By Marcello Cherchi, MD PhD
For patients
An inversion illusion or illusion of tilt is when you feel as if the world has flipped completely or partially upside-down or on its side. This is very rare. It is more common in men, and tends to begin when a person is in their 50s. Some brain diseases and ear diseases can cause this. If you have been experiencing this kind of illusion, then your doctor may consider checking some tests of inner ear function, or sending you to have brain imaging (usually an MRI) done.
For clinicians
Overview
An inversion illusion refers to the perception that the world has flipped 180 degrees in the coronal plane, but similar misperceptions of smaller angles or in different planes can also occur, so this problem can more generally be referred to as an illusion of tilt. Illusions of tilt are rare; they more commonly occur in males (60% – 66%), with a mean age of onset in the sixth decade, though with a broad range (12 – 85 years). The episodes are sometimes accompanied by nausea and/or vomiting. Physical examination sometimes shows various ocular motor abnormalities, gait ataxia, truncal ataxia, or other findings. The etiology is unknown, but is generally thought to arise either when actually conflicting peripheral inputs (visual, vestibular, somatosensory) cannot be reconciled, or a central disturbance fails to integrate inputs properly. In patients experiencing tilt illusions, a variety of anatomical localizations have been described from a range of central (neurologic) and peripheral (otologic) etiologies. An initial workup may include imaging (such as MRI of the brain and internal auditory canals without and with contrast) and otovestibular testing. Workup of an isolated (non-recurrent) episode sometimes reveals a “central” etiology such as ischemia/infarction of the brainstem or cerebellum. Etiologies of recurrent episodes include peripheral vestibular disease, migraine and seizure.
Introduction
Sierra-Hidalgo and colleagues (Sierra-Hidalgo et al. 2012) credit Bishopp (Bishopp 1805) as having published the first report of an inversion illusion in 1805. This phenomenon has been described under various terminologies, including:
