By Marcello Cherchi, MD PhD
For patients
Huntington’s disease (HD) is a familial neurological disorder that causes abnormal movements and problems with behavior and thinking. Most patients with HD also have abnormal eye movements. Imaging studies, such as MRI, usually show particular abnormalities in specific parts of the brain. The disease can be confirmed with genetic testing. There is no effective treatment.
For clinicians
Practical summary
Huntington’s disease (HD) is an autosomal dominant inherited movement disorder that manifests primarily with chorea, rigidity, and dementia. The majority of patients also have a variety of ocular motor disorders that may be most easily detected on instrumented testing; there is debate regarding whether the ocular motor abnormalities can effectively diagnose HD prior to the onset of motor symptoms, or be used to monitor progress of the disease. HD patients also exhibit abnormal performance on computerized dynamic posturography. Structural and functional imaging show abnormalities in the head of the caudate and striatum. HD is uniformly fatal; treatment is symptomatic; tetrabenzene and deutetrabenzene may modestly and transiently diminish chorea.
Introduction
Huntington’s disease (HD), also known as Huntington’s chorea, is a progressive neurodegenerative disorder affecting the basal ganglia and other structures in the central nervous system.
Vale and Cardoso (Vale and Cardoso 2015) state that Charles Oscar Waters published the first description of what was probably HD in 1841, but George Huntington provided a more complete description (Huntington 1872), and the disease is eponymously designated after him. Huntington’s original article was republished in 2003 (Huntington 2003). Wechsler (Wexler 2013) states that the phrase “Huntington’s chorea” first appeared in 1887 (Huber 1887).
Epidemiology
A systematic review and meta-analysis reported that the prevalence of HD is 2.71 per 100,000 people, and the incidence is 0.38 per 100,000 person-years (Medina et al. 2022).
Genetics
Huntington’s disease (OMIM 143100) is a heritable disorder transmitted in an autosomal dominant fashion. It results from a trinucleotide repeat (CAG) expansion in the Huntingtin gene, HTT (OMIM 613004), located on 4p16.3. Like other trinucleotide repeat diseases, the number of repeats usually expands with each generation, leading to anticipation (presentation of the disease earlier in life with each successive generation).
Pathophysiological mechanism of disease
Aggregates of abnormal huntingtin protein accumulate in the cytoplasm and nucleus of affected cells throughout the body, but predominantly in the central nervous system, and most prominently in the caudate and putamen. It is suspected that these protein aggregates are toxic to cellular function.
An autopsy study of the brains of four HD patients who had slow vertical saccades during life revealed abnormalities (reduced number of larger neurons in one patient, non-specific gliosis in three patients) in the rostral interstitial nucleus of the median longitudinal fasciculus, suggesting that this pathology is one underlying substrate for slowed vertical saccades (Leigh et al. 1985).
Clinical presentation
The initial manifestation of HD may be psychiatric or behavioral symptoms, which may precede other symptoms by 10 years. The other manifestations include motor (progressive chorea and rigidity) and cognitive decline (dementia), whose peak onset is in the fourth decade.
Physical examination
In a Huntington patient with no other diseases, physical examination shows chorea and rigidity.
Ocular motor examination
Face-to-face ocular motor examination may appear normal.
Testing: instrumented ocular motor testing
The majority of HD patients exhibit a variety of ocular motor abnormalities detectable on instrumented testing.
