By Marcello Cherchi, MD PhD
For patients
Gluten ataxia is thought to be an autoimmune disease provoked by exposure to gluten, a protein found in wheat and some other grains. Symptoms usually begin in middle adulthood (though the range of age of onset is broad), start subtly, and progress slowly. The symptoms are chronic, and usually include unsteadiness and imbalance; some patients also experience dysarthria (difficulty pronouncing words). If your doctor suspects gluten ataxia, they may check a brain imaging study (such as an MRI) or several blood tests. The treatment for gluten ataxia is to start and maintain a strict gluten-free diet. It can be difficult to start and maintain a gluten-free diet because it is not always clear which foods contain gluten, and also because an improper gluten-free diet may increase the risk of developing a nutritional deficiency, so most patients will get advice about this from a medical dietician or nutritionist.
For clinicians
Overview
Gluten ataxia (GA) is an autoimmune-mediated cerebellar ataxia believe to be provoked by exposure to gluten (a protein contained in wheat and several other grains). GA can occur in the context of other gluten-sensitive diseases (such as celiac disease) or in isolation. The age of onset is a broad range (from the 2ndto the 9th decades), though most studies report a mean age of onset in the 5th or 6th decades. GA affects males and females approximately equally. Some studies suggest that GA may account for 25 – 36% of sporadically occurring cerebellar ataxias. Symptoms usually start insidiously and progress slowly, though occasional cases have been reported of abrupt onset or rapid progression. Some literature suggests that alcohol intake may increase the risk of GA. The most common presenting symptoms include gait ataxia, limb ataxia and dysarthria. Physical examination may show midline and hemispheric cerebellar signs, as well as ocular motor findings compatible with cerebellar dysfunction. The serum antibodies detected are usually anti-gliadin IgG antibodies (more common) and anti-transglutaminase-6 IgA antibodies (less common). These antibodies are thought to attack Purkinje cells, though autopsy studies also show damage of cerebellar granular neurons, cerebellar nuclei and inferior olivary neurons. MR imaging often shows cerebellar atrophy, but MR spectroscopy can show abnormal cerebellar metabolism even in the absence of atrophy. The mainstay of treatment is a strict gluten-free diet, though this should not be taken lightly as it is not risk-free. Less studied (and thus second-line) therapies include intravenous immunoglobulin, plasmapheresis, corticosteroids or other immunosuppressants. Earlier treatment (including dietary treatment) retards progression in some (but not all) patients
The main value of identifying (or suspecting) gluten ataxia is that it is one of the few cerebellar ataxias for which treatment (usually gluten-free diet) has the potential to reverse symptoms, or retard their progression (Hadjivassiliou et al. 2003a).
In a patient with biopsy-proven celiac disease who has ataxia it is likely that the ataxia is also gluten-mediated, though it is still reasonable for the clinician to keep in mind a differential diagnosis that includes other causes of ataxia (such as alcoholism). A patient with celiac disease will likely be instructed by their gastroenterologist to initiate and maintain a gluten-free diet, and if in so doing the ataxia also improves, then ex joventibus the ataxia was likely gluten-related.
In a patient without celiac disease and without gastrointestinal symptoms who presents in adulthood with insidious onset, gradually progressive ataxia and no family history suggestive of any genetically-mediated ataxia, it is reasonable to suspect gluten ataxia. Obtaining a brain MRI is reasonable as this may (1) show cerebellar atrophy and (2) help exclude other diseases. Checking for anti-gliadin antibodies and anti-transglutaminase-6 antibodies is also reasonable. If there is reasonable evidence and suspicion for GA, then initiating and maintaining a strict gluten-free diet is reasonable, though this dietary change should ideally be supervised by a medical dietician or nutritionist.
Introduction
The topic of gluten ataxia is a “contentious concept” (Serratrice, Attarian et al. 2004), with opposing views expressed in the same journal issue, such as “Gluten ataxia: an overestimated condition?” (Meira, Franklin et al. 2022) and “Gluten ataxia: an underdiagnosed condition” (Hadjivassiliou and Grupsilonnewald 2022).
Mitoma and colleagues (Mitoma, Manto et al. 2021) credit Jean-Martin Charcot with having published the first description of a cerebellar ataxia as an immune-mediated illness in 1868 (Charcot 1868). Some investigators (Hadjivassiliou, Sanders et al. 2010) credit Cooke and Smith with having provided the “first comprehensive report of neurological manifestations in the context of histologically confirmed coeliac disease” in 1966 (Cooke and Smith 1966).
