By Marcello Cherchi, MD PhD
For patients
The middle ear (the space immediately behind the eardrum) has two tiny muscles, called the stapedius and the tensor tympani, that normally tighten the eardrum in order to protect the ear from excessively loud sounds. However, if these muscles contract in an abnormal rhythmic pattern (“middle ear myoclonus”), the motion of the eardrum that they produce can be perceived as a sound (tinnitus). Usually this occurs spontaneously, and sometimes it can also cease spontaneously. The abnormal contraction of the eardrum can sometimes be observed by an examiner using a microscope or otoscope inserted in the ear canal, and it can sometimes be further characterized by a test (impedance tympanometry) that measures eardrum motion. Treatment includes watchful waiting, physical (zygomatic pressure), audiologic (masking), pharmacologic (a muscle relaxant such as orphenadrine), by injection (onabotulinum toxin) and surgical (sectioning the tendon of the muscle to the stapedius or the tensor tympani).
For clinicians
Overview
Middle ear myoclonus (MEM) consists of involuntary rhythmic contractions of the muscle to the stapedius and/or the tensor tympani muscle. Most cases are unilateral and episodic. Most cases are sporadic, though sometimes can occur in the context of another illness, such as multiple sclerosis, facial nerve paralysis or benign fasciculation syndrome. Binocular otomicroscopy or handheld otoscopy can sometimes reveal contraction of the tympanic membrane synchronous with the patient’s perception of tinnitus. Impedance tympanometry may be able to document the abnormal contraction of the tympanic membrane. Treatment includes watchful waiting, physical (zygomatic pressure), audiologic (masking), pharmacologic (such as orphenadrine), by injection (onabotulinum toxin) and surgical (tenotomy of the muscle to the stapedius or the tensor tympani).
Introduction
Middle ear myoclonus (MEM) encompasses the phenomena of tensor tympani myoclonus and stapedial myoclonus (Ellenstein, Yusuf et al. 2013).
The muscle attached to the stapes is innervated by a branch of the facial nerve. Contraction of the stapedius “pulls the stapes posteriorly with lateral displacement of the posterior tympanic membrane” (Bhimrao, Masterson et al. 2012). In its protective reflex function, “the stapedius contracts in response to intense low frequency acoustic stimuli” (Mukerji, Windsor et al. 2010).
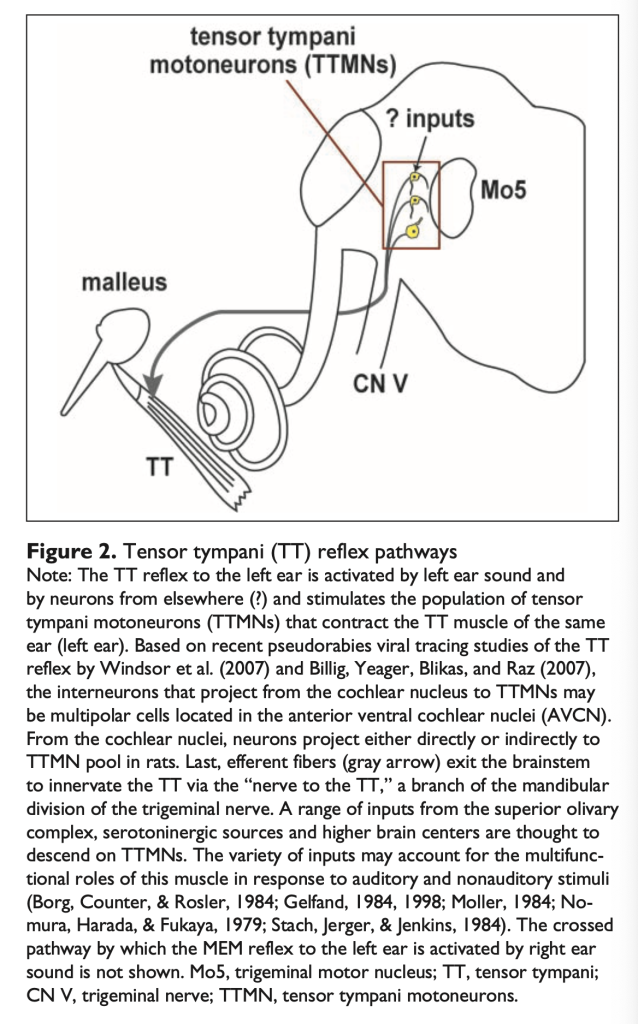
The tensor tympani muscle is innervated by the mandibular branch of the trigeminal nerve. When the tensor tympani contracts, it “pulls the malleus medially and anteriorly with inward movement of the tympanic membrane” (Bhimrao, Masterson et al. 2012). In its protective reflex function, “the tensor tympani is believed to contract in response to self-generated noise (chewing, swallowing) and non-auditory stimuli” (Mukerji, Windsor et al. 2010).