- “Illusion of tilting of the visual environment” (Ropper 1983)
- “Inverted vision” (Solms et al. 1988)
- “Reversal of vision metamorphopsia” (River et al. 1998; Yap 2022)
- “Room tilt illusion” (Akdal et al. 2017; Horga Hernandez et al. 2006; Kirsch et al. 2017; Sierra-Hidalgo et al. 2012)
- “Upside-down reversal of vision” (Deniz et al. 2012; Horga Hernandez et al. 2006; Pamir et al. 1990)
- “Upside-down vision” (Charles et al. 1992; Solms et al. 1988)
- “Upside-down visual inversion” (Deniz et al. 2012; Okuyucu et al. 2008)
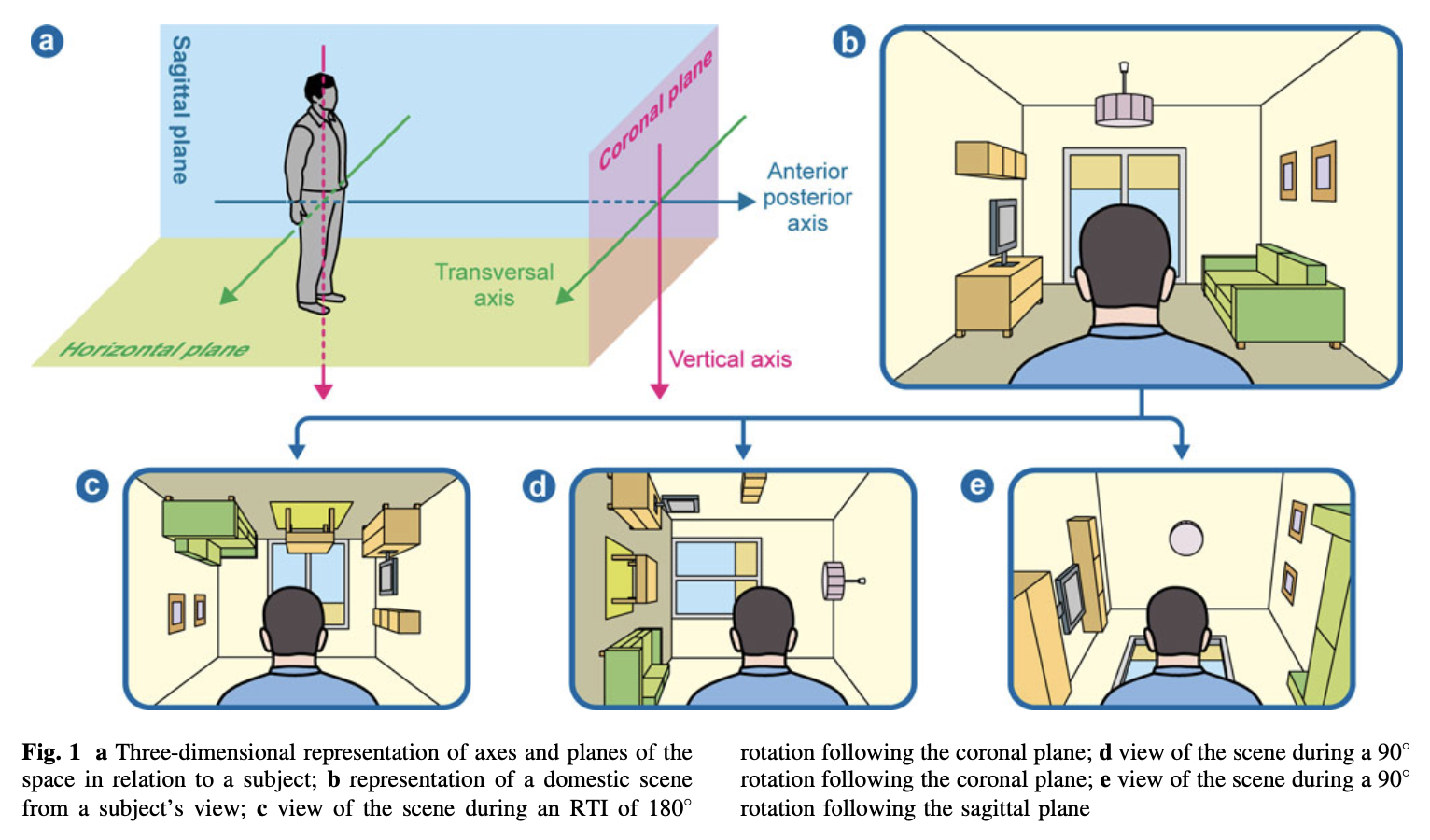
The illusion is often “complete inversion” (meaning a 180 degree flip) in the coronal plane, but it can be in other angles or in other planes — sometimes referred to as “oblique” (River et al. 1998). Many papers report that tilt illusions involve coronal rotations of 180 or 90 degrees, which has led some authors to conclude that, “Illusory rotations of the visual scene tend to be oriented along one of the principal orthogonals” (Solms et al. 1988). However, broader literature reviews conclude that many papers, “do not include the spectrum of manifestations of the RTI [room tilt illusion] phenomenon that may occur in a plane other than the coronal and/or in 90˚ steps” (Sierra-Hidalgo et al. 2012). For these reasons we prefer the phrase “tilt illusion” because it accommodates that the illusory perception of deviation from verticality can occur over a range, not only a complete inversion.
Sierra-Hidalgo and colleagues (Sierra-Hidalgo et al. 2012) provide the following Figure to illustrate the various misperceived orientations involved in tilt illusions.
Epidemiology
Tilt illusions are rare, and it is difficult to estimate their incidence or prevalence (Yap 2022).
In case series, most authors observe a male preponderance. Sierra-Hidalgo and colleagues (Sierra-Hidalgo et al. 2012) studied 135 cases and reported 60.2% were male. Yap conducted a literature review of 52 cases from 28 articles and reported that 66% of patients were male.
