By Marcello Cherchi, MD PhD
For patients
The phrase “orthostatic hypertension” describes a person whose blood pressure increases too much when they go from a lying-down position to a standing up position. Sometimes your doctor might see this when just examining you, but in other cases you might need to have a test done called “tilt table testing.” The cause of orthostatic hypertension is not known, but most patients with this should talk with a cardiologist or kidney doctor.
For clinicians
Overview
Orthostatic hypertension is a condition in which going from a supine to a standing posture triggers an inappropriate rise in blood pressure. This can sometimes be detected by a bedside examination, but since the hypertensive response can also be delayed, tilt table testing is more sensitive. There is no universally accepted definition, but most clinicians use an increase of 20 mm Hg in systolic blood pressure as a criterion. Orthostatic hypertension can occur at any age; literature often describes it as having a greater prevalence in older age, and it has also been reported in association with renal disease, diabetes mellitus, and dysautonomia. The underlying mechanism of disease is not known, though proposed mechanisms include primary autonomic dysfunction and vascular causes. Orthostatic hypertension can manifest with lightheadedness upon standing, curiously resembling the “opposite” condition of orthostatic hypotension. Given the association of orthostatic hypertension with cardiovascular and renal disease, these patients should be referred to cardiology and/or nephrology.
Introduction
Orthostatic hypertension falls under the broader category of orthostatic intolerance, but has been less well studied than other orthostatic phenomena, such as orthostatic hypotension and postural orthostatic tachycardia.
Jordan and colleagues review a dozen definitions of orthostatic hypertension and observe that, “A uniform definition of orthostatic hypertension has never been established” (Jordan et al. 2020). Nevertheless, Jordan and colleagues proposed consensus statements defining orthostatic hypertension as an increase in systolic blood pressure ≥20 mm Hg when going from a supine to a standing position (Jordan et al. 2023a, b).
Epidemiology
Jordan and colleagues report that, “In studies defining orthostatic hypertension as a sustained increase in systolic blood pressure ≥20 mm Hg and/ or diastolic blood pressure ≥10 mmHg within 3 minutes of standing, the reported prevalence of orthostatic hypertension ranged between 5% and 30%” (Jordan et al. 2020).
Orthostatic hypertension can occur at any age, including in the pediatric population (Hu et al. 2020a; Hu et al. 2020b; Hu et al. 2020c; Zhang et al. 2014). Some investigators report a similar prevalence across the lifespan; for example, Wecht and colleagues (Wecht et al. 2016) studied 286 veterans and reported that the prevalence of orthostatic hypertension was similar in patients aged 20 – 30 years (17%) and patients over 70 years (19%). Other investigators reach different conclusions; for example, Jordan and colleagues report that, “The proportion of individuals with orthostatic hypertension increases with advancing age, greater body mass index, and chronic cardiovascular conditions such as essential hypertension” (Jordan et al. 2020).
Citing Yoshinari and colleagues (Yoshinari et al. 2001), Jordan and colleagues comment that, “Patients with diabetes mellitus showed a 5-fold higher orthostatic hypertension prevalence compared with a nondiabetic population” (Jordan et al. 2020).
Pathophysiological mechanism of disease
Many diseases have been reported in association with orthostatic hypertension. Renal diseases are probably the most common, but other associated conditions include dysautonomia, diabetes mellitus and older age.
- Citing McCann and colleagues (McCann and Romansky 1940), Jordan and colleagues comment that, “The term orthostatic hypertension, which is an increase in blood pressure with standing, began to appear in the medical literature as early as in the 1940 and 1950s, typically in relation to kidney diseases” (Jordan et al. 2020).
- Chronic kidney disease appears to be a risk factor for orthostatic hypertension. Ghazi and colleagues (Ghazi et al. 2024) reported that out of 1386 adult patients with chronic kidney disease, 153 (11.0%) were found to have orthostatic hypertension. Rouabhi and colleagues (Rouabhi et al. 2021) reported that out of 3873 patients with chronic kidney disease, 81 (2.1%) were found to have orthostatic hypertension.
- Orthostatic hypertension has been “observed in association with a variety of other clinical conditions, including essential hypertension, dysautonomias, and type 2 diabetes mellitus” (Fessel and Robertson 2006).
- “Conditions associated with higher activity of the sympathetic nervous system and/or baroreflex dysregulation, such as diabetes, essential hypertension, and aging have been found to be often associated with [orthostatic hypertension]” (Palatini 2023).
Such associations are suggestive, but they do not prove causality.