In normal circumstances these muscles mediate protective acoustic reflexes against loud sounds through “increase[d] the stapes-annular ligament impedance and decreased middle ear sound transmission” (Bhimrao, Masterson et al. 2012). But if the tensor tympani or stapedius pathologically contract in a rhythmic fashion due to myoclonus, then the ossicular chain will move (as if sounds were entering the ear from the external environment) and be perceived as sound.
Some authors include within this group the phenomena of “tubal myoclonus” and “peri-tubal myoclonus” (such as tensor veli palatini myoclonus). So-called “tubal myoclonus” (Virtanen 1983) actually refers to palatal tremor. In this condition the rhythmic raising and lowering of the soft palate intermittently occludes the pharyngeal orifice of the Eustachian tube, which the patient may perceive as a clicking sound, and can sometimes also be auscultated by the examiner. The tensor veli palatini muscle, innervated by the mandibular nerve branch of the trigeminal nerve, mediates some motion of the soft palate. In tensor veli palatini myoclonus (Ellenstein, Yusuf et al. 2013), unintended contraction of the tensor veli palatini may present with perception of a clicking sound, and this objective tinnitus can sometimes be auscultated by an examiner. In our view these variants are probably more informatively classified as a “palatal tremor” variant of oculopalatal tremor.
Clinical presentation
Tensor tympani myoclonus usually presents unilaterally, though rare cases of bilateral involvement have been reported (Cohen and Perez 2003). Patients afflicted with tensor tympani myoclonus often perceive a low- to middle-pitched tinnitus, and sometimes experience a “fluttering” sensation in the ear.
Stapedial myoclonus often presents as a “screeching” tinnitus, though in some cases (Brigo, Storti et al. 2013) a patient may describe it as low-pitched.
Bento and colleagues (Bento, Sanchez et al. 1998) presented an unusual case in which middle ear myoclonus caused continuous tinnitus. In this case the investigators simultaneously sectioned both the stapedius and the tensor tympani tendons, so the source of the tinnitus (one or both muscles) was unclear.
Most instances of tensor tympani myoclonus and stapedial myoclonus occur in isolation, but some cases appear in the context of some other illness. Zipfel and colleagues reported a case of bilateral tensor tympani and stapedial myoclonus occurring in the context of multiple sclerosis (Zipfel, Kaza et al. 2000). Watanabe and colleagues (Watanabe, Kumagami et al. 1974) reported a case of unilateral stapedial myoclonus occurring in the context of facial nerve paralysis. Brigo and colleagues (Brigo, Storti et al. 2013) reported a case of unilateral stapedial myoclonus presenting in the context of “benign fasciculation syndrome.” The tinnitus spontaneously resolved within 48 hours.
Demographics
The epidemiology of middle ear myoclonus has not been well described. A tinnitus prevalence study observed that tensor tympani myoclonus is more common in patients with hyperacusis (Westcott, Sanchez et al. 2013), which seems logical since the tensor tympani reflex serves a protective function against stimuli perceived to be excessively loud.
Pathophysiology
The neuroanatomical pathways mediating the stapedial reflex and tensor tympani reflex are depicted below in Figures from Mukerji and colleagues (Mukerji, Windsor et al. 2010)
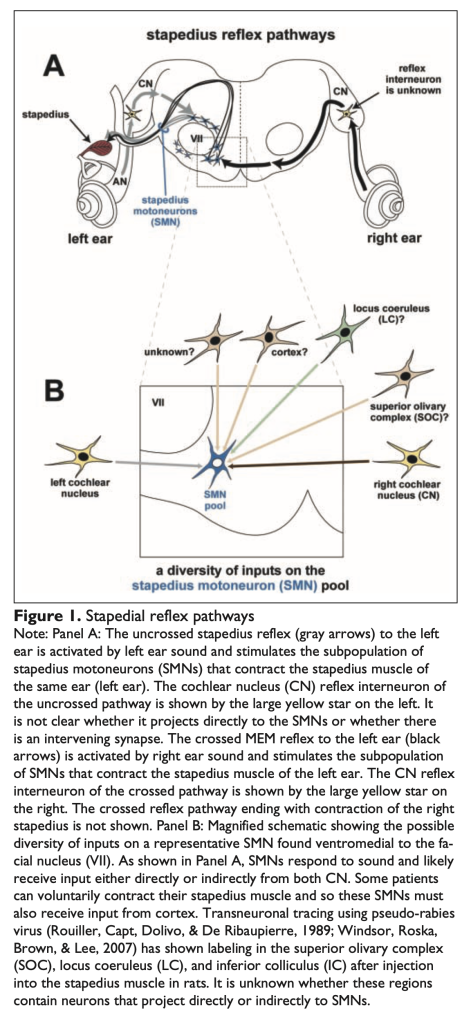
Although these neuroanatomical pathways are fairly well delineated, most instances of middle ear myoclonus do not have any clear precipitant, and the localization of the underlying lesion or dysfunction is unknown.