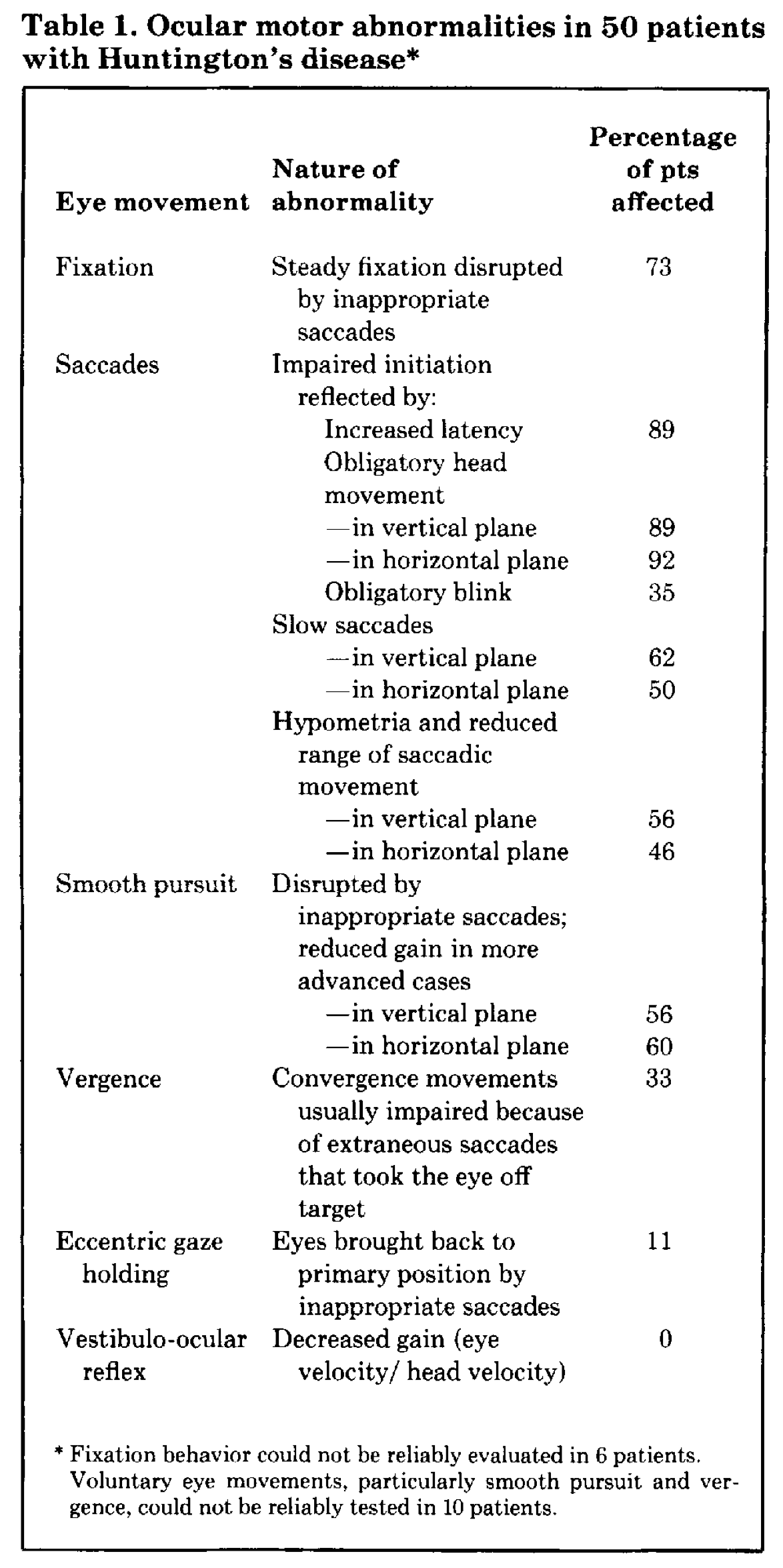
The Table below, from Leigh and colleagues (Leigh et al. 1983), provides a good overview of ocular motor abnormalities that can be observed in HD, and their relative frequency.
Although ocular motor abnormalities are common in HD, Beenen and colleagues noted that, “75% of the HD patients had pathologically slow saccades. This number rose to 87% if other ocular motor deficits were included. Thus a small, but definite number of HD patients had normal eye movements. This included patients with disease durations of more than 14 years” (Beenen, Büttner, Lange 1986).
