 (17%) complained of tinnitus.
Mucci and colleagues (Mucci et al. 2022) conducted a questionnaire-based study of 277 FM patients. They reported that 5.8% complained of “tinnitus.”
Wolfe and colleagues (Wolfe et al. 2012) studied 1199 FM patients and found that 36.2% (95% confidence interval 33.4% – 39.0%) complained of “hearing difficulties.”
Le and colleagues (Le et al. 2020) conducted a population-based retrospective cohort study of patients with new-onset FM. They compared 55,169 FM patients with 110,338 healthy controls and reported that, “The overall HL [hearing loss] risk in the FM group was 1.46-fold (95% confidence interval: 1.38 – 1.55) higher than that in the non-FM group.”
Clinical presentation: vestibular symptoms
Bayazit and colleagues (Bayazit et al. 2002) studied 24 female FM patients and reported that 9 (38%) complained of “dizziness” and 2 (8%) complained of “vertigo.”
Mucci and colleagues (Mucci et al. 2022) conducted a questionnaire-based study of 277 FM patients in an attempt “to establish a prevalence rate of vestibular symptoms in FM.” They reported that 63.6% of FM patients complained of “dizziness.”
Rosenhall and colleagues (Rosenhall et al. 1996) studied 168 FM patients, of whom 141 (83.9%) were women. They found that 72% of patients reported a complaint of “vertigo.” They further analyzed patient descriptions, and commented that of all 168 patients, “Most of them (48% of all patients) had slight, diffuse dizziness causing no or only minor discomfort. Four percent of all patients complained of constant, severe dizziness. Eighteen percent complained of attacks of rotatory or nautical vertigo. Disturbance of gait without dizziness or vertigo was reported by 2% of patients.”
Jones and colleagues (Jones et al. 2009) compared 34 FM patients (88% female) and 32 age-matched healthy controls through several questionnaires (Fibromyalgia Impact Questionnaire, Activities-specific Balance Confidence, report of falls) and a multi-factor gait and balance assessment called the Balance Evaluation Systems Test (BESTest) developed by Horak and colleagues (Horak et al. 2009). They concluded that, “FM is associated with balance problems and increased fall frequency.”
Jones and colleagues (Jones et al. 2011) compared 25 FM patients (88% female, mean age 50.8 ± 7.7 years) and 27 healthy control subjects (89% female, mean age 46.5 ± 10.9 years). They reported that, “FM patients reported significantly more falls over the past six months than HCs. Specifically, 3 (11%) of 27 HCs had fallen only once during the past six months, whereas 18 (72%) of 25 FM patients had fallen at least once, with 15 FM patients (60%) having fallen more than three times in the past six months.”
Physical examination
Aside from physical examination findings compatible with FM itself, there are no physical examination signs that are sensitive or specific for otovestibular symptoms in FM.
Ocular motor examination
Very few studies have specifically reported on positive bedside ocular motor findings in FM.
Rusy and colleagues (Rusy et al. 1999) studied pediatric FM and specifically commented that the following bedside findings were normal: spontaneous nystagmus, oculocephalic reflex, dynamic visual acuity, head shaking nystagmus, Quix test and the Dix-Hallpike maneuver.
In contrast, Bayazit and colleagues (Bayazit et al. 2002), who studied 24 female FM patients, reported that on the Dix-Hallpike maneuver, 21% had “rotary” nystagmus (without further description).
