By Marcello Cherchi, MD PhD
For patients
“Orthostatic intolerance” refers to symptoms such as dizziness and lightheadedness that tend to occur when a patient is upright (sitting or standing) rather than in a lying down position. These symptoms occur due to overly robust fluctuations in blood pressure and cardiac pulse rate.
“Orthostatic” means “pertaining to standing up.” “Hypotension” means “low blood pressure.” The phrase “orthostatic hypotension” refers to an excessive drop in blood pressure when a person assumes an upright posture (sitting or standing). Overly robust drops in blood pressure can cause people to become lightheaded when they stand up, or even to faint. There is no universal consensus on the criteria for diagnosis, but commonly used figures include a drop of systolic blood pressure (the “top number”) by more than 20 mm Hg, or a drop of diastolic blood pressure (the “bottom number”) by more than 10 mm Hg within 3 minutes of standing ([No authors] 1996, [No authors] 1996, [No authors] 1996, Kaufmann 1996). Orthostatic hypotension in itself is not a disease, but may be a manifestation of a variety of underlying medical conditions.
A related condition is postural orthostatic tachycardia syndrome (sometimes abbreviated “POTS”), which is an excessive increase in heart rate (“tachycardia”) when a person assumes an upright (sitting or standing) posture. Overly robust increases in heart rate when a person assumes an upright posture can cause dizziness. There is no universal consensus on the criteria for diagnosis, but a commonly used figure is an increase in heart rate of more than 30 beats per minute (McGee, Abernethy et al. 1999). Orthostatic tachycardia in itself is not a disease, but can reflect underlying medical conditions.
Part of the underlying mechanism of orthostatic hypotension and postural orthostatic tachycardia is that when you stand up, gravity pulls blood into the legs. This “pooling” of blood in the legs means that less blood is available in the thorax to be pumped upward and perfuse the brain adequately. A healthy person’s body quickly senses that this “pooling” is occurring, and invokes strategies for preventing it, including a modest increase in heart rate, an increase in the amount of blood that the heart ejects each time it pumps (the “stroke volume”), and constriction of peripheral blood vessels. If the body is diseased and either does not sense that blood is pooling in the legs, or does not invoke compensatory strategies, then the brain does not receive the blood it needs, and a person may feel lightheaded or may actually faint.
Although there are several ways of approaching these problems, it is generally preferable to start with methods that do not involve adding medications (Freeman 2003). Not all methods are applicable in all cases. Below are discussed some of the methods with which we usually start.
Below we discuss a range of non-pharmacologic strategies. We are aware that not every patient is able to (or wants to) use every single strategy, so we present about a dozen of them so that you can start with those that appear most practical or feasible to you. The more strategies you use, and the longer you use them, the more likely you will be to bring this problem under control. You can monitor your progress by purchasing a home blood pressure cuff. Check your blood pressure and pulse (while in a lying down position) after you have been lying flat for 3 minutes, then stand up and recheck your blood pressure (while in a standing position). Be sure to check your blood pressure and pulse at approximately the same time every day.
⬜ Review your medications with your other doctors to see whether any of the medications may be contributing to this problem. If it is possible to eliminate, reduce, or substitute any of those medications, do so. Certainly, medications intended to lower blood pressure can worsen this problem. However, many other medications have the unintended effect of lowering blood pressure. Do not simply stop medications without first consulting the physicians who originally prescribed them.
⬜ Increase the amount of fluid you drink. Overall this has been shown to be the most effective strategy for patients (Newton and Frith 2018). There are no exact criteria on how much of an increase is appropriate. We usually recommend that patients try to drink at least twice as much fluid as usual. Some fluids “don’t count” towards this goal. For instance, caffeine, alcohol, and very sugary drinks actually have mild diuretic actions, so after a few hours the net effect of such beverages is that you will have less fluid in your body than you did before drinking them. It is preferable, when possible, to drink water, or water containing electrolytes (such as Gatorade or Pedialyte). PLEASE NOTE that the strategy of increasing fluid intake may not be appropriate in all patients — for instance, patients with kidney failure may be advised by their doctor not to increase fluid intake.
⬜ Increase the amount of salt in your diet. Eating salt helps your body to maintain more effectively whatever water you drink. Usually we recommend that patients simply use the salt shaker a little more than usual. PLEASE NOTE that some patients should not increase their dietary salt — for instance, many patients with cardiac disease are specifically instructed to reduce salt in their diet.
⬜ Wear Jobst stockings. Jobst stockings are basically tights. By squeezing the legs and lower body, they reduce the amount of blood that pools there. Ideally the stockings should come up to the waist, because this prevents pooling of blood not only in the legs but also in the pelvic venous plexus. Stockings that only come up to the knee or to the hip are less effective. Jobst stockings can be obtained in medical supply stores. They do not require a prescription. There are different degrees of “tightness.” Choose a grade that you can tolerate. If the stockings are too loose, then they will not be effective.