A number of studies have explored ocular motor function in “presymptomatic” HD patients, which in this context generally refers to genetically confirmed HD individuals who have not yet developed motor symptoms. Many researchers have observed ocular motor abnormalities in these presymptomatic HD patients (Ali et al. 2006; Antoniades et al. 2007; Blekher et al. 2006; Blekher et al. 2004; Hicks et al. 2008; Robert et al. 2009; Rupp et al. 2010; Vaca-Palomares et al. 2017). However, not all investigators have found this to be reliable; Collewijn and colleagues conducted scleral search coil studies in HD patients and their offspring compared to controls, and concluded that, “The material as a whole suggests that ocular motor dysfunction does not develop prior to, but concurrently with and as a part of generalized, progressive deterioration of motor control. The implication is that ocular motor screening of clinically healthy at-risk subjects does not reliably contribute to an earlier diagnosis of future HD” (Collewijn et al. 1988).
Some investigators have studied the ocular motor abnormalities in HD as a “biomarker” not just for diagnosis, but also for disease progression (Ali et al. 2006; Antoniades et al. 2010; Blekher et al. 2009; Grabska et al. 2014; Hicks et al. 2008; Patel et al. 2012; Peltsch et al. 2008; Robert et al. 2009; Rupp et al. 2010; Rupp et al. 2012; Vaca-Palomares et al. 2019; Vaca-Palomares et al. 2017; Winder and Roos 2018). While this may be merely of academic interest now, if therapies for HD become available in the future, then such ocular motor “biomarkers” would have the potential to quantify treatment efficacy.
While the ocular motor findings in HD are fascinating and have implications for the underlying neuroanatomical substrates (Fielding et al. 2006; Hicks et al. 2008; Lasker and Zee 1997; Lasker et al. 1987, 1988; Rupp et al. 2012; Tian et al. 1991b; Vaca-Palomares et al. 2019; Vaca-Palomares et al. 2017; Winograd-Gurvich et al. 2003), clinicians would not rely on such findings to secure the diagnosis.
Testing: other vestibular
Several abnormalities have been described in computerized dynamic posturography in HD patients (Beckmann et al. 2018; Fekete et al. 2012; Medina et al. 2013; Nanetti et al. 2018; Reilmann et al. 2012; Reyes et al. 2018; Salomonczyk et al. 2010; Tian et al. 1991a; Valade, Davous, Rondot 1984), including:
- Impaired postural control at the limits of stability (Medina et al. 2013).
- Greater postural sway (Salomonczyk et al. 2010), resulting in poor performance on all conditions of sensory organization testing (Reyes et al. 2018).
- Increased latencies on motor control testing (Tian et al. 1991a).
Testing: other
A diagnosis of HD is confirmed by genetic testing which reveals more than 36 trinucleotide repeats in the HTT gene.
Imaging
Brain imaging has been studied extensively in HD (Johnson and Gregory 2019), both in structural (Wilson, Dervenoulas, Politis 2018) and functional (Gregory and Scahill 2018) modalities. Broadly, structural imaging shows atrophy of the caudate head; functional imaging shows reduced metabolic activity in the striatum.
Differential diagnosis
The differential diagnosis of HD includes other basal ganglionic disorders.
Treatment
If a diagnosis of HD is being entertained, a patient should strongly consider consultation with a genetic counselor.
There is no curative or arrestive therapy for HD. Treatment is symptomatic. Tetrabenzene and deutetrabenzene may modestly and transiently diminish chorea.
Tetrabenzene has been reported to improve performance on computerized dynamic posturography in sensory organization testing in which a single modality (either vision or proprioception) is sway-referenced (Fekete et al. 2012).
Deep brain stimulation (DBS) has been studied for a variety of movement disorders, including HD. Fawcett and colleagues reported that pallidal DBS improved some ocular motor abnormalities; specifically, “Pallidal DBS decreased pro-saccade latency, total movement time, and the number of correctly executed trials, as well as increasing saccade gain” (Fawcett et al. 2005).
Prognosis
HD is uniformly fatal. From the time that motor symptoms become manifest, death occurs on average within 17 years.