Testing: audiologic
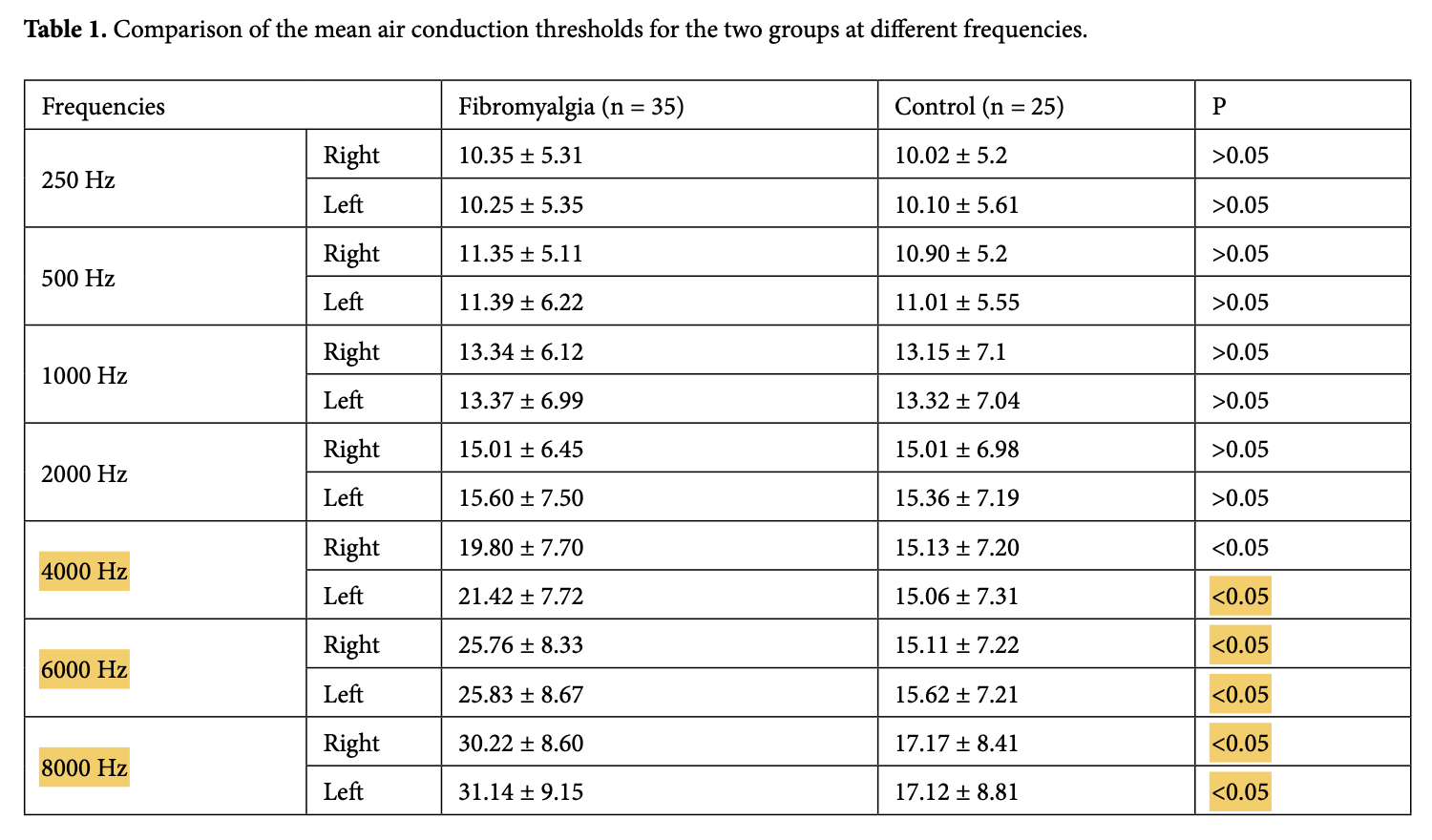
Gencer and colleagues (Kapusuz Gencer et al. 2017) compared audiometric results in 35 female FM patients (mean age 48.1 years, range 30 – 65 years) and 25 healthy control subjects. They reported that, “At high frequencies, the mean air conduction threshold values and tympanometric values between the FM and control groups were statistically significant (P < 0.05 for both).” The frequencies at which pure tone hearing was statistically significantly worse in FM patients than in healthy controls were 4 – 8 kHz, as shown in the Table below.