Given the rapidity of the hypertensive response, most investigators speculate that such response is mediated by the autonomic nervous system:
- “Dysfunction of the autonomous nervous system is considered to be the primary pathophysiological disturbance” (Magkas et al. 2019)
- “The underlying pathophysiology is thought to involve activation of the sympathetic nervous system” (Fessel and Robertson 2006).
- “Sympathetic overactivation” (Hu et al. 2020c)
- “Most conditions associated with orthostatic hypertension are associated with altered cardiovascular adrenergic control mechanisms” (Jordan et al. 2020).
Even if these speculations are correct, they leave open the question of whether orthostatic hypertension is a primary autonomic disorder, or whether such autonomic dysfunction is secondary to some other process.
The significantly greater prevalence of orthostatic hypertension in diabetics (Yoshinari et al. 2001) suggests (though does not prove) an autonomic neuropathy.
Another category of proposed mechanisms relates orthostatic hypertension to vascularly-based phenomena.
- Reports of renal arterial abnormalities suggest that circulatory disturbances (essentially, inadequate renal perfusion) inappropriately trigger an autonomic response. For example, Tsukamoto and colleagues (Tsukamoto et al. 1988) reported a case in which they concluded that orthostatic hypertension in their patient was due to renal artery stenosis and nephroptosis (defined as a “condition in which the kidney descends more than two vertebral bodies (or >5 cm) during a position change from supine to upright” (Murari et al. 2012)).
- Streeten and colleagues (Streeten et al. 1985) suggest that orthostatic hypertension, “involves excessive orthostatic blood pooling, which results in decreased venous return, decreased cardiac output, increased sympathetic stimulation (presumably through low-pressure cardiopulmonary receptors), and excessive arteriolar, but not venular, constriction.”
These explanations have their merits, but most investigators reach conclusions such as:
- “The actual etiology is poorly understood” and therefore “in need of further investigation” (Fessel and Robertson 2006) and “deserves more attention” (Jordan et al. 2020).
- “The pathogenetic mechanisms leading to [orthostatic hypertension] are still controversial and may vary with age” (Palatini 2023).