Sierra-Hidalgo and colleagues (Sierra-Hidalgo et al. 2012) reported the mean age at onset was 51.2 ± 20.3 years. Yap (Yap 2022) reported the mean age of onset to be 52.5 ± 20.2 years (range 12 – 85 years).
Pathophysiological mechanism of disease
“The perception of verticality is considered to be mediated by inputs from vestibular, somatosensory and visual symptoms and processed in the vestibular nuclei and then projected to the cortex via thalamic nuclei” (Akdal et al. 2017), and tilt illusions are usually, “attributed to an erroneous cortical mismatch of the visual and vestibular three-dimensional coordinate maps” (Sierra-Hidalgo et al. 2012), because, “lesions involving the necessary inputs to create a verticality perception” (Sierra-Hidalgo et al. 2012) result in “disintegration between vestibular, visual and somatosensory systems” (Akdal et al. 2017).
Most literature broadly agrees that tilt illusions can arise from both central and peripheral disorders (Akdal et al. 2017; Malis and Guyot 2003).
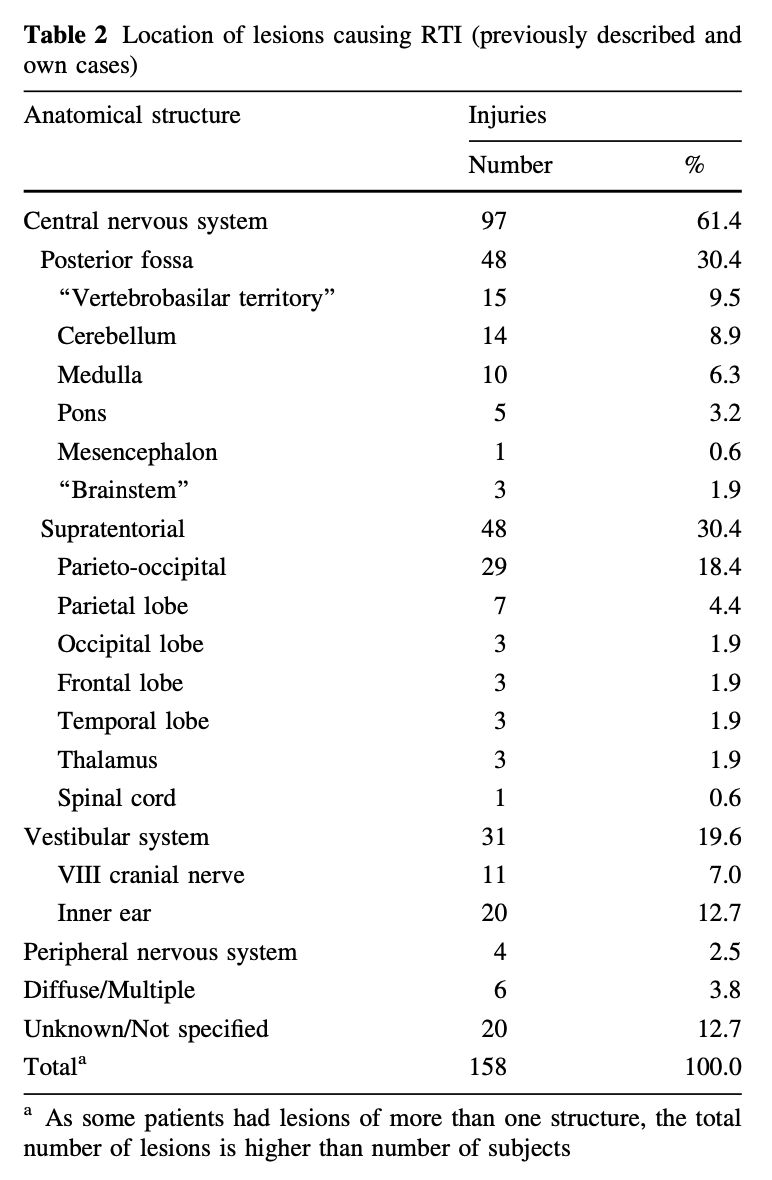
Sierra-Hidalgo and colleagues (Sierra-Hidalgo et al. 2012) studied 13 cases of their own patients with tilt illusions, as well as those from a review of the literature, amounting to a total of 135 cases. They provided the localization of tilt illusions in the following Table.