Testing: vestibular
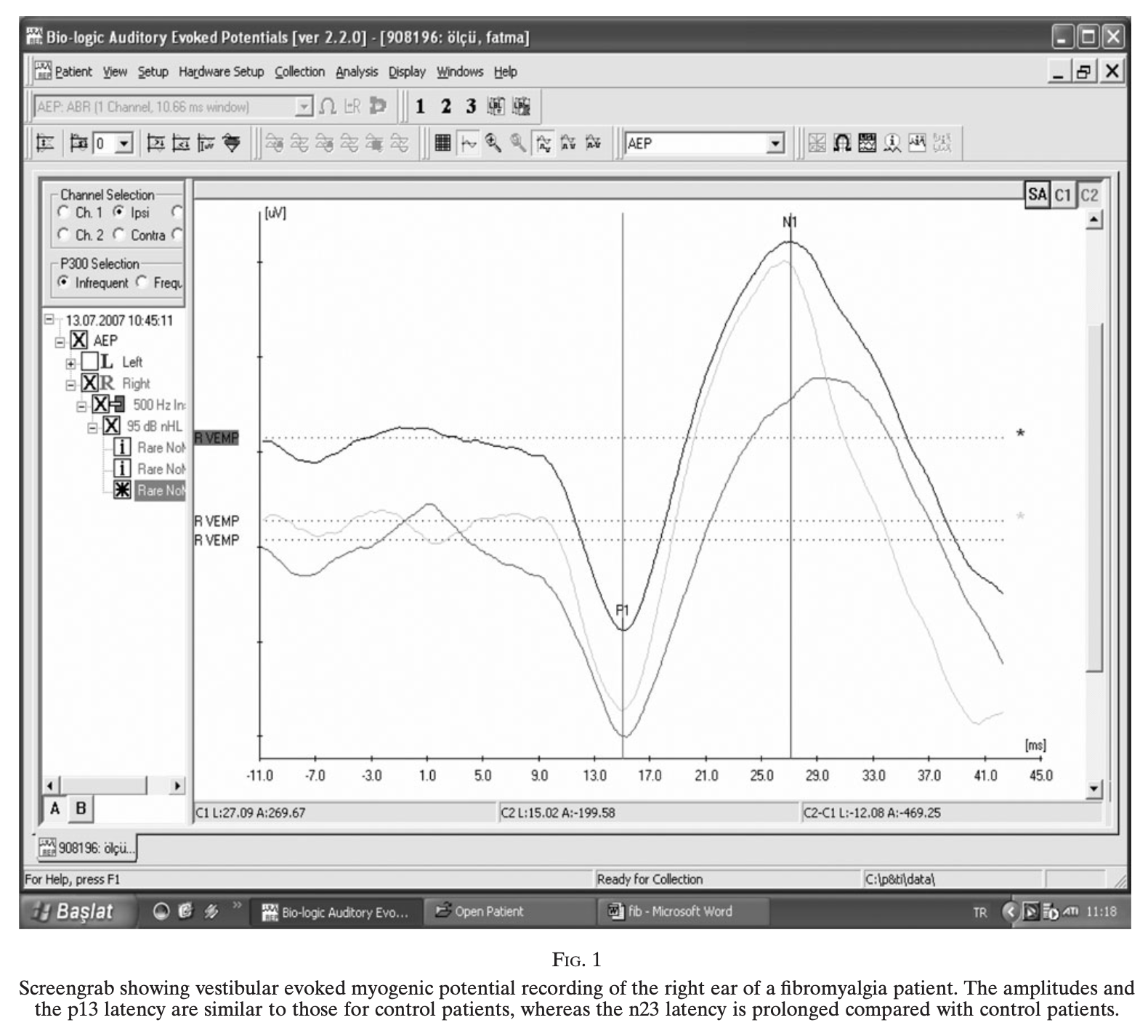
Bayazit and colleagues (Bayazit et al. 2010) compared cervical vestibular evoked myogenic potentials (cVEMPs) in 24 FM patients (22 women, 2 men) and 21 healthy female controls. They reported statistically significant differences between the two groups; specifically, the n23 latency was delayed, and the p13-n23 interpeak latency was prolonged, in FM patients compared to controls. The Figure below shows an example of the delayed n23 latency.
Rosenhall and colleagues (Rosenhall et al. 1996) compared ocular motor performance in 168 FM patients, of whom 141 (83.9%) were women, and 90 healthy controls, of whom 48 were women. With respect to smooth pursuit eye movements, they reported that, “The mean velocity gain was significantly lower in the patient group than in the control group for both women and men (p<0.001). Ninety-six of the 166 patients tested (58%) had pathological smooth pursuit eye movements. In all these cases the mean velocity gain of the 20 deg/sec smooth pursuits was significantly reduced. In 24% of all the patients the smooth pursuits were severely abnormal with a mean velocity gain of ≤0.5.”
Muto and colleagues (Muto et al. 2015) studied a case-control study of 117 women, of whom 67 carried a diagnosis of FM. The subjects completed several questionnaires and did (what from the authors’ description sounds like) static posturography. They concluded that, “Individuals with FM had impaired postural control showing increased speed of oscillation of the center of gravity (p=0.0004) and decreased balance self-efficacy (p<0.001).”