Physical examination
In some cases of tensor tympani myoclonus, binocular otomicroscopy or handheld otoscopy may show rhythmic movements of the tympanic membrane synchronous with the patient’s report of perceived sound (Cohen and Perez 2003, Abdul-Baqi 2004).
Testing
In some cases of tensor tympani myoclonus, impedance tympanometry may detect cyclical spikes in eardrum compliance (Abdul-Baqi 2004).
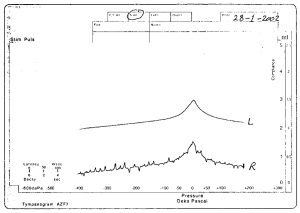
The Figure below compares tympanometry of the normal left ear, with tympanometry of the abnormal right ear (affected by middle ear myoclonus).
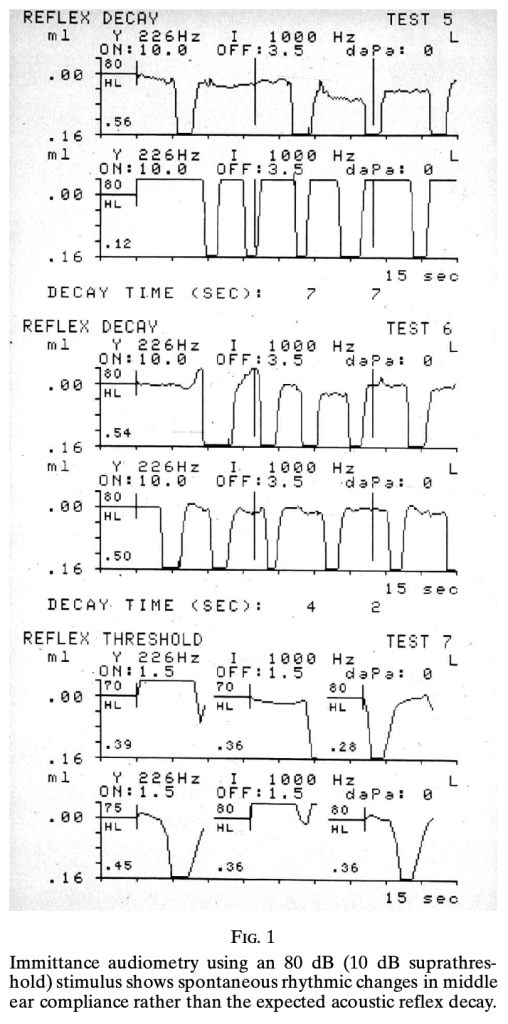
The Figure below shows impedance tympanometry of a patient with middle ear myoclonus (from Zipfel et al. 2000). In this case it was unclear whether the etiology was tensor tympani myoclonus or stapedial myoclonus.
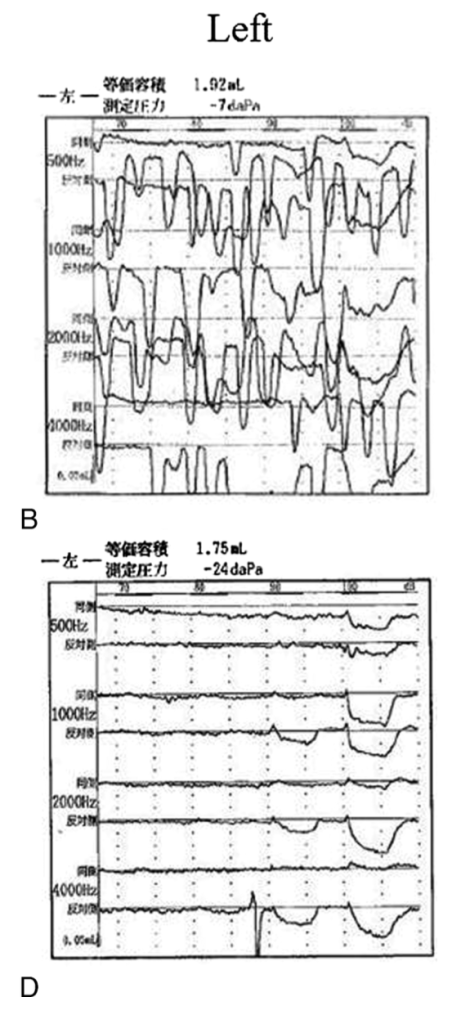
The Figure below displays impedance tympanometry from a patient with left-sided tensor tympani myoclonus pre-surgically (panel B) and post-surgically (panel D) (from Hidaka et al. 2013).
Treatment
There are no systematic treatment trials for middle ear myoclonus syndromes. Data are derived from case reports and case series.