Kirsch and colleagues (Kirsch et al. 2017) studied functional connectivity MRI in a patient with recurrent tilt illusions and reported “bilateral changes of vestibular and visual cortex activity… during RTI” (room tilt illusions).
Note that tilt illusions, including complete (180˚) inversion illusions, can occur in healthy individuals during parabolic flight (Roberts 1973), in which case it is usually attributed to erroneous otolith signaling from zero gravity conditions (Graybiel and Kellogg 1967).
Clinical presentation
Episodes of tilt illusions are often isolated, but can be recurrent. In the series of 13 of their own patients, Sierra-Hidalgo and colleagues (Sierra-Hidalgo et al. 2012) reported that 8 (62%) “had two or more episodes,” and “only one patient [8%] suffered from recurrent RTI [room tilt illusions] for 1 year.”
The duration of tilt illusions is variable, lasting from seconds to hours. Yap reviewed 52 cases from 28 articles and reported the mean duration to be 16 minutes (Yap 2022).
Some authors report that during a tilt illusion patients will complain of feeling “dizzy” (Ropper 1983). Of the 52 cases reviewed by Yap (Yap 2022) they noted the following symptoms associated with the tilt illusion:
- “Vertigo” in 40%
- Vomiting in 25%
- Nausea in 23%
- “Dizziness” in 8%
Physical examination and ocular motor examination
Of the 52 cases reviewed by Yap (Yap 2022), 44% had a “normal clinical examination at the time of presentation.” Of those with physical examination findings, these included:
- Ocular motor and ophthalmological abnormalities:
- “Nystagmus” (not further specified) in 33%
- “Abnormal saccade” in 2%
- “Apraxia” in 2%
- Hemianopia in 2%
- Internuclear ophthalmoplegia in 2%
- “Gaze palsy” (not further specified) in 2%
- “Skew” (presumably vertical skew deviation) in 2%
- Ataxia in 23%, including:
- “Gait ataxia” in 8%
- Truncal ataxia in 8%
- “Abnormal sensory findings” (not further specified) in 14%
- “Weakness” (not further specified) in 8%
- “Abnormal reflexes” (not further specified) in 6%
- “Hearing deficits” (not further specified) in 4%
Testing: auditory
Very few studies report any audiologic testing in patients with tilt illusions. In one of the patients reported by Stracciari and colleagues, “Brainstem auditory evoked potentials (BAER) revealed increased latency of V wave on right stimulation” (Stracciari et al. 1993).
Testing: vestibular
Very few studies report on any audiologic or vestibular testing in patients with tilt illusions.
In the patient described by Kirsch and colleagues (Kirsch et al. 2017) they reported normal caloric testing.
Tiliket and colleagues studied 3 patients “with persistent skew deviation caused by a brain stem lesion” in whom “vestibular stimulation” elicited “a sudden 90 degrees room tilt illusion (RTI)” (Tiliket et al. 1996). They studied these 3 patients with rotatory chair testing, “including earth-vertical axis rotation for canal stimulation and off-vertical axis rotation (OVAR) for otolith stimulation. Measurement of the subjective visual vertical (SVV) was also performed.” They reported that, “The otolith-ocular reflex registered by OVAR was impaired in the 3 patients with skew deviation and the SVV in 2 patients.”
