By Marcello Cherchi, MD PhD
For patients
The labyrinth (inner ear) has several “compartments” filled with fluids of different compositions and with different patterns of flow. There are connections between the labyrinth and the inside of the skull. A variety of conditions can change intracranial pressure (the pressure inside the skull), and those pressure changes can get transmitted to the labyrinth. Thus, intracranial pressure fluctuations can cause intra-labyrinthine pressure fluctuations, which in turn can cause temporary or permanent changes in hearing.
For clinicians
Overview
A common model (probably an oversimplification) of labyrinthine fluid dynamics is that the intracranial compartment communicates through the cochlear aqueduct to the perilymphatic space, and the endolymphatic space communicates via the endolymphatic duct to the endolymphatic sac. Changes in intracranial pressure can be transmitted to the labyrinth, and such changes (whether increase or decrease) appear to affect cochlear function adversely. The resulting cochlear dysfunction is probably a combination of mechanical disruption and alteration in chemical composition of the perilymphatic fluid and endolymphatic fluid.
When the cochlear dysfunction (manifesting as hearing loss) is the result of increased intracranial pressure (such as from hydrocephalus), normalization of intracranial pressure can bring about improvement in hearing.
When cochlear dysfunction (manifesting as hearing loss) is the result of decreased intracranial pressure (such as after a lumbar puncture, or over-shunting of normal pressure hydrocephalus), normalization of intracranial pressure can bring about improvement in hearing.
Hydraulics of the labyrinth
Outlining the “hydraulics” of the labyrinth can aid in understanding the mechanism by which intracranial pressure fluctuations may affect hearing.
The bony labyrinth is a convoluted cavity within the temporal bone that is filled with perilymphatic fluid. Within that perilymph-filled space is also located the membranous labyrinth, which is similarly shaped as the bony labyrinth (though slightly smaller), and the membranous labyrinth is in turn filled with endolymphatic fluid. These relationships are shown in the Figure below.
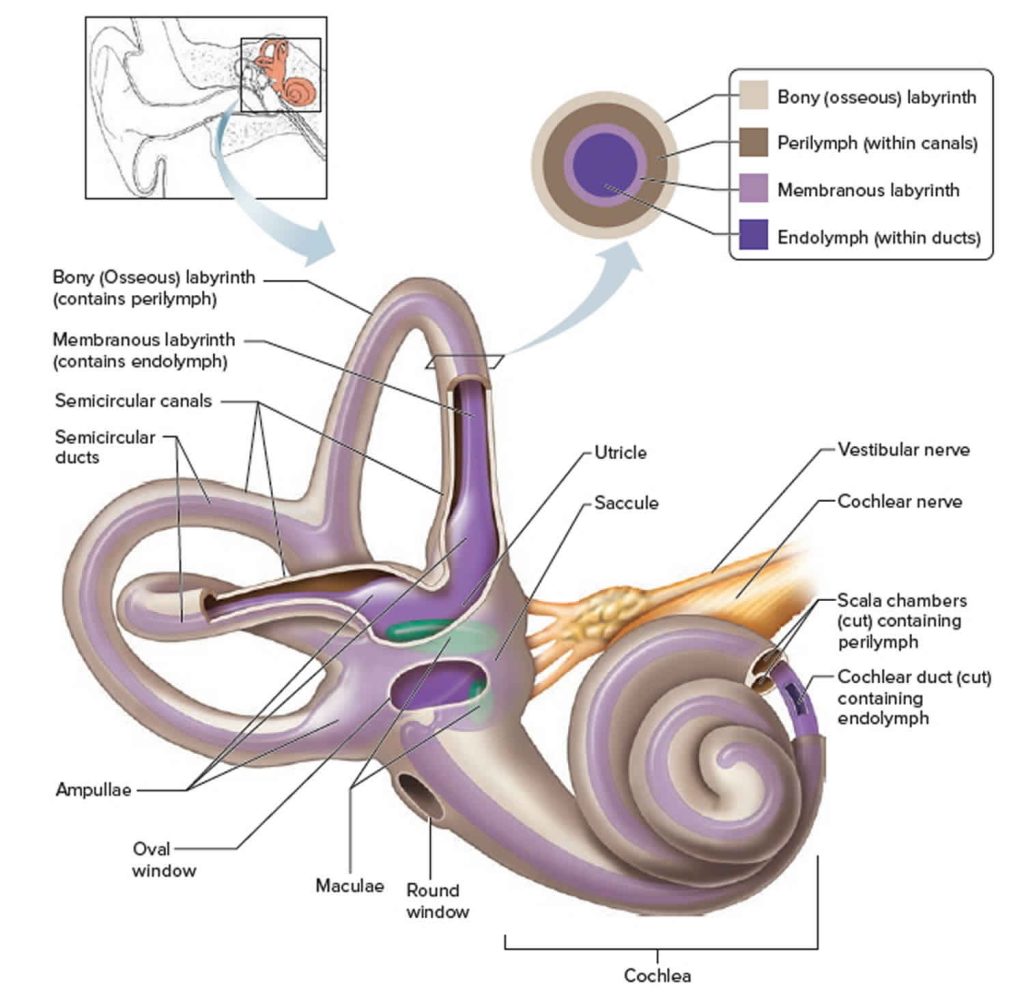
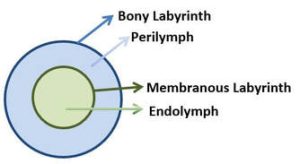
The Figure below is a schematic of the “containment relationships” between the bony labyrinth, perilymphatic fluid, membranous labyrinth and endolymphatic fluid.
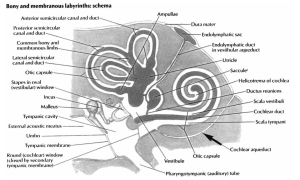
The perilymphatic fluid space communicates with the intracranial space via the cochlear aqueduct. The Figure below from Walsted (Walsted 2000), which gives credit to Frank Netter, shows the location of the cochlear aqueduct in the labyrinth.
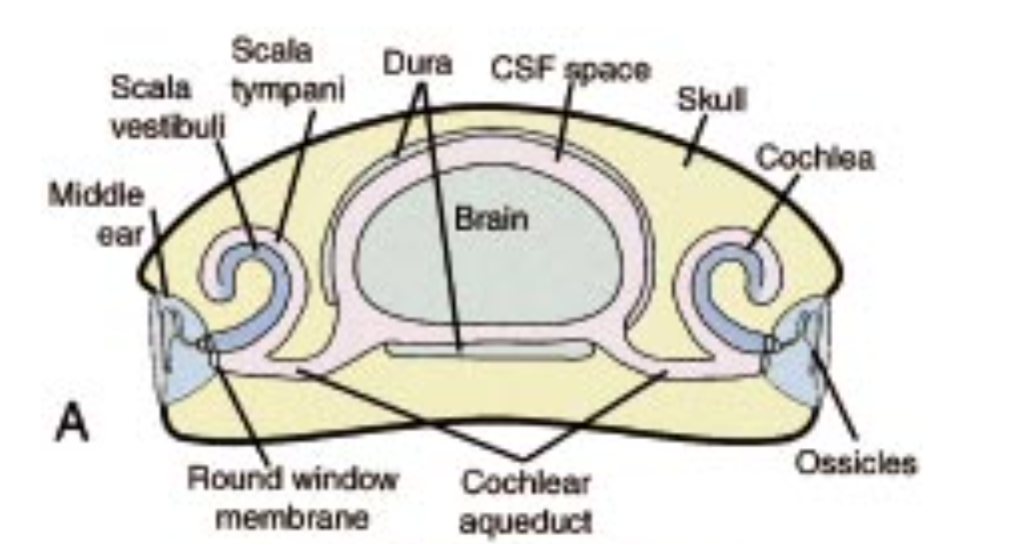
This relationship between the perilymph and the cerebrospinal fluid is schematically depicted in the Figure below.