Treatment, physical
Chan and Palaniappan (Chan and Palaniappan 2010) reported two cases of middle ear myoclonus that improved with “non-invasive, self-administered zygomatic pressure.”
Treatment, audiologic
Somewhat surprisingly, East and Hazell (East and Hazell 1987) report a case series of patients in whom the tinnitus from palatal myoclonus responded to wide band masking.
Treatment, pharmacologic
Since middle ear myoclonus syndromes are fundamentally myoclonic, some cases may respond to the use of muscle relaxants such as orphenadrine (Abdul-Baqi 2004).
Treatment, surgical
Stapedial myoclonus has been treated with injection of onabotulinum toxin (Liu, Fan et al. 2011).
Some cases of tensor tympani or stapedial myoclonus may be treated surgically, typically by resection (tenotomy) of the tendons of the tensor tympani muscle or the muscle to the stapedius (Badia, Parikh et al. 1994, Zipfel, Kaza et al. 2000). When it is known with confidence that the tinnitus is due to myoclonus of a specific muscle, it is desirable to apply this procedure only to that involved muscle while preserving the unaffected muscle (Cohen and Perez 2003, Hidaka, Honkura et al. 2013). While these procedures may cure the tinnitus, they also ablate the middle ear protective response that those intact muscles would mediate, leaving the patient more vulnerable to auditory trauma.
References
Abdul-Baqi KJ (2004) Objective high-frequency tinnitus of middle-ear myoclonus. J Laryngol Otol 118: 231-3. doi: 10.1258/002221504322928044
Badia L, Parikh A, Brookes GB (1994) Management of middle ear myoclonus. J Laryngol Otol 108: 380-2.
Bento RF, Sanchez TG, Miniti A, Tedesco-Marchesi AJ (1998) Continuous, high-frequency objective tinnitus caused by middle ear myoclonus. Ear Nose Throat J 77: 814-8.
Bhimrao SK, Masterson L, Baguley D (2012) Systematic review of management strategies for middle ear myoclonus. Otolaryngol Head Neck Surg 146: 698-706. doi: 10.1177/0194599811434504
Brigo F, Storti M, Lochner P, Nardone R (2013) Transitory stapedial myoclonus in a patient with benign fasciculation syndrome. J Laryngol Otol 127: 605-6. doi: 10.1017/S0022215113000297
Chan C, Palaniappan R (2010) Middle ear myoclonus: a new technique for suppression of spontaneous clicking tinnitus. Int Tinnitus J 16: 51-4.
Cohen D, Perez R (2003) Bilateral myoclonus of the tensor tympani: a case report. Otolaryngol Head Neck Surg 128: 441. doi: 10.1067/mhn.2003.6
East CA, Hazell JW (1987) The suppression of palatal (or intra-tympanic) myoclonus by tinnitus masking devices. A preliminary report. J Laryngol Otol 101: 1230-4.
Ellenstein A, Yusuf N, Hallett M (2013) Middle ear myoclonus: two informative cases and a systematic discussion of myogenic tinnitus. Tremor Other Hyperkinet Mov (N Y) 3. doi: 10.7916/D8RX9BS1
Hidaka H, Honkura Y, Ota J, Gorai S, Kawase T, Kobayashi T (2013) Middle ear myoclonus cured by selective tenotomy of the tensor tympani: strategies for targeted intervention for middle ear muscles. Otol Neurotol 34: 1552-8. doi: 10.1097/MAO.0000000000000126
Liu HB, Fan JP, Lin SZ, Zhao SW, Lin Z (2011) Botox transient treatment of tinnitus due to stapedius myoclonus: case report. Clin Neurol Neurosurg 113: 57-8. doi: 10.1016/j.clineuro.2010.07.022
Mukerji S, Windsor AM, Lee DJ (2010) Auditory brainstem circuits that mediate the middle ear muscle reflex. Trends Amplif 14: 170-91. doi: 10.1177/1084713810381771
Virtanen H (1983) Objective tubal tinnitus: a report of two cases. J Laryngol Otol 97: 857-62.
Watanabe I, Kumagami H, Tsuda Y (1974) Tinnitus due to abnormal contraction of stapedial muscle. An abnormal phenomenon in the course of facial nerve paralysis and its audiological significance. ORL J Otorhinolaryngol Relat Spec 36: 217-26. doi: 10.1159/000275177
Westcott M, Sanchez TG, Diges I, Saba C, Dineen R, McNeill C, Chiam A, O’Keefe M, Sharples T (2013) Tonic tensor tympani syndrome in tinnitus and hyperacusis patients: a multi-clinic prevalence study. Noise Health 15: 117-28. doi: 10.4103/1463-1741.110295
Zipfel TE, Kaza SR, Greene JS (2000) Middle-ear myoclonus. J Laryngol Otol 114: 207-9.
![]()