⬜ Wear an abdominal binder. An abdominal binder is like a girdle. By modestly compressing the abdomen, it promotes the return of blood from the abdominal venous plexus up into the thorax, and can benefit patients with orthostatic hypotension (Smit, Wieling et al. 2004, Figueroa, Singer et al. 2015). Abdominal binders are available at medical supply stores. They come in different sizes and degrees of tightness, and do not require a prescription.
⬜ Adjust your bed so that the head is higher than the pelvis, and the pelvis is higher than the feet. This is called the “reverse Trendelenburg position.” This strategy keeps a little bit of blood pooled in the legs at night and thereby keeps the blood pressure maintaining system (called the renin-angiotensin-aldosterone axis) slightly activated, so that when you get up in the morning, you will be less likely to suffer a large drop in blood pressure. PLEASE NOTE that it is NOT ADEQUATE simply to sleep with a few extra pillows beneath the head. Rather, THE WHOLE BED MUST BE INCLINED. Usually this is most easily accomplished by putting 1 or 2 bricks beneath each post at the head of the bed. The reverse Trendelenburg position is shows below. The angle (35˚) in the figure below is exaggerated for purposes of illustration. In your case, an angle of 15˚ to 20˚ is adequate.
|
Reverse Trendelenburg position. From http://www.eschmann.co.uk/operatingtheatre/operatingtables/powered/t20as/procedures.html. |

⬜ Avoid eating large meals. When you eat a large meal, your body purposefully shunts up to 20% of the blood to the gastrointestinal tract to aid in digestion (Victor and Ropper 2001). This means that less blood is available for other tasks, such as circulating to the brain. When feasible, it is preferable to eat a greater number of small meals rather than a smaller number of large meals. This does not mean that you need to reduce the total amount of food per day that you eat; rather, it means that you should distribute your food intake more evenly throughout the day. In other words, it is better to “graze” rather than “feast.”
⬜ Avoid hot environments. When you feel warm, or when you perspire, your body purposefully shunts blood to circulate just beneath the skin in an attempt to dissipate heat. This means that less blood is available for other tasks, such as circulating to the brain. When possible, avoid hot environments.
⬜ Avoid straining at stool. The act of straining is called the Valsalva maneuver. It is part of many other tasks, such as lifting heavy objects. The Valsalva maneuver actually induces a decrease in blood pressure both during the maneuver itself, and after “releasing” from the straining (Looga 2005). If constipation is causing you to strain frequently at stool, try to alleviate the constipation with increased hydration, increased dietary fiber, prunes, or laxatives.
⬜ Get up gradually in the morning. Most people have already learned to do this instinctively. When you wake up, first sit at the side of the bed for a few minutes before actually standing up to walk.
⬜ Orthostatic training. This consists of several relatively simple exercises that can be taught to you by a physical therapist familiar with the problem of orthostatic hypotension.
The main exercise is simple and can be done at home. It consists simply of standing up against a wall for 30 minutes. Initially patients may find they are unable to maintain this posture for a full 30 minutes, but over time they increase their tolerance and usually are able to achieve this target. One study of an orthostatic training program followed 24 patients who actually experienced syncope (fainting) due to their orthostatic hypotension (Abe, Kondo et al. 2002). The intention was for patients to stand against a wall without moving for 30 minutes twice per day. However, most patients only ended up doing the exercise once per day. Nevertheless, after 5 to 18 months, 22 patients (92%) no longer suffered syncope. Most other studies have found similar results (Ector, Reybrouck et al. 1998, Reybrouck, Heidbuchel et al. 2000, Abe, Kohshi et al. 2003, Abe, Sumiyoshi et al. 2003, Kinay, Yazici et al. 2004, Reybrouck and Ector 2006). However, a minority of studies found no significant difference between those patients who performed the exercises and those who did not (Foglia-Manzillo, Giada et al. 2004, On, Park et al. 2007, Duygu, Zoghi et al. 2008).
For patients who have failed other therapies, we usually recommend trying orthostatic training since there is no significant medical risk. The more frequently you perform the exercises, and the greater the length of time (i.e., preferably months rather than simply weeks), the more likely it is that you will benefit from them.
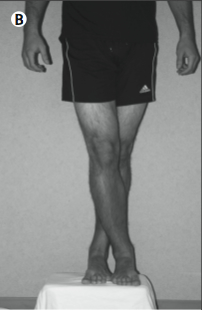
Even when the above-mentioned exercise is helpful, some patients may still experience occasional lightheadedness when upright. If a patient has this sensation and fears that she might faint, then there are several “counter-maneuvers” that reduce its likelihood. The maneuvers include toe raising, leg crossing, thigh contraction, and bending at the waist, all of which reduce venous capacity and increase total peripheral resistance (Low and Singer 2008). Illustrations of these maneuvers are given below.
|
|
|
|
|
|
|
|
Toe raise |
Leg cross |
Forward lean |
Step up |
Genuflection |
Squat |





References
[No authors] (1996a) Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. J Neurol Sci 144: 218-9.