Hadjivassiliou and colleagues began publishing on this topic in 1998 (Hadjivassiliou, Grunewald et al. 1998), and has contributed substantially to the literature (Hadjivassiliou, Grunewald et al. 1998, Hadjivassiliou, Grunewald et al. 2001, Hadjivassiliou, Boscolo et al. 2002, Hadjivassiliou, Davies-Jones et al. 2003, Hadjivassiliou, Grunewald et al. 2003, Hadjivassiliou, Maki et al. 2006, Hadjivassiliou, Aeschlimann et al. 2008, Hadjivassiliou, Sanders et al. 2008, Hadjivassiliou, Sanders et al. 2010, Hadjivassiliou 2012, Hadjivassiliou, Wallis et al. 2012, Hadjivassiliou, Aeschlimann et al. 2013, Hadjivassiliou, Duker et al. 2014, Hadjivassiliou, Sanders et al. 2015, Hadjivassiliou, Grunewald et al. 2017, Hadjivassiliou, Martindale et al. 2017, Hadjivassiliou, Grunewald et al. 2018, Hadjivassiliou and Grupsilonnewald 2022, Hadjivassiliou, Manto et al. 2022).
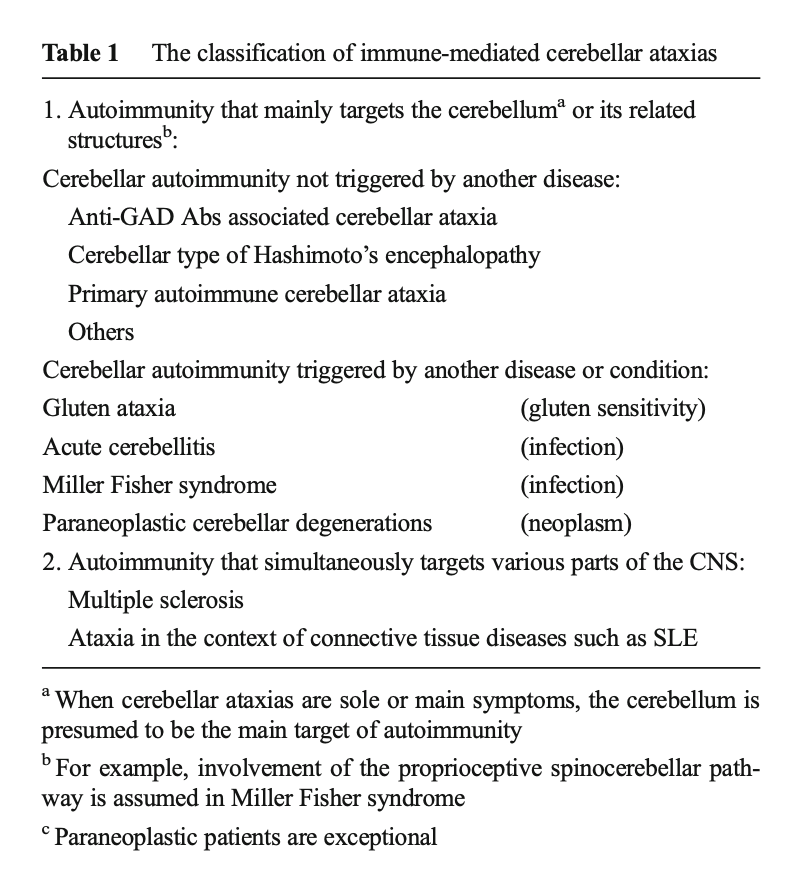
Celiac disease is an autoimmune gastrointestinal illness whose diagnosis can be secured from duodenal biopsy. Dicke and colleagues are credited with having identified the wheat protein gluten as the antigen (Dicke, Weijers et al. 1953). When an individual with biopsy-proven celiac disease develops other symptoms, it is reasonable to speculate that the other symptoms may also be mediated by an autoimmune mechanism. In the case of cerebellar ataxias, this seems especially reasonable since a range of autoimmune-mediated cerebellar ataxias have already been well-described.
The Table below, from Mitoma and colleagues (Mitoma, Adhikari et al. 2016), lists the main cerebellar ataxias that have been attributed to an autoimmune mechanism.
In some cases an individual with cerebellar ataxia but no gastrointestinal symptoms may be found on duodenal biopsy to have celiac disease, and in such circumstances the patient is often described as having “sub-clinical celiac disease” (Pellecchia, Scala et al. 1999, Jain, Bhaduri et al. 2019).
The scenario becomes more complex when an individual has neither gastrointestinal symptoms nor histopathologic evidence of celiac disease (Hadjivassiliou, Grunewald et al. 2003, Guan, Liu et al. 2013, Rodrigo, Hernandez-Lahoz et al. 2016). This situation is sometimes referred to as “non-celiac gluten sensitivity” (NCGS) — but the broader concept is that an immunological response to gluten is somehow causing an ataxia.
Epidemiology of gluten ataxia
In the series of 100 gluten ataxia patients studied by Hadjivassiliou and colleagues, the mean age at onset of ataxia was 53 years (Hadjivassiliou 2012), though the age range is quite broad. Hadjivassiliou and colleagues studied 68 patients with gluten ataxia and reported the age of onset to range from 14 – 81 years, with a mean of 48 years (Hadjivassiliou, Grunewald et al. 2003). Although this is predominantly a disease of older patients, it can (rarely) also occur in the pediatric population (Gordon 2000).
In a series of 404 patients with sporadically occurring progressive ataxia, Hadjivassiliou reported that 101 (25%) had gluten ataxia (Hadjivassiliou 2012) which, if correct, makes gluten ataxia among the most common of all sporadically-occurring ataxias.