References
Ali FR, Michell AW, Barker RA, Carpenter RH (2006) The use of quantitative oculometry in the assessment of Huntington’s disease. Exp Brain Res 169: 237-45. doi: 10.1007/s00221-005-0143-6
Antoniades CA, Altham PM, Mason SL, Barker RA, Carpenter R (2007) Saccadometry: a new tool for evaluating presymptomatic Huntington patients. Neuroreport 18: 1133-6. doi: 10.1097/WNR.0b013e32821c560d
Antoniades CA, Xu Z, Mason SL, Carpenter RH, Barker RA (2010) Huntington’s disease: changes in saccades and hand-tapping over 3 years. J Neurol 257: 1890-8. doi: 10.1007/s00415-010-5632-2
Beckmann H, Bohlen S, Saft C, Hoffmann R, Gerss J, Muratori L, Ringelstein EB, Landwehrmeyer GB, Reilmann R (2018) Objective assessment of gait and posture in premanifest and manifest Huntington disease – A multi-center study. Gait Posture 62: 451-457. doi: 10.1016/j.gaitpost.2018.03.039
Beenen N, Büttner U, Lange HW (1986) The diagnostic value of eye movement recordings in patients with Huntington’s disease and their offspring. Electroencephalogr Clin Neurophysiol 63: 119-27. doi: 10.1016/0013-4694(86)90005-2
Blekher T, Johnson SA, Marshall J, White K, Hui S, Weaver M, Gray J, Yee R, Stout JC, Beristain X, Wojcieszek J, Foroud T (2006) Saccades in presymptomatic and early stages of Huntington disease. Neurology 67: 394-9. doi: 10.1212/01.wnl.0000227890.87398.c1
Blekher T, Weaver MR, Cai X, Hui S, Marshall J, Jackson JG, Wojcieszek J, Yee RD, Foroud TM (2009) Test-retest reliability of saccadic measures in subjects at risk for Huntington disease. Invest Ophthalmol Vis Sci 50: 5707-11. doi: 10.1167/iovs.09-3538
Blekher TM, Yee RD, Kirkwood SC, Hake AM, Stout JC, Weaver MR, Foroud TM (2004) Oculomotor control in asymptomatic and recently diagnosed individuals with the genetic marker for Huntington’s disease. Vision Res 44: 2729-36. doi: 10.1016/j.visres.2004.06.006
Collewijn H, Went LN, Tamminga EP, Vegter-Van der Vlis M (1988) Oculomotor defects in patients with Huntington’s disease and their offspring. J Neurol Sci 86: 307-20. doi: 10.1016/0022-510x(88)90107-4
Fawcett AP, Moro E, Lang AE, Lozano AM, Hutchison WD (2005) Pallidal deep brain stimulation influences both reflexive and voluntary saccades in Huntington’s disease. Mov Disord 20: 371-7. doi: 10.1002/mds.20356
Fekete R, Davidson A, Ondo WG, Cohen HS (2012) Effect of tetrabenazine on computerized dynamic posturography in Huntington disease patients. Parkinsonism Relat Disord 18: 896-8. doi: 10.1016/j.parkreldis.2012.04.029
Fielding J, Georgiou-Karistianis N, Millist L, Fahey M, White O (2006) Saccadic trajectory in Huntington’s disease. J Int Neuropsychol Soc 12: 455-64. doi: 10.1017/s1355617706060589
Grabska N, Rudzińska M, Wójcik-Pędziwiatr M, Michalski M, Sławek J, Szczudlik A (2014) Saccadic eye movements in juvenile variant of Huntington disease. Neurol Neurochir Pol 48: 236-41. doi: 10.1016/j.pjnns.2014.06.003
Gregory S, Scahill RI (2018) Functional Magnetic Resonance Imaging in Huntington’s Disease. Int Rev Neurobiol 142: 381-408. doi: 10.1016/bs.irn.2018.09.013
Hicks SL, Robert MP, Golding CV, Tabrizi SJ, Kennard C (2008) Oculomotor deficits indicate the progression of Huntington’s disease. Prog Brain Res 171: 555-8. doi: 10.1016/s0079-6123(08)00678-x
Huber A (1887) Chorea hereditaria er Erwachsenen. Virchow’s Archiv für pathologische Anatomie 108: 267-285.
