By Marcello Cherchi, MD PhD
For patients
Sudden sensorineural hearing loss (SSNHL) presents with abrupt-onset hearing loss, usually on one side, and sometimes with other ear symptoms such as fullness or tinnitus. In most cases it is helpful to quantify the hearing loss on formal audiometry. It is reasonable to attempt treatment with a course of oral steroids, and some otolaryngologists may also offer a transtympanic (through the eardrum) injection of steroids. If those treatments fail, then it is reasonable to consult an audiologist to be evaluated for amplification (such as a hearing aid).
For clinicians
Overview
Idiopathic sudden sensorineural hearing loss (SSNHL) is thought to be due to cochlear inflammation of uncertain etiology. Most cases present with unilateral hearing loss (typically greater in the high frequencies) and sometimes tinnitus. Treatment with oral or transtympanic steroids is often attempted, though the supporting data are weak.
What is sudden sensorineural hearing loss?
Idiopathic sudden sensorineural hearing loss (SSNHL), as its name suggests, sensorineural hearing loss, presenting acutely (over hours to a couple of days), and generally presenting unilaterally. Bilateral SSNHL appears to be a different disease entity.
What is the cause of SSNHL?
Idiopathic SSNHL is currently suspected to be due to an inflammatory-mediated insult (damage) to the “hearing component” (cochlea) of the inner ear, which technically should be termed “cochleitis,” though that term is seldom used (Sataloff and Vassallo 1968, Fitzgerald and Mark 1999, Luigetti, Cianfoni et al. 2011). However, damage to the auditory component of the vestibulocochlear nerve could manifest in a similar fashion clinically; this would be termed “cochlear neuritis.” Thus, distinguishing between sudden sensorineural hearing loss from “cochleitis” (inflammatory damage of the hearing-related components of the inner ear) and “cochlear neuritis” (inflammation of the hearing-related nerve) would be difficult (Goodale, Golub et al. 2016).
Most cases of idiopathic SSNHL present unilaterally. Bilateral SSNHL is much less common, and appears to be a different disease entity, with a differential diagnosis including toxic, autoimmune, neoplastic and vascular conditions (Sara, Teh et al. 2014). Some research has implicated genetic predisposition to bilateral SSNHL (Varga, Jovankovicova et al. 2019).
Demographics of SSNHL
Alexander and Harris (Alexander and Harris 2013) report that, “During 2006 and 2007, the annual incidence of SSNHL was 27 per 100,000 in the United States. The incidence increased with increasing age, ranging from 11 per 100,000 for patients younger than 18 years to 77 per 100,000 for patients 65 years and older. There was an overall slight male preponderance with a male-to-female ratio of 1.07:1. This was more pronounced in patients 65 years and older, with a ratio of 1.30:1.” The authors also criticize earlier estimates of incidence as suffering from sampling bias. Rausch (Rauch 2008) adds that the peak age of incidence is 43 – 53 years. Some studies report a slight male preponderance (Alexander and Harris 2013), while others report an equal distribution between genders (Rauch 2008).
How does SSNHL present?
Idiopathic SSNHL is usually unilateral, and presents acutely, typically over hours to a couple of days. A patient may experience the initial symptoms as aural fullness without perceiving loss of hearing. Tinnitus sometimes accompanies the hearing loss.
How is SSNHL diagnosed?
Idiopathic SSNHL is diagnosed based on a compatible clinical history, usually defined as hearing loss occurring over 24 – 72 hours. The criteria for audiometric confirmation usually require 30 dB of hearing loss in at least 3 contiguous frequencies (Alexander and Harris 2013). Note that this requires comparison to a pre-morbid baseline, and since often no such baseline is available, many practitioners instead look for asymmetry (of the required magnitude) between the two ears, assuming that pre-morbid hearing was symmetrical.
The idealized Figure below, from Rausch (Rauch 2008), shows an annotated audiogram compatible with a diagnosis of idiopathic SSNHL.

How is SSNHL treated?
Some practitioners attempt a course of oral steroids, even though the data supporting that approach are weak (Cinamon, Bendet et al. 2001, Nosrati-Zarenoe and Hultcrantz 2012, Wei, Stathopoulos et al. 2013). If that fails, referral to otolaryngology to be evaluated for a transtympanic injection of steroids (Garavello, Galluzzi et al. 2012) is sometimes considered, even though the evidence supporting that approach are also weak (Crane, Camilon et al. 2015, El Sabbagh, Sewitch et al. 2017).