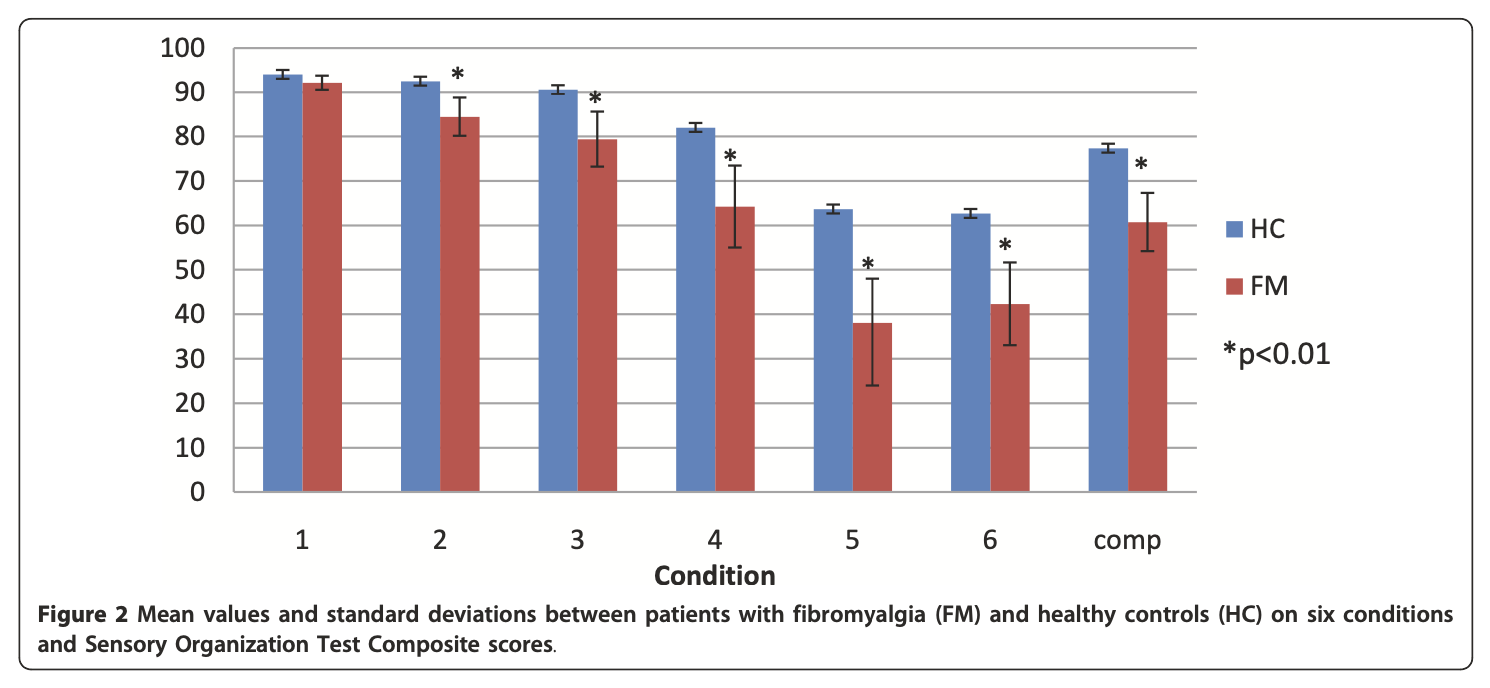
Jones and colleagues (Jones et al. 2011) compared 25 FM patients (88% female, mean age 50.8 ± 7.7 years) and 27 healthy control subjects (89% female, mean age 46.5 ± 10.9 years) using computerized dynamic posturography (CDP). They reported that on all six conditions of sensory organization testing, FM patients performed statistically significantly worse than healthy controls. Their findings are summarized in the Figure below.
Perez-se-Heredia-Torres and colleagues (Perez-de-Heredia-Torres et al. 2017) compared performance on computerized dynamic posturography (CDP) in 20 women with FM and 20 matched healthy controls. They reported that on sensory organization testing, “Women with FM exhibited balance deficiencies and used different strategies for maintaining their balance in standing” compared to healthy controls.
Differential diagnosis
In patients with FM, the characteristics of hearing and balance symptoms, and physical examination findings, cannot distinguish whether the etiology of the otovestibular symptoms is FM itself, or some other disease. Consequently, the differential diagnosis (of the otovestibular symptoms) is broad, and a reasonable screening search for known otovestibular disorders should be considered.