A case series of sporadically occurring cerebellar ataxias in Japan reported that 5/14 (36%) of patients were found to nave anti-gliadin antibodies (Ihara, Makino et al. 2006).
In the series analyzed by Hadjivassiliou, the disease is nearly equally distributed between males (49%) and females (51%).
Risk factors
There is modest evidence that alcohol intake may increase susceptibility to gluten ataxia (Currie, Hoggard et al. 2013). The mechanism for this is not known; it is not clear whether cerebellar toxicity of alcohol simply adds to what would otherwise have been an isolated gluten-mediated autoimmune cerebellar insult, or whether alcohol somehow potentiates the autoimmune process itself.
Clinical presentation
The Table below, from Hadjivassiliou (Hadjivassiliou, Sanders et al. 2010), lists other clinical features of patients with gluten ataxia.

Symptoms less commonly reported in association with gluten ataxia include palatal tremor (Kheder, Currie et al. 2012), cognitive impairment (Makhlouf, Messelmani et al. 2018) and myoclonus (Sarrigiannis, Hoggard et al. 2014). One might speculate that these are “gluten ataxia plus” syndromes — in other words, cases in which gluten ataxia is only one facet of a broader gluten-triggered autoimmune disease.
Physical examination
Hadjivassiliou and colleagues reported that in a series of 68 patients with gluten ataxia, 100% exhibited gait ataxia, 90% exhibited lower limb ataxia, and 70% exhibited upper limb ataxia (Hadjivassiliou, Grunewald et al. 2003).
Burk and colleagues (Burk, Bosch et al. 2001) studied 104 patients with sporadic cerebellar ataxia and reported that 100% exhibited ataxia of stance and gait, 100% exhibited dysarthria, and 97% exhibited limb ataxia.
Ocular motor examination
Hadjivassiliou and colleagues reported that in a series of 68 patients with gluten ataxia, 84% exhibited “ocular signs,” which they qualify as, “spontaneous and gaze-evoked nystagmus and/or abnormal saccades” (Hadjivassiliou, Grunewald et al. 2003).
Burk and colleagues (Burk, Bosch et al. 2001) studied 104 patients with sporadic cerebellar ataxia and reported that 66.7% exhibited gaze-evoked nystagmus, 33.3% exhibited spontaneous nystagmus, 25% exhibited slowing of saccades and 16.7% exhibited an upward gaze palsy.
Mechanism
Similar to other exogenously-triggered autoimmune diseases, in gluten ataxia it has been suspected that antibody cross-reactivity (molecular mimicry) plays a significant mechanistic role (Green, Alaedini et al. 2005). Indeed, Hadjivassiliou and colleagues report experimental evidence suggesting such cross-reactivity between antigenic epitopes on Purkinje cells and gluten peptides (Hadjivassiliou, Boscolo et al. 2002). The specific target of these autoantibodies is not known, but some research suggests that it may be synapsin I (Alaedini, Okamoto et al. 2007).
Antibodies
A number of antibodies have been reported in the serum of patients with gluten ataxia. The best studied include anti-gliadin antibodies (Burk, Bosch et al. 2001, Abele, Schols et al. 2003) and anti-transglutaminase-6 antibodies (Hadjivassiliou, Aeschlimann et al. 2008, Hadjivassiliou, Aeschlimann et al. 2013, Osman, Umar et al. 2021).
Antibodies: anti-gliadin antibodies
Lock and colleagues (Lock, Tengah et al. 2006) studied a series of 20 patients with “idiopathic ataxia” and reported that anti-gliadin antibodies (either IgG or IgA) were found in 40% of patients.
Liu and colleagues (Liu, Soong et al. 2010) reported on a series of 361 patients with sporadic ataxia. They found that 9% of patients had “gluten sensitivity.” In these gluten sensitive patients they found anti-gliadin IgG and IgA antibodies, and t-transglutaminase IgA antibodies. They reported that anti-gliadin IgG antibodies were “more specific to the disease of sporadic ataxia.”
Rashtak and colleagues (Rashtak, Rashtak et al. 2011) report that levels of anti-gliadin antibodies are higher in gluten sensitive patients with both ataxia and enteropathy (which is to say, patients with celiac disease and ataxia) compared to patients with only ataxia but no enteropathy.
Not all investigators find a strong correlation between anti-gliadin antibodies and gluten ataxia (Wong, Dwinnel et al. 2007).
Antibodies: anti-gliadin antibodies occur in the healthy population
Anti-gliadin antibodies are present in about 10% of asymptomatic individuals (Lock, Pengiran Tengah et al. 2005).
Antibodies: anti-gliadin antibodies can also occur in patients with hereditary ataxias
One series of 50 patients reported the presence of anti-gliadin antibodies in 7/26 (27%) patients with sporadic ataxias, and 9/24 (37%) of patients with genetically confirmed autosomal dominant ataxias (Bushara, Goebel et al. 2001).