If hearing with oral and/or oral steroids does not improve sufficiently after 4 – 6 months, and if the residual hearing loss is interfering with a patient’s level of function, then referral to audiology for amplification is appropriate.
What is the prognosis of SSNHL?
Idiopathic SSNHL may improve spontaneously to some degree over about 4 – 6 months. A common clinical practice is to perform a hearing test as close as possible to the beginning of the disease, and then repeat a hearing test at 4 – 6 months after symptom onset. If the hearing loss appears to have “plateaued,” then consultation with audiology is appropriate in order to discuss amplification options (such as a hearing aid) and perhaps masking strategies (if tinnitus is present).
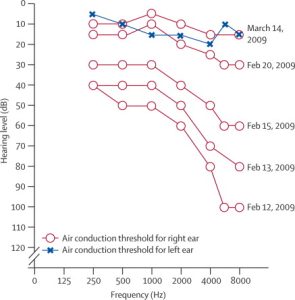
The Figure below shows a composite audiogram exhibiting spontaneous recovery from idiopathic sudden sensorineural hearing loss over approximately one month from Schreiber and colleagues (Schreiber, Agrup et al. 2010).
References
Alexander, T. H. and J. P. Harris (2013). “Incidence of sudden sensorineural hearing loss.” Otol Neurotol 34(9): 1586-1589.
Cinamon, U., E. Bendet and J. Kronenberg (2001). “Steroids, carbogen or placebo for sudden hearing loss: a prospective double-blind study.” Eur Arch Otorhinolaryngol 258(9): 477-480.
Crane, R. A., M. Camilon, S. Nguyen and T. A. Meyer (2015). “Steroids for treatment of sudden sensorineural hearing loss: a meta-analysis of randomized controlled trials.” Laryngoscope 125(1): 209-217.
El Sabbagh, N. G., M. J. Sewitch, A. Bezdjian and S. J. Daniel (2017). “Intratympanic dexamethasone in sudden sensorineural hearing loss: A systematic review and meta-analysis.” Laryngoscope 127(8): 1897-1908.
Fitzgerald, D. C. and A. S. Mark (1999). “Viral cochleitis with gadolinium enhancement of the cochlea on magnetic resonance imaging scan.” Otolaryngol Head Neck Surg 121(1): 130-132.
Garavello, W., F. Galluzzi, R. M. Gaini and D. Zanetti (2012). “Intratympanic steroid treatment for sudden deafness: a meta-analysis of randomized controlled trials.” Otol Neurotol 33(5): 724-729.
Goodale, A. D., J. S. Golub, R. S. Cornelius and R. N. Samy (2016). “Isolated cochlear neuritis from varicella reactivation mimicking a vestibular schwannoma.” World J Otorhinolaryngol Head Neck Surg 2(3): 181-184.
Luigetti, M., A. Cianfoni, A. Modoni, A. Conte, G. Conti and M. Sabatelli (2011). “Teaching NeuroImages: cochleitis: a rare cause of acute deafness in a patient with HCV.” Neurology 77(18): e109.
Nosrati-Zarenoe, R. and E. Hultcrantz (2012). “Corticosteroid treatment of idiopathic sudden sensorineural hearing loss: randomized triple-blind placebo-controlled trial.” Otol Neurotol 33(4): 523-531.
Rauch, S. D. (2008). “Clinical practice. Idiopathic sudden sensorineural hearing loss.” N Engl J Med 359(8): 833-840.
Sara, S. A., B. M. Teh and P. Friedland (2014). “Bilateral sudden sensorineural hearing loss: review.” J Laryngol Otol128 Suppl 1: S8-15.
Sataloff, J. and L. Vassallo (1968). “Head colds and viral cochleitis.” Arch Otolaryngol 87(1): 56-59.
Schreiber, B. E., C. Agrup, D. O. Haskard and L. M. Luxon (2010). “Sudden sensorineural hearing loss.” Lancet375(9721): 1203-1211.
Varga, L., A. Jovankovicova, M. Huckova, L. Demesova, D. Gasperikova, I. Sebova and M. Profant (2019). “Hereditary bilateral sudden sensorineural hearing loss.” Bratisl Lek Listy 120(9): 699-702.
Wei, B. P., D. Stathopoulos and S. O’Leary (2013). “Steroids for idiopathic sudden sensorineural hearing loss.” Cochrane Database Syst Rev 2013(7): CD003998.
![]()