Imaging
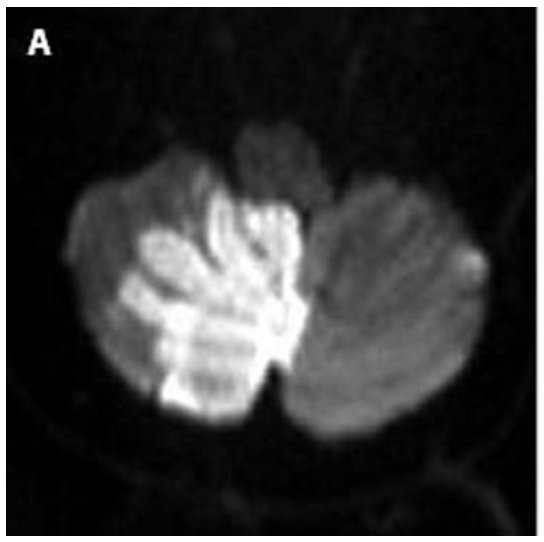
Imaging findings are as variable as the etiologies. A straightforward case of an acute right medial cerebellar infarct in the territory of the right posterior inferior cerebellar artery was reported as the etiology of a tilt illusion in the case described by Horga Hernandez and colleagues (Horga Hernandez et al. 2006), as shown in the Figure below.
Differential diagnosis
Of cases attributed to central etiologies the most commonly reported include ischemia or infarction (Charles et al. 1992; Horga Hernandez et al. 2006; Steiner et al. 1987; Stracciari et al. 1993) and multiple sclerosis (Deniz et al. 2012; Okuyucu et al. 2008).
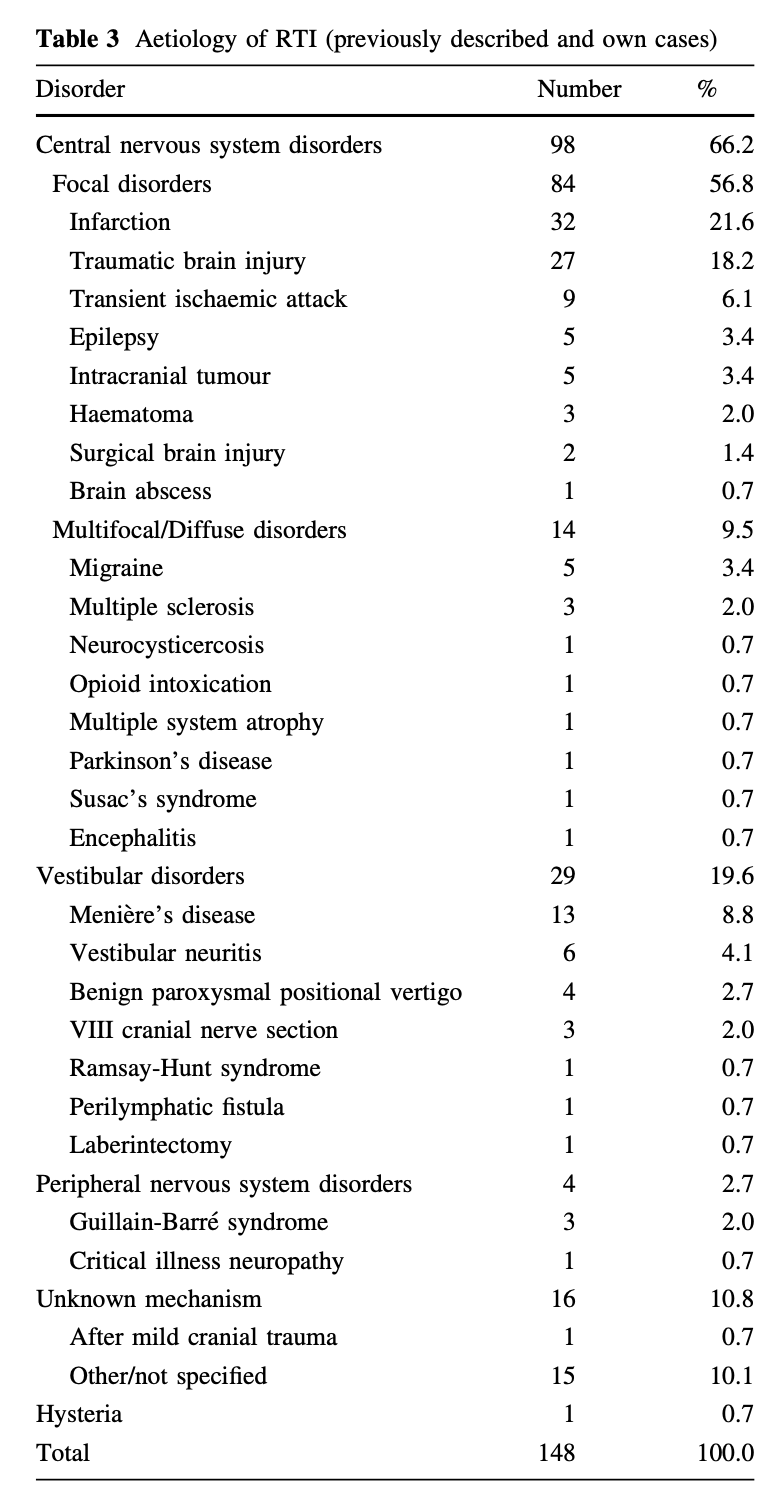
Sierra-Hidalgo and colleagues (Sierra-Hidalgo et al. 2012) studied 13 cases of their own patients with tilt illusions, as well as those from a review of the literature, amounting to a total of 135 cases. They provided the etiologies organized in the following Table.
Subclavian steal syndrome (SSS) has also been reported as a mechanism of illusions of inversion and tilt (Arntzen and Alstadhaug 2020).
In view of this differential diagnosis, a medically reasonable workup may include:
- Auditory testing, such as audiometry.
- Vestibular testing, such as cervical vestibular evoked myogenic potentials, ocular vestibular evoked myogenic potentials, video head impulse testing, videonystagmography and rotatory chair testing.
- MRI of the brain and internal auditory canals without and with contrast.
- If physical examination reveals a difference in blood pressure of ≥20 mm Hg between the arms, then consider checking Doppler ultrasound of the subclavian arteries to evaluate for subclavian steal syndrome.