Antibodies: anti-transglutaminase-6 antibodies
Hadjivassiliou and colleagues reported that, “The prevalence of TG6 [transglutaminase-6] antibodies was 21 of 65 (32%) in idiopathic sporadic ataxia, 35 of 48 (73%) in GA, 16 of 50 (32%) in CD, 4 of 82 (5%) in neurology controls, and 2 of 57 (4%) in healthy controls” (Hadjivassiliou, Aeschlimann et al. 2013).
Notably, in gluten ataxia patients with anti-transglutaminase-6 antibodies, the ataxia can be present in the absence of any gastrointestinal symptoms (Hadjivassiliou, Aeschlimann et al. 2008).
Antibodies: anti-transglutaminase-6 antibodies occur in other diseases
Anti-transglutaminase-6 antibodies occur in other diseases as well (Ferlazzo, Polidoro et al. 2019). For example, anti-transglutaminase-6 antibodies have been reported in gluten sensitive patients with neuropathy (Zis, Rao et al. 2017).
Antibodies: anti-endomysial antibodies
Hadjivassiliou and colleagues report that anti-endomysial antibodies may be found in 22% of patients with gluten ataxia (Hadjivassiliou 2012).
Antibodies: anti-ganglioside antibodies
Several investigators have identified anti-ganglioside antibodies in patients with gluten ataxia (Shill, Alaedini et al. 2003, Volta, De Giorgio et al. 2006).
Imaging
Hadjivassiliou and colleagues reported that in a series of 68 patients with gluten ataxia, “MRI revealed atrophy of the cerebellum in 79% and white matter hyperintensities in 19%” (Hadjivassiliou, Grunewald et al. 2003).
It was recognized that even in the absence of cerebellar atrophy, patient with gluten ataxia could still exhibit metabolic abnormalities in the cerebellum detectable on magnetic resonance spectroscopy (MRS) (Wilkinson, Hadjivassiliou et al. 2005). Hadjivassiliou and colleagues reported that “up to 60% of patients with gluten ataxia have evidence of cerebellar atrophy on MR imaging” (Hadjivassiliou, Sanders et al. 2010), but on MRS “all patients have spectroscopic abnormalities primarily affecting the vermis” (Hadjivassiliou, Sanders et al. 2015), suggesting that, “MRS abnormalities and atrophy do not necessarily occur concurrently” (Hadjivassiliou, Wallis et al. 2012).
These metabolic abnormalities on MR spectroscopy can improve in patients who maintain a strict gluten-free diet (Hadjivassiliou, Grunewald et al. 2017, Hadjivassiliou, Grunewald et al. 2018).
Histopathology
Clark (Clark 2022) reviewed multiple cases and autopsy series of patients with gluten ataxia (in some cases with other neurological symptoms as well). He concluded that, “Nearly all patients studied at autopsy had significant loss of Purkinje neurons with Bergmann gliosis. The other commonly affected targets were cerebellar granular neurons, inferior olivary neurons, and cerebellar nuclei.”
Prognosis
Similar to other untreated autoimmune cerebellar ataxias, gluten ataxia tends to appear insidiously and progress relatively slowly (Newrick, Hoggard et al. 2021), though there are also reports of more rapid progression (Hermaszewski, Rigby et al. 1991).
Treatment
The mainstay of therapy is initiating and maintaining a gluten-free diet. Second-line therapies include intravenous immunoglobulin, plasmapheresis, corticosteroids or other immunosuppressants. Since autoimmune disease brings about neuronal damage and neuronal death, some researchers reasonably maintain the position that “time is brain” or “time is cerebellum” (Mitoma, Manto et al. 2017) and therefore suggest that treatment be initiated as early as possible (Mitoma, Manto et al. 2019).
Treatment: dietary restriction
For patients with gluten sensitivity, including gluten ataxia, several studies report improvement in at least some symptoms (Hadjivassiliou, Davies-Jones et al. 2003, Aljada, Zohni et al. 2021).
In gluten-sensitive patients with neurological symptoms, eliminating gluten from the diet may bring about improvement in some of the neurological symptoms, but not others. For example, in patients with gluten sensitivity who exhibit both ataxia and neuropathy, maintaining a strict gluten-free diet may improve both symptoms (Mearns, Taylor et al. 2019), or only the neuropathy but not the ataxia (Anandacoomaraswamy, Ullal et al. 2008).
There has been considerable media attention directed towards the putative ills of gluten and the putative benefits of a gluten-free diet.
A gluten-free diet has achieved some popularity among health faddists (Palmieri, Vadala et al. 2019), which in the United States has been promoted through the media by commercial interests, and this has given rise to spurious claims of health benefits based on little or no evidence. It is important to keep in mind that a gluten-free diet is not without risk. For example, maintaining a strict gluten-free diet increases the risk of certain nutritional deficiencies (Aljada, Zohni et al. 2021). Marketing of gluten-free products often downplays their disadvantages (Khairuddin and Lasekan 2021). Thus the “intervention” of initiating and maintaining a gluten-free diet should not be taken lightly; if there is reasonable evidence that a patient’s symptoms can be confidently connected to gluten, then dietary modification is sensible, but invoking a gluten-free diet in an individual with no evidence of gluten-related disease for purposes of prophylaxis or on the basis of poorly articulated “health benefits” should be discouraged (Niland and Cash 2018).