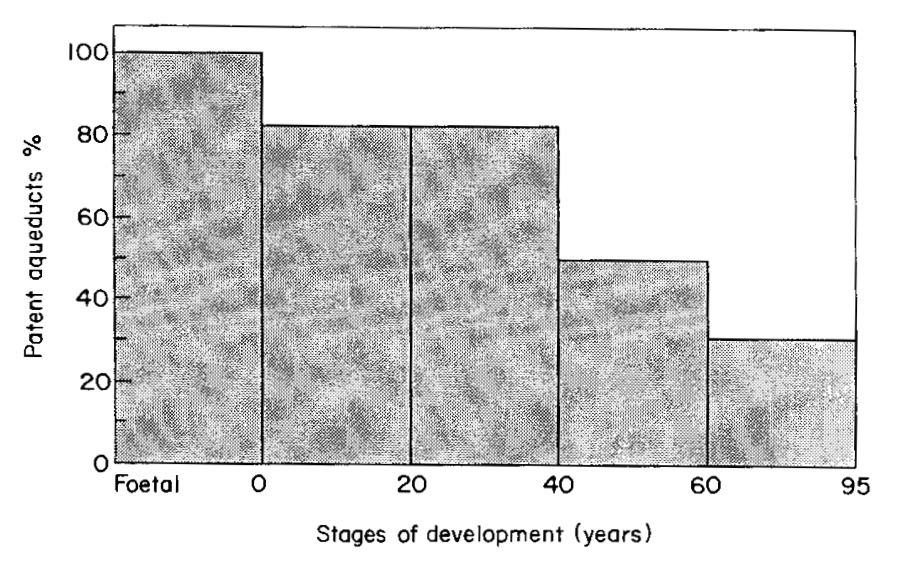
Although the cochlear aqueduct permits passage of fluid between the perilymphatic space and the intracranial space, a study of 250 human cadavers found that the patency of the cochlear aqueduct gradually decreases over the course of life (Włodyka 1978). The Figure below from Marchbanks and Reid (Marchbanks and Reid 1990) re‑depicts data originally from Wlodyka (Włodyka 1978).
The production and flow of perilymphatic fluid and endolymphatic fluid is complex (Sterkers, Ferrary et al. 1988). Perilymphatic fluid has a composition fairly similar to that of cerebrospinal fluid. Endolymphatic fluid has a very different ionic composition from that of perilymphatic fluid (Gagov, Chichova et al. 2018), yet there is some evidence that endolymph is derived from perilymph (Thalmann and Thalmann 1999).
Pressure fluctuations, intracranial and intra-labyrinthine
The relationships between endolymphatic fluid, perilymphatic fluid, and cerebrospinal fluid is inadequately understood. A commonly proposed model regarding, “perilymphatic and endolymphatic pressure balance is generally linked to the theory that the endolymphatic sac transmits cerebrospinal fluid (CSF) pressure changes to the endolymph to equalize CSF pressure changes transmitted to the perilymph via the cochlear aqueduct” (Carlborg and Farmer 1983). This model’s simplicity is appealing, but animal experiments suggest that the relationship is not so straightforward (Carlborg, Densert et al. 1982, Carlborg and Farmer 1983, Kishimoto, Nagahara et al. 1983, Marchbanks and Reid 1990, Carlborg, Konradsson et al. 1992).
Endolymph “is believed to be reabsorbed along the scala media by the stria vascularis, Reissner’s membrane, and the planum semilunatum, and at the saccus endolymphaticus which lies intracranially among the dural sheaths” (Barlas, Gokay et al. 1983).
It is thought that when intracranial pressure decreases, this results in perilymphatic fluid exiting the perilymphatic space and entering the intracranial compartment. This effectively permits the endolymphatic space to expand and “inflate” with more endolymphatic fluid, which results in “endolymphatic hydrops” (excessive endolymphatic fluid). This state of endolymphatic hydrops is similar to what occurs in Ménière’s disease, and is also associated with a similar pattern of hearing loss (predominantly low frequency sensorineural).
In contrast, when intracranial pressure increases, equilibration of that increased pressure will entail an increase in pressure in the perilymphatic space, a state of affairs sometimes referred to as perilymphatic hypertension (Paparella, Schachern et al. 1988, Miranda, Suzuki et al. 2006). Since the bony labyrinth is incompressible, perilymphatic hypertension will exert pressure on the membranous labyrinth, which may decrease the volume of endolymphatic fluid.
Both increased endolymphatic fluid (“endolymphatic hydrops”) and decreased endolymphatic fluid can have deleterious effects on cochlear function.
Increased intracranial pressure
Numerous case reports have documented hearing loss associated with increased intracranial pressure (Tandon, Sinha et al. 1973), and correction of intracranial pressure results in improvement (if not complete restoration) of hearing (Barlas, Gokay et al. 1983, Sammons, Jacobson et al. 2009, Dixon and Jones 2012, Jamshidi, Glidewell et al. 2017).