Huntington G (1872) On chorea. The Medical and Surgical Reporter of Philadelphia 26: 317-321.
Huntington G (2003) On chorea. George Huntington, M.D. J Neuropsychiatry Clin Neurosci 15: 109-12. doi: 10.1176/jnp.15.1.109
Johnson EB, Gregory S (2019) Huntington’s disease: Brain imaging in Huntington’s disease. Prog Mol Biol Transl Sci 165: 321-369. doi: 10.1016/bs.pmbts.2019.04.004
Lasker AG, Zee DS (1997) Ocular motor abnormalities in Huntington’s disease. Vision Res 37: 3639-45. doi: 10.1016/s0042-6989(96)00169-1
Lasker AG, Zee DS, Hain TC, Folstein SE, Singer HS (1987) Saccades in Huntington’s disease: initiation defects and distractibility. Neurology 37: 364-70. doi: 10.1212/wnl.37.3.364
Lasker AG, Zee DS, Hain TC, Folstein SE, Singer HS (1988) Saccades in Huntington’s disease: slowing and dysmetria. Neurology 38: 427-31. doi: 10.1212/wnl.38.3.427
Leigh RJ, Newman SA, Folstein SE, Lasker AG, Jensen BA (1983) Abnormal ocular motor control in Huntington’s disease. Neurology 33: 1268-75. doi: 10.1212/wnl.33.10.1268
Leigh RJ, Parhad IM, Clark AW, Buettner-Ennever JA, Folstein SE (1985) Brainstem findings in Huntington’s disease. Possible mechanisms for slow vertical saccades. J Neurol Sci 71: 247-56. doi: 10.1016/0022-510x(85)90063-2
Medina A, Mahjoub Y, Shaver L, Pringsheim T (2022) Prevalence and Incidence of Huntington’s Disease: An Updated Systematic Review and Meta-Analysis. Mov Disord 37: 2327-2335. doi: 10.1002/mds.29228
Medina LD, Pirogovsky E, Salomonczyk D, Goldstein J, Panzera R, Gluhm S, Simmons R, Corey-Bloom J, Gilbert PE (2013) Postural limits of stability in premanifest and manifest Huntington’s disease. J Huntingtons Dis 2: 177-84. doi: 10.3233/JHD-130048
Nanetti L, Contarino VE, Castaldo A, Sarro L, Bachoud-Levi AC, Giavazzi M, Frittoli S, Ciammola A, Rizzo E, Gellera C, Bruzzone MG, Taroni F, Grisoli M, Mariotti C (2018) Cortical thickness, stance control, and arithmetic skill: An exploratory study in premanifest Huntington disease. Parkinsonism Relat Disord 51: 17-23. doi: 10.1016/j.parkreldis.2018.02.033
Patel SS, Jankovic J, Hood AJ, Jeter CB, Sereno AB (2012) Reflexive and volitional saccades: biomarkers of Huntington disease severity and progression. J Neurol Sci 313: 35-41. doi: 10.1016/j.jns.2011.09.035
Peltsch A, Hoffman A, Armstrong I, Pari G, Munoz DP (2008) Saccadic impairments in Huntington’s disease. Exp Brain Res 186: 457-69. doi: 10.1007/s00221-007-1248-x
Reilmann R, Rumpf S, Beckmann H, Koch R, Ringelstein EB, Lange HW (2012) Huntington’s disease: objective assessment of posture–a link between motor and functional deficits. Mov Disord 27: 555-9. doi: 10.1002/mds.24908
Reyes A, Salomonczyk D, Teo WP, Medina LD, Bartlett D, Pirogovsky-Turk E, Zaenker P, Bloom JC, Simmons RW, Ziman M, Gilbert PE, Cruickshank T (2018) Computerised Dynamic Posturography in Premanifest and Manifest individuals with Huntington’s Disease. Sci Rep 8: 14615. doi: 10.1038/s41598-018-32924-y