Gluten is found primarily in wheat products, but also in other grains. In the United States food labeling regulations from the Food and Drug Administration have made it somewhat easier to distinguish gluten-containing foods from gluten-free foods in a supermarket, and some restaurants will also clarify the gluten content of foods on their menus. Given the discussion above regarding the nutritional risks of maintaining a gluten-free diet, if a patient is considering instituting a gluten-free diet, it is sensible to consult a medical dietician or nutritionist to make sure that the patient can maintain a diet that is gluten-free yet still provides adequate nutrition in other respects.
Treatment: other methods
Less well-studied interventions of gluten ataxia include intravenous immunoglobulin (Burk, Melms et al. 2001, Nanri, Okita et al. 2009), plasmapheresis (Mitoma, Manto et al. 2019) corticosteroids and other immunosuppressants (Mitoma, Hadjivassiliou et al. 2015). These are generally regarded as second-line therapies, and there are no clear guidelines regarding when to consider them. Hadjivassiliou and colleagues (Hadjivassiliou 2012) suggest, “Treatment with immunosuppressants and intravenous immunoglobulins could be considered if a strict gluten-free diet for at least a year has not resulted in any improvement of the ataxia or if the ataxia is rapidly progressive.”
References
Abele M, Schols L, Schwartz S, Klockgether T (2003) Prevalence of antigliadin antibodies in ataxia patients. Neurology 60: 1674-5. doi: 10.1212/01.wnl.0000069606.82919.04
Alaedini A, Okamoto H, Briani C, Wollenberg K, Shill HA, Bushara KO, Sander HW, Green PH, Hallett M, Latov N (2007) Immune cross-reactivity in celiac disease: anti-gliadin antibodies bind to neuronal synapsin I. J Immunol 178: 6590-5. doi: 10.4049/jimmunol.178.10.6590
Aljada B, Zohni A, El-Matary W (2021) The Gluten-Free Diet for Celiac Disease and Beyond. Nutrients 13. doi: 10.3390/nu13113993
Anandacoomaraswamy D, Ullal J, Vinik AI (2008) A 70-year-old male with peripheral neuropathy, ataxia and antigliadin antibodies shows improvement in neuropathy, but not ataxia, after intravenous immunoglobulin and gluten-free diet. J Multidiscip Healthc 1: 93-6. doi: 10.2147/jmdh.s3018
Burk K, Bosch S, Muller CA, Melms A, Zuhlke C, Stern M, Besenthal I, Skalej M, Ruck P, Ferber S, Klockgether T, Dichgans J (2001a) Sporadic cerebellar ataxia associated with gluten sensitivity. Brain 124: 1013-9. doi: 10.1093/brain/124.5.1013
Burk K, Melms A, Schulz JB, Dichgans J (2001b) Effectiveness of intravenous immunoglobin therapy in cerebellar ataxia associated with gluten sensitivity. Ann Neurol 50: 827-8. doi: 10.1002/ana.1281
Bushara KO, Goebel SU, Shill H, Goldfarb LG, Hallett M (2001) Gluten sensitivity in sporadic and hereditary cerebellar ataxia. Ann Neurol 49: 540-3.
Charcot J-M (1868) Séance du 14 mars. CR Soc Biol (Paris) 20: 13.
Clark HB (2022) The Neuropathology of Autoimmune Ataxias. Brain Sci 12. doi: 10.3390/brainsci12020257
Cooke WT, Smith WT (1966) Neurological disorders associated with adult coeliac disease. Brain 89: 683-722. doi: 10.1093/brain/89.4.683
Currie S, Hoggard N, Clark MJ, Sanders DS, Wilkinson ID, Griffiths PD, Hadjivassiliou M (2013) Alcohol induces sensitization to gluten in genetically susceptible individuals: a case control study. PLoS One 8: e77638. doi: 10.1371/journal.pone.0077638
Dicke WK, Weijers HA, Van De Kamer JH (1953) Coeliac disease. II. The presence in wheat of a factor having a deleterious effect in cases of coeliac disease. Acta Paediatr (Stockh) 42: 34-42. doi: 10.1111/j.1651-2227.1953.tb05563.x
Ferlazzo E, Polidoro S, Gobbi G, Gasparini S, Sueri C, Cianci V, Sofia V, Giuliano L, Giallonardo AT, Di Bonaventura C, Casciato S, Messana T, Coppola A, Striano S, Bilo L, Monoriti M, Genovese G, Sarica P, Arcudi L, Aguglia U (2019) Epilepsy, cerebral calcifications, and gluten-related disorders: Are anti-transglutaminase 6 antibodies the missing link? Seizure 73: 17-20. doi: 10.1016/j.seizure.2019.10.012
Gordon N (2000) Cerebellar ataxia and gluten sensitivity: a rare but possible cause of ataxia, even in childhood. Dev Med Child Neurol 42: 283-6. doi: 10.1017/s0012162200000499