Treatment and prognosis
Yip states that, “There is no current evidence that acute management has any beneficial effect on reducing RVM [reversal of vision metamorphopsia] episode duration” (Yap 2022).
There is no literature to support any specific intervention for prophylaxis against recurrent episodes. However:
- If otovestibular workup provides evidence of disease of the labyrinth or vestibular nerve (Akdal et al. 2017; Malis and Guyot 2003; Sierra-Hidalgo et al. 2012; Yap 2022), then it is logical to treat that underlying disease.
- Seizure appears to be a very rare cause of tilt illusions (Unal et al. 2006), but if there are grounds to suspect this (and if episodes are recurrent), then a trial of an anti-epileptic (or referral to an epileptologist) is reasonable.
- If workup provides no evidence of structural abnormalities (neurologic ischemia, demyelination, tumor, etc.) and an otovestibular workup provides no evidence of an otologic source, then (by exclusion) it is medically reasonable to entertain the possibility of migraine (Akdal et al. 2017; Lopez Dominguez et al. 2007; Sierra-Hidalgo et al. 2012; Yap 2022) and (if episodes are recurrent) consider a trial of migraine prophylaxis.
References
Akdal G, Toydemir HE, Tanriverdizade T, Halmagyi GM (2017) Room tilt illusion: a symptom of both peripheral and central vestibular disorders. Acta Neurol Belg 117: 363-365. doi: 10.1007/s13760-016-0628-z
Arntzen K, Alstadhaug KB (2020) Room tilt illusion and subclavian steal – a case report. BMC Neurol 20: 369. doi: 10.1186/s12883-020-01947-2
Bishopp T (1805) Case of Optical Illusion from Hysteria. Med Phys J 14: 117-118.
