By Marcello Cherchi, MD PhD
For patients
Sometimes when the inner ear is damaged, scar tissue develops within the inner ear, which sometimes turns into bone, which is called labyrinthine ossification. In these cases a patient loses hearing, and sometimes suffers from disequilibrium. If your doctor suspects labyrinthine ossification, they may check your hearing, and do a special CT or MRI of the inner ear.
For clinicians
Overview
In response to a variety of labyrinthine insults (infection, trauma, vascular problems, etc.), inflammatory responses may result in scar tissue which, in some cases, leads to abnormal bone formation within the labyrinth called labyrinthine ossification. This is a particularly feared complication of meningitis involving the labyrinth (Caye-Thomasen et al. 2012). This always manifests with sensorineural hearing loss, and less commonly with disequilibrium. The ossification is sometimes detectable by a combination of abnormalities on temporal bone CT and MRI of the internal auditory canals. There is no direct treatment because the end organ (labyrinth) is destroyed. Patients with labyrinthine ossification involving only one ear may benefit from a BiCROS hearing aid or bone-anchored hearing aid.
Introduction
The labyrinth can be damaged by a variety of processes, including infectious, inflammatory, traumatic, vascular, and abnormal bone metabolism (such as Paget’s disease) (Schwaber and Tarasidis 1990, Aralasmak, Dincer et al. 2009). The body’s attempt to heal from these insults often involves inflammatory responses, an unintended consequence of which can be fibrosis (Schwaber and Tarasidis 1990, Aralasmak, Dincer et al. 2009) — essentially the formation of scar tissue — and formation of new bone (Schwaber and Tarasidis 1990).
This can manifest in an abnormality variously referred to as labyrinthine ossification, labyrinthitis ossificans or sclerosis labyrinthitis (Swartz, Mandell et al. 1985, Schwaber and Tarasidis 1990, Aralasmak, Dincer et al. 2009). This is histopathologically characterized by the “formation of fibrous tissue and new bone within the labyrinthine space” (Schwaber and Tarasidis 1990) “as the final result of many inflammatory processes” (Swartz, Mandell et al. 1985) and fibrosis (Schwaber and Tarasidis 1990, Aralasmak, Dincer et al. 2009). Cases of labyrinthine ossification always involve hearing loss, and can also present with vestibular symptoms (Swartz, Mandell et al. 1985, Schwaber and Tarasidis 1990, Aralasmak, Dincer et al. 2009).