Green PH, Alaedini A, Sander HW, Brannagan TH, 3rd, Latov N, Chin RL (2005) Mechanisms underlying celiac disease and its neurologic manifestations. Cell Mol Life Sci 62: 791-9. doi: 10.1007/s00018-004-4109-9
Guan WJ, Liu XJ, Tang BS, Liu YT, Zhou Y, Jiang H, Shen L, Xia K, Wang JL (2013) Gluten ataxia of sporadic and hereditary cerebellar ataxia in patients from mainland China. Neurol India 61: 226-30. doi: 10.4103/0028-3886.115056
Hadjivassiliou M (2012) Immune-mediated acquired ataxias. Handb Clin Neurol 103: 189-99. doi: 10.1016/B978-0-444-51892-7.00011-5
Hadjivassiliou M, Aeschlimann P, Sanders DS, Maki M, Kaukinen K, Grunewald RA, Bandmann O, Woodroofe N, Haddock G, Aeschlimann DP (2013) Transglutaminase 6 antibodies in the diagnosis of gluten ataxia. Neurology 80: 1740-5. doi: 10.1212/WNL.0b013e3182919070
Hadjivassiliou M, Aeschlimann P, Strigun A, Sanders DS, Woodroofe N, Aeschlimann D (2008a) Autoantibodies in gluten ataxia recognize a novel neuronal transglutaminase. Ann Neurol 64: 332-43. doi: 10.1002/ana.21450
Hadjivassiliou M, Boscolo S, Davies-Jones GA, Grunewald RA, Not T, Sanders DS, Simpson JE, Tongiorgi E, Williamson CA, Woodroofe NM (2002) The humoral response in the pathogenesis of gluten ataxia. Neurology 58: 1221-6. doi: 10.1212/wnl.58.8.1221
Hadjivassiliou M, Davies-Jones GA, Sanders DS, Grunewald RA (2003a) Dietary treatment of gluten ataxia. J Neurol Neurosurg Psychiatry 74: 1221-4. doi: 10.1136/jnnp.74.9.1221
Hadjivassiliou M, Duker AP, Sanders DS (2014) Gluten-related neurologic dysfunction. Handb Clin Neurol 120: 607-19. doi: 10.1016/B978-0-7020-4087-0.00041-3
Hadjivassiliou M, Grunewald R, Sharrack B, Sanders D, Lobo A, Williamson C, Woodroofe N, Wood N, Davies-Jones A (2003b) Gluten ataxia in perspective: epidemiology, genetic susceptibility and clinical characteristics. Brain 126: 685-91. doi: 10.1093/brain/awg050
Hadjivassiliou M, Grunewald RA, Chattopadhyay AK, Davies-Jones GA, Gibson A, Jarratt JA, Kandler RH, Lobo A, Powell T, Smith CM (1998) Clinical, radiological, neurophysiological, and neuropathological characteristics of gluten ataxia. Lancet 352: 1582-5. doi: 10.1016/s0140-6736(98)05342-2
Hadjivassiliou M, Grunewald RA, Lawden M, Davies-Jones GA, Powell T, Smith CM (2001) Headache and CNS white matter abnormalities associated with gluten sensitivity. Neurology 56: 385-8. doi: 10.1212/wnl.56.3.385
Hadjivassiliou M, Grunewald RA, Sanders DS, Shanmugarajah P, Hoggard N (2017a) Effect of gluten-free diet on cerebellar MR spectroscopy in gluten ataxia. Neurology 89: 705-709. doi: 10.1212/WNL.0000000000004237
Hadjivassiliou M, Grunewald RA, Sanders DS, Zis P, Croal I, Shanmugarajah PD, Sarrigiannis PG, Trott N, Wild G, Hoggard N (2018) The Significance of Low Titre Antigliadin Antibodies in the Diagnosis of Gluten Ataxia. Nutrients 10. doi: 10.3390/nu10101444
Hadjivassiliou M, Grupsilonnewald RA (2022) Gluten Ataxia: an Underdiagnosed Condition. Cerebellum 21: 620-622. doi: 10.1007/s12311-021-01270-7
Hadjivassiliou M, Maki M, Sanders DS, Williamson CA, Grunewald RA, Woodroofe NM, Korponay-Szabo IR (2006) Autoantibody targeting of brain and intestinal transglutaminase in gluten ataxia. Neurology 66: 373-7. doi: 10.1212/01.wnl.0000196480.55601.3a
Hadjivassiliou M, Manto M, Mitoma H (2022) Rare Etiologies in Immune-Mediated Cerebellar Ataxias: Diagnostic Challenges. Brain Sci 12. doi: 10.3390/brainsci12091165
Hadjivassiliou M, Martindale J, Shanmugarajah P, Grunewald RA, Sarrigiannis PG, Beauchamp N, Garrard K, Warburton R, Sanders DS, Friend D, Duty S, Taylor J, Hoggard N (2017b) Causes of progressive cerebellar ataxia: prospective evaluation of 1500 patients. J Neurol Neurosurg Psychiatry 88: 301-309. doi: 10.1136/jnnp-2016-314863
Hadjivassiliou M, Sanders DD, Aeschlimann DP (2015) Gluten-related disorders: gluten ataxia. Dig Dis 33: 264-268. doi: 10.1159/000369509
Hadjivassiliou M, Sanders DS, Grunewald RA, Woodroofe N, Boscolo S, Aeschlimann D (2010) Gluten sensitivity: from gut to brain. Lancet Neurol 9: 318-30. doi: 10.1016/S1474-4422(09)70290-X
Hadjivassiliou M, Sanders DS, Woodroofe N, Williamson C, Grunewald RA (2008b) Gluten ataxia. Cerebellum 7: 494-8. doi: 10.1007/s12311-008-0052-x