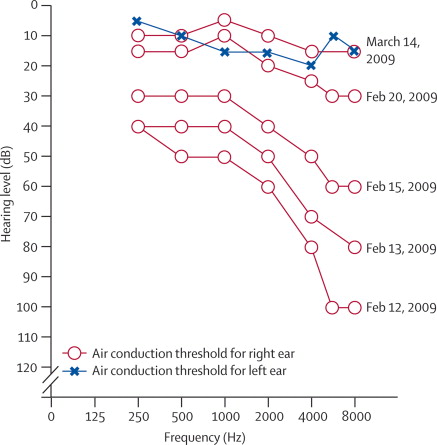
The Figure below, from Dixon and colleagues (Dixon and Jones 2012), clearly documents post-operative improvement (bottom panel) in pure tone hearing compared to pre-operative hearing (top panel) in a 14-year-old girl with hydrocephalus who underwent ventriculostomy without shunt placement.
Decreased intracranial pressure
Numerous case reports have documented that decreased intracranial pressure (such as following neurosurgical procedures in which cerebrospinal fluid is temporarily depleted) is also associated with hearing loss (Walsted, Salomon et al. 1991, Michel and Brusis 1992, Walsted, Nielsen et al. 1994, Hussain, Heard et al. 1996, Walsted 2000, Girardi, Cammisa et al. 2001, Spirakis and Hurley 2003, Pogodzinski, Shallop et al. 2008, Guillaume, Knight et al. 2012, Lim, Shim et al. 2014). Walsted (Walsted 2000) studied 126 patients who underwent “different neurosurgical procedures that involved puncture or incision of the dura,” and observed that, “The size of the [resulting] hearing loss, the number of affected patients, and the number of frequencies involved increased with increasing amount of CSF [cerebrospinal fluid] lost.” Walsted and colleagues (Walsted, Nielsen et al. 1994) also conducted a prospective study of 32 neurosurgical patients and found that the post-surgical hearing loss recovered in one week.
Note that this hearing loss can occur after shunt placement even in patients who (pre-surgically) had normal pressure hydrocephalus (van Veelen-Vincent, Delwel et al. 2001).
References
Barlas O, Gokay H, Turantan MI, Baserer N (1983) Adult aqueductal stenosis presenting with fluctuating hearing loss and vertigo. Report of two cases. J Neurosurg 59: 703-5. doi: 10.3171/jns.1983.59.4.0703
Carlborg B, Densert B, Densert O (1982) Functional patency of the cochlear aqueduct. Ann Otol Rhinol Laryngol 91: 209-15. doi: 10.1177/000348948209100219
Carlborg BI, Farmer JC, Jr. (1983) Transmission of cerebrospinal fluid pressure via the cochlear aqueduct and endolymphatic sac. Am J Otolaryngol 4: 273-82. doi: 10.1016/s0196-0709(83)80071-4
Carlborg BI, Konradsson KS, Carlborg AH, Farmer JC, Jr., Densert O (1992) Pressure transfer between the perilymph and the cerebrospinal fluid compartments in cats. Am J Otol 13: 41-8.
Dixon JF, Jones RO (2012) Hydrocephalus-associated hearing loss and resolution after ventriculostomy. Otolaryngol Head Neck Surg 146: 1037-9. doi: 10.1177/0194599811431234
Gagov H, Chichova M, Mladenov M (2018) Endolymph composition: paradigm or inevitability? Physiol Res 67: 175-179. doi: 10.33549/physiolres.933684
Girardi FP, Cammisa FP, Jr., Sangani PK, Parvataneni HK, Khan SN, Grewal H, Sandhu HS (2001) Sudden sensorineural hearing loss after spinal surgery under general anesthesia. J Spinal Disord 14: 180-3. doi: 10.1097/00002517-200104000-00014
Guillaume DJ, Knight K, Marquez C, Kraemer DF, Bardo DM, Neuwelt EA (2012) Cerebrospinal fluid shunting and hearing loss in patients treated for medulloblastoma. J Neurosurg Pediatr 9: 421-7. doi: 10.3171/2011.12.PEDS11357
Hussain SS, Heard CM, Bembridge JL (1996) Hearing loss following spinal anaesthesia with bupivacaine. Clin Otolaryngol Allied Sci 21: 449-54. doi: 10.1046/j.1365-2273.1996.00827.x
Jamshidi A, Glidewell C, Murnick J, Magge S, Reilly BK (2017) Resolution of bilateral sensorineural hearing loss following ventriculoperitoneal shunt and literature review. Int J Pediatr Otorhinolaryngol 100: 141-144. doi: 10.1016/j.ijporl.2017.06.034
Kishimoto S, Nagahara K, Fisch U, Dillier N (1983) Inner ear pressure measurements. Effects of obstruction of the cochlear aqueduct and endolymphatic duct on the perilymphatic pressure. Otolaryngol Clin North Am 16: 21-35.