Charles N, Froment C, Rode G, Vighetto A, Turjman F, Trillet M, Aimard G (1992) Vertigo and upside down vision due to an infarct in the territory of the medial branch of the posterior inferior cerebellar artery caused by dissection of a vertebral artery. J Neurol Neurosurg Psychiatry 55: 188-9. doi: 10.1136/jnnp.55.3.188
Deniz O, Keklikoglu HD, Vural G, Temel S, Dilbaz FA (2012) Acute “upside-down” visual inversion in a patient with multiple sclerosis. Neurol Sci 33: 635-7. doi: 10.1007/s10072-011-0781-3
Graybiel A, Kellogg RS (1967) Inversion illusion in parabolic flight: its probable dependence on otolith function. Aerosp Med 38: 1099-103.
Horga Hernandez A, Pujadas F, Purroy F, Delgado P, Huertas R, Alvarez-Sabin J (2006) Upside down reversal of vision due to an isolated acute cerebellar ischemic infarction. J Neurol 253: 953-4. doi: 10.1007/s00415-006-0124-0
Kirsch V, Keeser D, Becker-Bense S, Karali T, Ertl-Wagner B, Brandt T, Dieterich M (2017) Vestibular and visual cortex activity during room tilt illusion. J Neurol 264: 70-73. doi: 10.1007/s00415-017-8457-4
Lopez Dominguez JM, Rojas-Marcos I, Sanz Fernandez G, Diaz Espejo C (2007) [Room tilt illusion: a rare symptom of migraine aura]. Neurologia 22: 58-60.
Malis DD, Guyot JP (2003) Room tilt illusion as a manifestation of peripheral vestibular disorders. Ann Otol Rhinol Laryngol 112: 600-5. doi: 10.1177/000348940311200705
Okuyucu EE, Okuyucu S, Karazincir S, Akoglu E, Duman T (2008) Acute ‘upside-down’ visual inversion due to multiple sclerosis. Mult Scler 14: 266-7. doi: 10.1177/1352458507082045
Pamir MN, Ozer AF, Siva A, Ozek MM, Kansu T (1990) “Upside down” reversal of vision after third ventriculostomy. J Clin Neuroophthalmol 10: 271-2.
River Y, Ben Hur T, Steiner I (1998) Reversal of vision metamorphopsia: clinical and anatomical characteristics. Arch Neurol 55: 1362-8. doi: 10.1001/archneur.55.10.1362
Roberts TD (1973) Inversion illusion in the so-called zero-gravity conditions of parabolic flight. Aerosp Med 44: 484-7.
Ropper AH (1983) Illusion of tilting of the visual environment. Report of five cases. J Clin Neuroophthalmol 3: 147-51.
Sierra-Hidalgo F, de Pablo-Fernandez E, Herrero-San Martin A, Correas-Callero E, Herreros-Rodriguez J, Romero-Munoz JP, Martin-Gil L (2012) Clinical and imaging features of the room tilt illusion. J Neurol 259: 2555-64. doi: 10.1007/s00415-012-6536-0
Solms M, Kaplan-Solms K, Saling M, Miller P (1988) Inverted vision after frontal lobe disease. Cortex 24: 499-509. doi: 10.1016/s0010-9452(88)80044-3
Steiner I, Shahin R, Melamed E (1987) Acute “upside down” reversal of vision in transient vertebrobasilar ischemia. Neurology 37: 1685-6. doi: 10.1212/wnl.37.10.1685-a
Stracciari A, Guarino M, Ciucci G, Pazzaglia P (1993) Acute upside down reversal of vision in vertebrobasilar ischaemia. J Neurol Neurosurg Psychiatry 56: 423. doi: 10.1136/jnnp.56.4.423
Tiliket C, Ventre-Dominey J, Vighetto A, Grochowicki M (1996) Room tilt illusion. A central otolith dysfunction. Arch Neurol 53: 1259-64. doi: 10.1001/archneur.1996.00550120071018
Unal A, Cila A, Saygi S (2006) Reversal of vision metamorphopsia: a manifestation of focal seizure due to cortical dysplasia. Epilepsy Behav 8: 308-11. doi: 10.1016/j.yebeh.2005.08.012
Yap JA (2022) Upside-down vision: a systematic review of the literature. BMJ Neurol Open 4: e000337. doi: 10.1136/bmjno-2022-000337
![]()