Clinical presentation
Curiously, the presentation of orthostatic hypertension can closely resemble orthostatic hypotension, even though these appear to be diametrically opposed blood pressure phenomena. Specifically, patients with orthostatic hypertension may complain of lightheadedness upon standing.
Physical examination
As mentioned earlier, various definitions of orthostatic hypertension have been proposed (Jordan et al. 2020). Practically, most clinicians use the consensus statement proposed by Jordan and colleagues, defining orthostatic hypertension as an increase in systolic blood pressure ≥20 mm Hg when going from a supine to a standing position (Jordan et al. 2023a, b).
Somewhat similarly to orthostatic hypotension, orthostatic hypertension can be variably present, and may depend in part on the time of day during which it is measured (Ghazi et al. 2024). Given its intermittent nature, if a practitioner does not find orthostatic hypertension on physical examination, yet has a high index of suspicion for it, it is medically reasonable to re-examine the patient subsequently, or refer them for tilt table testing (on the possibility that there is delayed orthostatic hypertension).
Testing
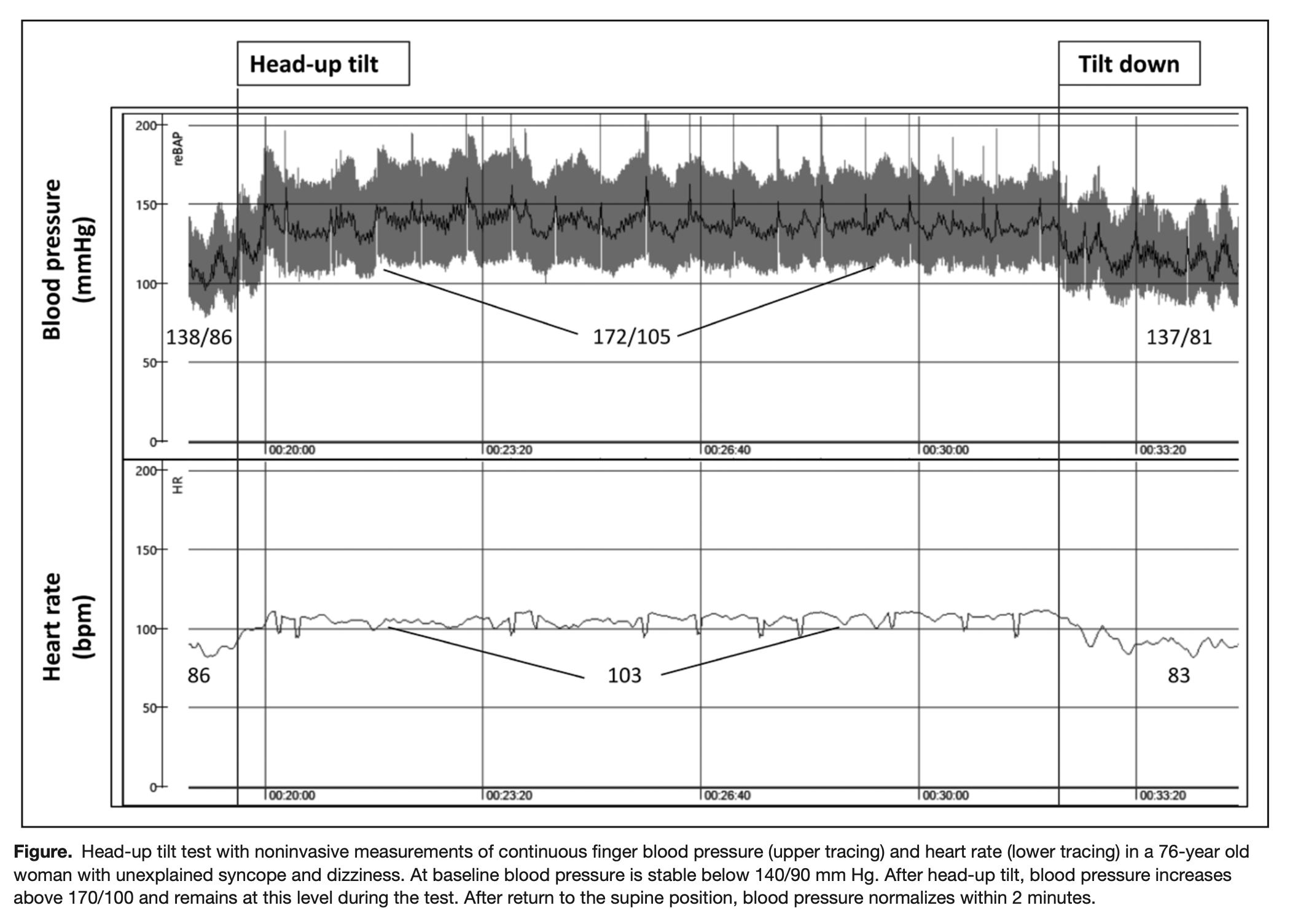
Although orthostatic hypertension can often be detected on a bedside examination, tilt table testing is the modality of choice for securing the diagnosis (Lee and Kim 2016; Petersen et al. 2021), in part because the manifestation of hypertension can occur at any point after the head upright tilt (Petersen et al. 2021), including after some delay.
The Figure below, from Jordan and colleagues (Yoshinari et al. 2001), shows results from a tilt table test in a 76-year-old woman with orthostatic hypertension.
Differential diagnosis
The main differential diagnosis of orthostatic hypertension includes other disorders in which disequilibrium is triggered upon assuming an upright posture, such as orthostatic hypotension, or (less commonly) benign paroxysmal positional vertigo.
Treatment
Given the proposed mechanisms of disease, and given the other medical conditions in whose context orthostatic hypertension occurs, it is sensible for these patients to be referred to a cardiologist and/or nephrologist.