Robert MP, Nachev PC, Hicks SL, Golding CV, Tabrizi SJ, Kennard C (2009) Saccadometry of conditional rules in presymptomatic Huntington’s disease. Ann N Y Acad Sci 1164: 444-50. doi: 10.1111/j.1749-6632.2008.03736.x
Rupp J, Blekher T, Jackson J, Beristain X, Marshall J, Hui S, Wojcieszek J, Foroud T (2010) Progression in prediagnostic Huntington disease. J Neurol Neurosurg Psychiatry 81: 379-84. doi: 10.1136/jnnp.2009.176982
Rupp J, Dzemidzic M, Blekher T, West J, Hui S, Wojcieszek J, Saykin AJ, Kareken DA, Foroud T (2012) Comparison of vertical and horizontal saccade measures and their relation to gray matter changes in premanifest and manifest Huntington disease. J Neurol 259: 267-76. doi: 10.1007/s00415-011-6172-0
Salomonczyk D, Panzera R, Pirogovosky E, Goldstein J, Corey-Bloom J, Simmons R, Gilbert PE (2010) Impaired postural stability as a marker of premanifest Huntington’s disease. Mov Disord 25: 2428-33. doi: 10.1002/mds.23309
Tian JR, Herdman SJ, Zee DS, Folstein SE (1991a) Postural control in Huntington’s disease (HD). Acta Otolaryngol Suppl 481: 333-6. doi: 10.3109/00016489109131415
Tian JR, Zee DS, Lasker AG, Folstein SE (1991b) Saccades in Huntington’s disease: predictive tracking and interaction between release of fixation and initiation of saccades. Neurology 41: 875-81. doi: 10.1212/wnl.41.6.875
Vaca-Palomares I, Brien DC, Coe BC, Ochoa-Morales A, Martínez-Ruano L, Munoz DP, Fernandez-Ruiz J (2019) Implicit learning impairment identified via predictive saccades in Huntington’s disease correlates with extended cortico-striatal atrophy. Cortex 121: 89-103. doi: 10.1016/j.cortex.2019.06.013
Vaca-Palomares I, Coe BC, Brien DC, Campos-Romo A, Munoz DP, Fernandez-Ruiz J (2017) Voluntary saccade inhibition deficits correlate with extended white-matter cortico-basal atrophy in Huntington’s disease. Neuroimage Clin 15: 502-512. doi: 10.1016/j.nicl.2017.06.007
Valade D, Davous P, Rondot P (1984) Comparative study of posturography and electrooculography in at-risk subjects for Huntington’s disease. Eur Neurol 23: 252-64. doi: 10.1159/000115739
Vale TC, Cardoso F (2015) Chorea: A Journey through History. Tremor and Other Hyperkinetic Movements. doi: 10.5334/tohm.275
Wexler A (2013) A brief prehistory of Huntington’s disease. J Huntingtons Dis 2: 231-7. doi: 10.3233/JHD-139006
Wilson H, Dervenoulas G, Politis M (2018) Structural Magnetic Resonance Imaging in Huntington’s Disease. Int Rev Neurobiol 142: 335-380. doi: 10.1016/bs.irn.2018.09.006
Winder JY, Roos RAC (2018) Premanifest Huntington’s disease: Examination of oculomotor abnormalities in clinical practice. PLoS One 13: e0193866. doi: 10.1371/journal.pone.0193866
Winograd-Gurvich CT, Georgiou-Karistianis N, Evans A, Millist L, Bradshaw JL, Churchyard A, Chiu E, White OB (2003) Hypometric primary saccades and increased variability in visually-guided saccades in Huntington’s disease. Neuropsychologia 41: 1683-92. doi: 10.1016/s0028-3932(03)00096-4
![]()