Treatment
As of this writing there were no specific trials regarding auditory and vestibular symptoms apparently associated with FM. If workup provides no evidence for an alternative explanation, then treatment of the fibromyalgia itself (under the guidance of a rheumatologist) is reasonable. If hearing loss and /or tinnitus are interfering with function, then referral to audiology is reasonable. Although vestibular rehabilitation therapy (VRT) has not been specifically studied for disequilibrium in FM, a trial of VRT is probably reasonable as it incurs no medical risk.
References
Arnold LM, Bennett RM, Crofford LJ, Dean LE, Clauw DJ, Goldenberg DL, Fitzcharles MA, Paiva ES, Staud R, Sarzi-Puttini P, Buskila D, Macfarlane GJ (2019) AAPT Diagnostic Criteria for Fibromyalgia. J Pain 20: 611-628. doi: 10.1016/j.jpain.2018.10.008
Bayazit YA, Celenk F, Gunduz AG, Gunduz B, Ondag N, Meray J (2010) Vestibular evoked myogenic potentials in patients with fibromyalgia syndrome. J Laryngol Otol 124: 610-5. doi: 10.1017/S0022215110000010
Bayazit YA, Gursoy S, Ozer E, Karakurum G, Madenci E (2002) Neurotologic manifestations of the fibromyalgia syndrome. J Neurol Sci 196: 77-80.
D’Agnelli S, Arendt-Nielsen L, Gerra MC, Zatorri K, Boggiani L, Baciarello M, Bignami E (2019) Fibromyalgia: Genetics and epigenetics insights may provide the basis for the development of diagnostic biomarkers. Mol Pain 15: 1744806918819944. doi: 10.1177/1744806918819944
Horak FB, Wrisley DM, Frank J (2009) The Balance Evaluation Systems Test (BESTest) to differentiate balance deficits. Phys Ther 89: 484-98. doi: 10.2522/ptj.20080071
Jones KD, Horak FB, Winters-Stone K, Irvine JM, Bennett RM (2009) Fibromyalgia is associated with impaired balance and falls. J Clin Rheumatol 15: 16-21. doi: 10.1097/RHU.0b013e318190f991
Jones KD, King LA, Mist SD, Bennett RM, Horak FB (2011) Postural control deficits in people with fibromyalgia: a pilot study. Arthritis Res Ther 13: R127. doi: 10.1186/ar3432
Kapusuz Gencer Z, Balbaloglu O, Ozkiris M, Saydam L (2017) Does fibromyalgia have an effect on hearing loss in women? Turk J Med Sci 47: 1699-1702. doi: 10.3906/sag-1511-25
Le TP, Tzeng YL, Muo CH, Ting H, Sung FC, Lee SD, Teng YK (2020) Risk of hearing loss in patients with fibromyalgia: A nationwide population-based retrospective cohort study. PLoS One 15: e0238502. doi: 10.1371/journal.pone.0238502
Mucci V, Demori I, Rapallo F, Molinari E, Losacco S, Marinelli L, Browne CJ, Burlando B (2022) Vestibular Disability/Handicap in Fibromyalgia: A Questionnaire Study. J Clin Med 11. doi: 10.3390/jcm11144017
Muto LH, Sauer JF, Yuan SL, Sousa A, Mango PC, Marques AP (2015) Postural control and balance self-efficacy in women with fibromyalgia: are there differences? Eur J Phys Rehabil Med 51: 149-54.
Perez-de-Heredia-Torres M, Huertas-Hoyas E, Martinez-Piedrola R, Palacios-Cena D, Alegre-Ayala J, Santamaria-Vazquez M, Fernandez-de-Las-Penas C (2017) Balance deficiencies in women with fibromyalgia assessed using computerised dynamic posturography: a cross-sectional study in Spain. BMJ Open 7: e016239. doi: 10.1136/bmjopen-2017-016239
Queiroz LP (2013) Worldwide epidemiology of fibromyalgia. Curr Pain Headache Rep 17: 356. doi: 10.1007/s11916-013-0356-5
Rosenhall U, Johansson G, Orndahl G (1996) Otoneurologic and audiologic findings in fibromyalgia. Scand J Rehabil Med 28: 225-32.
Rusy LM, Harvey SA, Beste DJ (1999) Pediatric fibromyalgia and dizziness: evaluation of vestibular function. J Dev Behav Pediatr 20: 211-5. doi: 10.1097/00004703-199908000-00002
Wolfe F, Rasker JJ, Hauser W (2012) Hearing loss in fibromyalgia? Somatic sensory and non-sensory symptoms in patients with fibromyalgia and other rheumatic disorders. Clin Exp Rheumatol 30: 88-93.
![]()