References
Fessel J, Robertson D (2006) Orthostatic hypertension: when pressor reflexes overcompensate. Nat Clin Pract Nephrol 2: 424-31. doi: 10.1038/ncpneph0228
Ghazi L, Cohen JB, Townsend RR, Drawz PE, Rahman M, Pradhan N, Cohen DL, Weir MR, Rincon-Choles H, Juraschek SP (2024) Orthostatic hypotension, orthostatic hypertension, and ambulatory blood pressure in patients with chronic kidney disease in CRIC. J Hypertens 42: 329-336. doi: 10.1097/hjh.0000000000003604
Hu Y, He B, Han Z, Wang Y, Tao C, Wang Y, Jin H, Du J (2020a) Risk Factors for Orthostatic Hypertension in Children. J Pediatr 227: 212-217.e1. doi: 10.1016/j.jpeds.2020.07.030
Hu Y, Jin H, Du J (2020b) Orthostatic Hypertension in Children: An Update. Front Pediatr 8: 425. doi: 10.3389/fped.2020.00425
Hu Y, Wang Y, He B, Wang Y, Han Z, Tao C, Li H, Jiang Y, Tang C, Du J (2020c) Sympathetic Overactivation From Supine to Upright Is Associated With Orthostatic Hypertension in Children and Adolescents. Front Pediatr 8: 54. doi: 10.3389/fped.2020.00054
Jordan J, Biaggioni I, Kotsis V, Nilsson P, Grassi G, Fedorowski A, Kario K (2023a) Consensus statement on the definition of orthostatic hypertension endorsed by the American Autonomic Society and the Japanese Society of Hypertension. Clin Auton Res 33: 69-73. doi: 10.1007/s10286-022-00897-8
Jordan J, Biaggioni I, Kotsis V, Nilsson P, Grassi G, Fedorowski A, Kario K (2023b) Consensus statement on the definition of orthostatic hypertension endorsed by the American Autonomic Society and the Japanese Society of Hypertension. Hypertens Res 46: 291-294. doi: 10.1038/s41440-022-01074-0
Jordan J, Ricci F, Hoffmann F, Hamrefors V, Fedorowski A (2020) Orthostatic Hypertension: Critical Appraisal of an Overlooked Condition. Hypertension 75: 1151-1158. doi: 10.1161/hypertensionaha.120.14340
Lee H, Kim HA (2016) Orthostatic hypertension: An underestimated cause of orthostatic intolerance. Clin Neurophysiol 127: 2102-7. doi: 10.1016/j.clinph.2015.12.017
Magkas N, Tsioufis C, Thomopoulos C, Dilaveris P, Georgiopoulos G, Doumas M, Papadopoulos D, Tousoulis D (2019) Orthostatic hypertension: From pathophysiology to clinical applications and therapeutic considerations. J Clin Hypertens (Greenwich) 21: 426-433. doi: 10.1111/jch.13491
McCann WS, Romansky MJ (1940) Orthostatic hypertension: the effect of nephroptosis on the renal blood flow. Journal of the American Medical Association 115: 573-578. doi: 10.1001/jama.1940.02810340001001
Murari SB, Gadepalli T, Rao VP, Ram R (2012) Renal scintigraphy in diagnosis and management of nephroptosis. Indian J Nucl Med 27: 52-4. doi: 10.4103/0972-3919.108874
Palatini P (2023) Orthostatic Hypertension: A Newcomer Among the Hypertension Phenotypes. Hypertension 80: 1993-2002. doi: 10.1161/hypertensionaha.123.21537
Petersen Á, Salas-Herrera C, Lerma C, Brown-Escobar C, Kostin A, Sierra-Beltrán M, González-Hermosillo JA (2021) Transient Orthostatic Hypertension During Head-Up Tilt Test in Young Adults: A Phenotype of Blood Pressure Variability. J Clin Neurophysiol 38: 242-249. doi: 10.1097/wnp.0000000000000685
Rouabhi M, Durieux J, Al-Kindi S, Cohen JB, Townsend RR, Rahman M (2021) Orthostatic Hypertension and Hypotension and Outcomes in CKD: The CRIC (Chronic Renal Insufficiency Cohort) Study. Kidney Med 3: 206-215.e1. doi: 10.1016/j.xkme.2020.10.012
Streeten DH, Auchincloss JH, Jr., Anderson GH, Jr., Richardson RL, Thomas FD, Miller JW (1985) Orthostatic hypertension. Pathogenetic studies. Hypertension 7: 196-203. doi: 10.1161/01.hyp.7.2.196
Tsukamoto Y, Komuro Y, Akutsu F, Fujii K, Marumo F, Kusano S, Kikawada R (1988) Orthostatic hypertension due to coexistence of renal fibromuscular dysplasia and nephroptosis. Jpn Circ J 52: 1408-14. doi: 10.1253/jcj.52.1408
Wecht JM, Weir JP, Martinez S, Eraifej M, Bauman WA (2016) Orthostatic hypotension and orthostatic hypertension in American veterans. Clin Auton Res 26: 49-58. doi: 10.1007/s10286-015-0328-4
Yoshinari M, Wakisaka M, Nakamura U, Yoshioka M, Uchizono Y, Iwase M (2001) Orthostatic hypertension in patients with type 2 diabetes. Diabetes Care 24: 1783-6. doi: 10.2337/diacare.24.10.1783
Zhang Q, Li J, Xie Y, Zhao J, Du J (2014) Orthostatic hypertension in children and adolescents with postural tachycardia syndrome. J Trop Pediatr 60: 461-6. doi: 10.1093/tropej/fmu055
![]()