[No authors] (1996b) Consensus statement on the definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. The Consensus Committee of the American Autonomic Society and the American Academy of Neurology. Neurology 46: 1470.
[No authors] (1996c) The definition of orthostatic hypotension, pure autonomic failure, and multiple system atrophy. J Auton Nerv Syst 58: 123-4.
Abe H, Kohshi K, Nakashima Y (2003) Effects of orthostatic self-training on head-up tilt testing and autonomic balance in patients with neurocardiogenic syncope. J Cardiovasc Pharmacol 41 Suppl 1: S73-6.
Abe H, Kondo S, Kohshi K, Nakashima Y (2002) Usefulness of orthostatic self-training for the prevention of neurocardiogenic syncope. Pacing Clin Electrophysiol 25: 1454-8.
Abe H, Sumiyoshi M, Kohshi K, Nakashima Y (2003) Effects of orthostatic self-training on head-up tilt testing for the prevention of tilt-induced neurocardiogenic syncope: comparison of pharmacological therapy. Clin Exp Hypertens 25: 191-8.
Duygu H, Zoghi M, Turk U, Akyuz S, Ozerkan F, Akilli A, Erturk U, Onder R, Akin M (2008) The role of tilt training in preventing recurrent syncope in patients with vasovagal syncope: a prospective and randomized study. Pacing Clin Electrophysiol 31: 592-6. doi: 10.1111/j.1540-8159.2008.01046.x
Ector H, Reybrouck T, Heidbuchel H, Gewillig M, Van de Werf F (1998) Tilt training: a new treatment for recurrent neurocardiogenic syncope and severe orthostatic intolerance. Pacing Clin Electrophysiol 21: 193-6.
Figueroa JJ, Singer W, Sandroni P, Sletten DM, Gehrking TL, Gehrking JA, Low P, Basford JR (2015) Effects of patient-controlled abdominal compression on standing systolic blood pressure in adults with orthostatic hypotension. Arch Phys Med Rehabil 96: 505-10. doi: 10.1016/j.apmr.2014.10.012
Foglia-Manzillo G, Giada F, Gaggioli G, Bartoletti A, Lolli G, Dinelli M, Del Rosso A, Santarone M, Raviele A, Brignole M (2004) Efficacy of tilt training in the treatment of neurally mediated syncope. A randomized study. Europace 6: 199-204. doi: 10.1016/j.eupc.2004.01.002
Freeman R (2003) Treatment of orthostatic hypotension. Semin Neurol 23: 435-42. doi: 10.1055/s-2004-817727
Kaufmann H (1996) Consensus statement on the definition of orthostatic hypotension, pure autonomic failure and multiple system atrophy. Clin Auton Res 6: 125-6.
Kinay O, Yazici M, Nazli C, Acar G, Gedikli O, Altinbas A, Kahraman H, Dogan A, Ozaydin M, Tuzun N, Ergene O (2004) Tilt training for recurrent neurocardiogenic syncope: effectiveness, patient compliance, and scheduling the frequency of training sessions. Jpn Heart J 45: 833-43. doi: JST.JSTAGE/jhj/45.833 [pii]
Looga R (2005) The Valsalva manoeuvre–cardiovascular effects and performance technique: a critical review. Respir Physiol Neurobiol 147: 39-49.
Low PA, Singer W (2008) Management of neurogenic orthostatic hypotension: an update. Lancet Neurol 7: 451-8. doi: S1474-4422(08)70088-7
McGee S, Abernethy WB, 3rd, Simel DL (1999) The rational clinical examination. Is this patient hypovolemic? JAMA 281: 1022-9. doi: jrc80003 [pii]
Newton JL, Frith J (2018) The efficacy of nonpharmacologic intervention for orthostatic hypotension associated with aging. Neurology 91: e652-e656. doi: 10.1212/WNL.0000000000005994
On YK, Park J, Huh J, Kim JS (2007) Is home orthostatic self-training effective in preventing neurally mediated syncope? Pacing Clin Electrophysiol 30: 638-43. doi: 10.1111/j.1540-8159.2007.00725.x
Reybrouck T, Ector H (2006) Tilt training: a new challenge in the treatment of neurally mediated syncope. Acta Cardiol 61: 183-9.
Reybrouck T, Heidbuchel H, Van de Werf F, Ector H (2000) Tilt training: a treatment for malignant and recurrent neurocardiogenic syncope. Pacing Clin Electrophysiol 23: 493-8.
Smit AA, Wieling W, Fujimura J, Denq JC, Opfer-Gehrking TL, Akarriou M, Karemaker JM, Low PA (2004) Use of lower abdominal compression to combat orthostatic hypotension in patients with autonomic dysfunction. Clin Auton Res 14: 167-75. doi: 10.1007/s10286-004-0187-x
Victor M, Ropper AH (2001) Adams and Victor’s Principles of Neurology, 7 edn. McGraw-Hill, New York
![]()