Hadjivassiliou M, Wallis LI, Hoggard N, Grunewald RA, Griffiths PD, Wilkinson ID (2012) MR spectroscopy and atrophy in Gluten, Friedreich’s and SCA6 ataxias. Acta Neurol Scand 126: 138-43. doi: 10.1111/j.1600-0404.2011.01620.x
Hermaszewski RA, Rigby S, Dalgleish AG (1991) Coeliac disease presenting with cerebellar degeneration. Postgrad Med J 67: 1023-4. doi: 10.1136/pgmj.67.793.1023
Ihara M, Makino F, Sawada H, Mezaki T, Mizutani K, Nakase H, Matsui M, Tomimoto H, Shimohama S (2006) Gluten sensitivity in Japanese patients with adult-onset cerebellar ataxia. Intern Med 45: 135-40. doi: 10.2169/internalmedicine.45.1351
Jain D, Bhaduri G, Giri K, Balania V, Jain P (2019) Underlying coeliac disease in a case of cerebellar ataxia with unknown etiology. Arch Clin Cases 6: 22-25. doi: 10.22551/2019.22.0601.10149
Khairuddin MAN, Lasekan O (2021) Gluten-Free Cereal Products and Beverages: A Review of Their Health Benefits in the Last Five Years. Foods 10. doi: 10.3390/foods10112523
Kheder A, Currie S, Romanowski C, Hadjivassiliou M (2012) Progressive ataxia with palatal tremor due to gluten sensitivity. Mov Disord 27: 62-3. doi: 10.1002/mds.23987
Liu CS, Soong BW, Lee YC, Chen WL, Kuo CL, Cheng WL, Huang CS, Lin WT (2010) Gluten sensitivity: associated sporadic cerebellar ataxia in Taiwan. Acta Neurol Taiwan 19: 263-9.
Lock RJ, Pengiran Tengah DS, Unsworth DJ, Ward JJ, Wills AJ (2005) Ataxia, peripheral neuropathy, and anti-gliadin antibody. Guilt by association? J Neurol Neurosurg Psychiatry 76: 1601-3. doi: 10.1136/jnnp.2004.058487
Lock RJ, Tengah DP, Williams AJ, Ward JJ, Bingley PJ, Wills AJ, Unsworth DJ (2006) Cerebellar ataxia, peripheral neuropathy, “gluten sensitivity” and anti-neuronal autoantibodies. Clin Lab 52: 589-92.
Makhlouf S, Messelmani M, Zaouali J, Mrissa R (2018) Cognitive impairment in celiac disease and non-celiac gluten sensitivity: review of literature on the main cognitive impairments, the imaging and the effect of gluten free diet. Acta Neurol Belg 118: 21-27. doi: 10.1007/s13760-017-0870-z
Mearns ES, Taylor A, Thomas Craig KJ, Puglielli S, Leffler DA, Sanders DS, Lebwohl B, Hadjivassiliou M (2019) Neurological Manifestations of Neuropathy and Ataxia in Celiac Disease: A Systematic Review. Nutrients 11. doi: 10.3390/nu11020380
Meira AT, Franklin GL, Ferreira MG, Martinez ARM, Franca MC, Jr., Pedroso JL, Barsottini OGP, Teive HAG (2022) Gluten Ataxia: an Overestimated Condition? Cerebellum 21: 617-619. doi: 10.1007/s12311-021-01269-0
Mitoma H, Adhikari K, Aeschlimann D, Chattopadhyay P, Hadjivassiliou M, Hampe CS, Honnorat J, Joubert B, Kakei S, Lee J, Manto M, Matsunaga A, Mizusawa H, Nanri K, Shanmugarajah P, Yoneda M, Yuki N (2016) Consensus Paper: Neuroimmune Mechanisms of Cerebellar Ataxias. Cerebellum 15: 213-32. doi: 10.1007/s12311-015-0664-x
Mitoma H, Hadjivassiliou M, Honnorat J (2015) Guidelines for treatment of immune-mediated cerebellar ataxias. Cerebellum Ataxias 2: 14. doi: 10.1186/s40673-015-0034-y
Mitoma H, Manto M, Hadjivassiliou M (2021) Immune-Mediated Cerebellar Ataxias: Clinical Diagnosis and Treatment Based on Immunological and Physiological Mechanisms. J Mov Disord 14: 10-28. doi: 10.14802/jmd.20040
Mitoma H, Manto M, Hampe CS (2017) Immune-mediated cerebellar ataxias: from bench to bedside. Cerebellum Ataxias 4: 16. doi: 10.1186/s40673-017-0073-7
Mitoma H, Manto M, Hampe CS (2019) Immune-mediated Cerebellar Ataxias: Practical Guidelines and Therapeutic Challenges. Curr Neuropharmacol 17: 33-58. doi: 10.2174/1570159X16666180917105033
Nanri K, Okita M, Takeguchi M, Taguchi T, Ishiko T, Saito H, Otsuka T, Mitoma H, Koizumi K (2009) Intravenous immunoglobulin therapy for autoantibody-positive cerebellar ataxia. Intern Med 48: 783-90. doi: 10.2169/internalmedicine.48.1802
Newrick L, Hoggard N, Hadjivassiliou M (2021) Recognition and management of rapid-onset gluten ataxias: case series. Cerebellum Ataxias 8: 16. doi: 10.1186/s40673-021-00139-z
Niland B, Cash BD (2018) Health Benefits and Adverse Effects of a Gluten-Free Diet in Non-Celiac Disease Patients. Gastroenterol Hepatol (N Y) 14: 82-91.