Lim HW, Shim BS, Yang CJ, Kim JH, Cho YH, Cho YS, Kong DS, Koo JW, Han JH, Chung JW (2014) Hearing loss following ventriculoperitoneal shunt in communicating hydrocephalus patients: a pilot study. Laryngoscope 124: 1923-7. doi: 10.1002/lary.24553
Marchbanks RJ, Reid A (1990) Cochlear and cerebrospinal fluid pressure: their inter-relationship and control mechanisms. Br J Audiol 24: 179-87. doi: 10.3109/03005369009076554
Michel O, Brusis T (1992) Hearing loss as a sequel of lumbar puncture. Ann Otol Rhinol Laryngol 101: 390-4. doi: 10.1177/000348949210100503
Miranda JA, Suzuki FA, de Carvalho Borges MH (2006) Perilymphatic hyperension. Braz J Otorhinolaryngol 72: 430. doi: 10.1016/s1808-8694(15)30983-6
Paparella MM, Schachern PA, Goycoolea MV (1988) Perilymphatic hypertension. Otolaryngol Head Neck Surg 99: 408-13. doi: 10.1177/019459988809900410
Pogodzinski MS, Shallop JK, Sprung J, Weingarten TN, Wong GY, McDonald TJ (2008) Hearing loss and cerebrospinal fluid pressure: case report and review of the literature. Ear Nose Throat J 87: 144-7.
Sammons VJ, Jacobson E, Lawson J (2009) Resolution of hydrocephalus-associated sensorineural hearing loss after insertion of ventriculoperitoneal shunt. J Neurosurg Pediatr 4: 394-6. doi: 10.3171/2009.4.PEDS09103
Spirakis SE, Hurley RM (2003) Unilateral hearing loss in children with shunt-treated hydrocephalus. J Am Acad Audiol 14: 510-7. doi: 10.3766/jaaa.14.9.6
Sterkers O, Ferrary E, Amiel C (1988) Production of inner ear fluids. Physiol Rev 68: 1083-1128. doi: 10.1152/physrev.1988.68.4.1083
Tandon PN, Sinha A, Kacker SK, Saxena RK, Singh K (1973) Auditory function in raised intracranial pressure. J Neurol Sci 18: 455-67. doi: 10.1016/0022-510x(73)90139-1
Thalmann R, Thalmann I (1999) Source and role of endolymph macromolecules. Acta Otolaryngol 119: 293-6. doi: 10.1080/00016489950181260
van Veelen-Vincent ML, Delwel EJ, Teeuw R, Kurt E, de Jong DA, Brocaar MP, Pauw BK, Avezaat CJ, van Zanten BG (2001) Analysis of hearing loss after shunt placement in patients with normal-pressure hydrocephalus. J Neurosurg 95: 432-4. doi: 10.3171/jns.2001.95.3.0432
Walsted A (2000) Effects of cerebrospinal fluid loss on hearing. Acta Otolaryngol Suppl 543: 95-8. doi: 10.1080/000164800454099
Walsted A, Nielsen OA, Borum P (1994) Hearing loss after neurosurgery. The influence of low cerebrospinal fluid pressure. J Laryngol Otol 108: 637-41. doi: 10.1017/s0022215100127719
Walsted A, Salomon G, Thomsen J, Tos M (1991) Hearing decrease after loss of cerebrospinal fluid. A new hydrops model? Acta Otolaryngol 111: 468-76. doi: 10.3109/00016489109138371
Włodyka J (1978) Studies on cochlear aqueduct patency. Ann Otol Rhinol Laryngol 87: 22-8. doi: 10.1177/000348947808700105
![]()