Testing: audiometry
The Figure below shows an audiogram from a patient with left-sided labyrinthine ossification following labyrinthine concussion without temporal bone fracture reported by Schwaber and Tarasidis (Schwaber and Tarasidis 1990).

Imaging
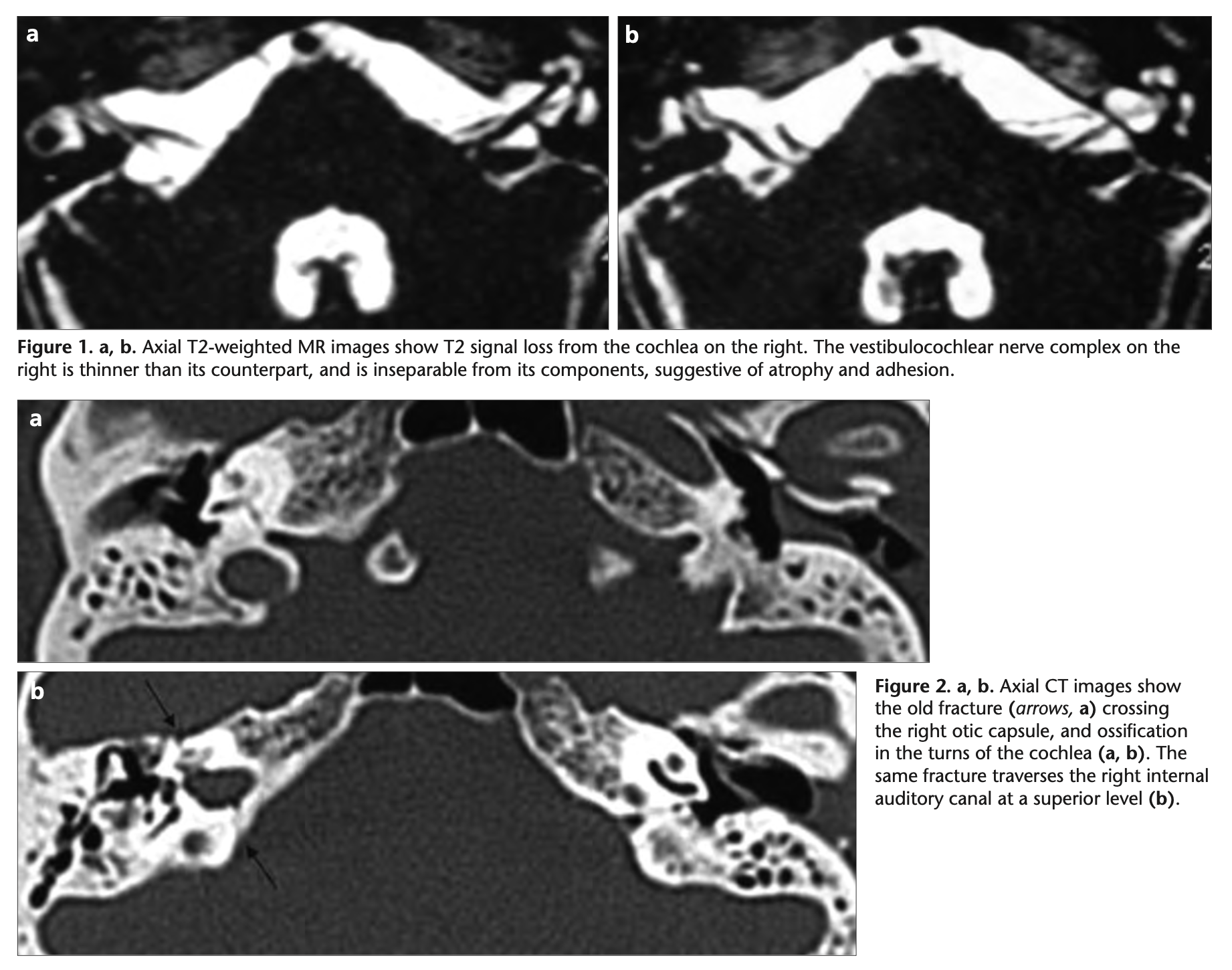
Labyrinthine ossification can be identified radiographically through a combination of findings on temporal bone CT (which can capture ossification of the bony labyrinth, and pneumolabyrinth) and MRI (which better images the membranous labyrinth and vestibulocochlear nerve) (Aralasmak, Dincer et al. 2009).
The Figure below, from Aralasmak and colleagues (Aralasmak, Dincer et al. 2009), shows an MRI of the internal auditory canals (upper two panels) and temporal bone CT (middle and lower panels) of a patient with labyrinthine ossification following a right-sided temporal bone fracture. The MRI images show signal loss of T2 signal in the right cochlea. The temporal bone CT images show ossification of the right cochlea and evidence of the original transverse temporal bone fracture.
Prognosis
The prognosis of labyrinthine ossification is poor because the end organ is destroyed.
Treatment
There is no known direct therapy for labyrinthine ossification. Since this disease process involves unilateral loss of auditory and vestibular function, patients may benefit from amplification strategies such as a BiCROS (bilateral contralateral routing of signals) hearing aid, or a BAHA (bone attached hearing aid), and from vestibular rehabilitation therapy aimed at unilateral vestibular loss.
References
Caye-Thomasen P, Dam MS, Omland SH, Mantoni M (2012) Cochlear ossification in patients with profound hearing loss following bacterial meningitis. Acta Otolaryngol 132: 720-5. doi: 10.3109/00016489.2012.656323
Schwaber MK, Tarasidis NG (1990) Labyrinthitis ossificans following post-traumatic hearing loss and vertigo: a case report with antemortem histopathology. Otolaryngol Head Neck Surg 102: 89-91. doi: 10.1177/019459989010200115
Swartz JD, Mandell DM, Faerber EN, Popky GL, Ardito JM, Steinberg SB, Rojer CL (1985) Labyrinthine ossification: etiologies and CT findings. Radiology 157: 395-8. doi: 10.1148/radiology.157.2.3931172
![]()