Osman D, Umar S, Muhammad H, Nikfekr E, Rostami K, Ishaq S (2021) Neurological manifestation of coeliac disease with particular emphasis on gluten ataxia and immunological injury: a review article. Gastroenterol Hepatol Bed Bench 14: 1-7.
Palmieri B, Vadala M, Laurino C (2019) Gluten-free diet in non-celiac patients: beliefs, truths, advantages and disadvantages. Minerva Gastroenterol Dietol 65: 153-162. doi: 10.23736/S1121-421X.18.02519-9
Pellecchia MT, Scala R, Perretti A, De Michele G, Santoro L, Filla A, Ciacci C, Barone P (1999) Cerebellar ataxia associated with subclinical celiac disease responding to gluten-free diet. Neurology 53: 1606-8. doi: 10.1212/wnl.53.7.1606-a
Rashtak S, Rashtak S, Snyder MR, Pittock SJ, Wu TT, Gandhi MJ, Murray JA (2011) Serology of celiac disease in gluten-sensitive ataxia or neuropathy: role of deamidated gliadin antibody. J Neuroimmunol 230: 130-4. doi: 10.1016/j.jneuroim.2010.09.024
Rodrigo L, Hernandez-Lahoz C, Lauret E, Rodriguez-Pelaez M, Soucek M, Ciccocioppo R, Kruzliak P (2016) Gluten ataxia is better classified as non-celiac gluten sensitivity than as celiac disease: a comparative clinical study. Immunol Res 64: 558-64. doi: 10.1007/s12026-015-8750-1
Sarrigiannis PG, Hoggard N, Aeschlimann D, Sanders DS, Grunewald RA, Unwin ZC, Hadjivassiliou M (2014) Myoclonus ataxia and refractory coeliac disease. Cerebellum Ataxias 1: 11. doi: 10.1186/2053-8871-1-11
Serratrice J, Attarian S, Disdier P, Weiller PJ, Serratrice G (2004) Neuromuscular diseases associated with antigliadin antibodies. A contentious concept. Acta Myol 23: 146-50.
Shill HA, Alaedini A, Bushara KO, Latov N, Hallett M (2003) Anti-ganglioside antibodies in idiopathic and hereditary cerebellar degeneration. Neurology 60: 1672-3. doi: 10.1212/01.wnl.0000060185.30001.46
Volta U, De Giorgio R, Granito A, Stanghellini V, Barbara G, Avoni P, Liguori R, Petrolini N, Fiorini E, Montagna P, Corinaldesi R, Bianchi FB (2006) Anti-ganglioside antibodies in coeliac disease with neurological disorders. Dig Liver Dis 38: 183-7. doi: 10.1016/j.dld.2005.11.013
Wilkinson ID, Hadjivassiliou M, Dickson JM, Wallis L, Grunewald RA, Coley SC, Widjaja E, Griffiths PD (2005) Cerebellar abnormalities on proton MR spectroscopy in gluten ataxia. J Neurol Neurosurg Psychiatry 76: 1011-3. doi: 10.1136/jnnp.2004.049809
Wong D, Dwinnel M, Schulzer M, Nimmo M, Leavitt BR, Spacey SD (2007) Ataxia and the role of antigliadin antibodies. Can J Neurol Sci 34: 193-6. doi: 10.1017/s031716710000603x
Zis P, Rao DG, Sarrigiannis PG, Aeschlimann P, Aeschlimann DP, Sanders D, Grunewald RA, Hadjivassiliou M (2017) Transglutaminase 6 antibodies in gluten neuropathy. Dig Liver Dis 49: 1196-1200. doi: 10.1016/j.dld.2017.08.019
![]()