By Marcello Cherchi, MD PhD
For patients
Discomfort or pain in the ear can arise from diseases of the ear itself. However, diseases “outside” of the ear can also cause symptoms perceived in the ear; the medical term for this is that the ear symptoms are “referred” from a problem in a different anatomical location.
A different example of referred pain with which many people are familiar is the condition called sciatica, in which lumbosacral nerve roots are impinged on (“pinched”) in the lower back, yet most of the pain is perceived in the leg (which those nerve roots innervate).
Since ear pain can arise from a number of different sources (ear, skull, jaw, teeth, neck), the treatment may differ depending on the source.
For clinicians
Overview
Ear pain and discomfort usually result from disease of the ear itself, for which there is a broad differential diagnosis. However, aural symptoms can also be referred from other anatomical locations, with the most common sources being dental, temporomandibular and cervical. Migraine can also cause aural symptoms. Practically, cases of otalgia are generally referred to an otolaryngologist specializing in otology. If there is evidence of (or clinical suspicion for) dental disease, then a dental evaluation is also reasonable.
Discussion
Hwa and Brant (Hwa and Brant 2021) offer the following differential diagnosis of otalgia:
Congenital
-
- Branchial cleft cyst
- Sebaceous cyst
- Epidermoid cyst
Infectious
-
- Perichondritis
- Cellulitis
- Acute otitis externa
- Herpes zoster oticus
- Malignant otitis externa
- Acute otitis media—complicated or uncomplicated
- Otomastoiditis/petrous apicitis
- Suppurative labyrinthitis
Traumatic
-
- Auricular trauma/hematoma
- External auditory canal laceration
- Tympanic membrane perforation (blast or puncture)
- Ear foreign body
Autoimmune/Inflammatory
-
- Relapsing polychondritis
- Granulomatosis with polyangiitis (GPA)
- Sarcoidosis
Neurologic
-
- Trigeminal neuralgia
- Glossopharyngeal neuralgia
- Vagal neuralgia
- Migraine
Neoplastic
-
- Cutaneous malignancy
- Nasopharyngeal carcinoma
- Squamous cell carcinoma of the head and neck
Other
-
- Chondrodermatitis nodularis helicis
- TMJ arthralgia/arthritis
- Dental pathology
- Eagle syndrome
The majority of cases of otalgia are attributable to primary otologic problems. However, a significant minority of cases of otalgia are referred otalgia. The work by Taziki and Behnampour (Taziki and Behnampour 2012) reported that of 770 patients with otalgia, 94 patients (12.2%) had referred otalgia. Of the patients with referred otalgia, the pain was referred from dental problems (62.8%), pharyngitis (24.5%), temporomandibular joint dysfunction (8.8%), sinusitis (2.1%), Bell’s palsy (1.1%) and pharyngeal abscess (1.1%).
The multiple somatosensory innervations of the ear (Charlett and Coatesworth 2007, Taziki and Behnampour 2012) comprises the mechanism underlying the variety of sources of referred otalgia. This complexity is reflected by the anatomy depicted in the figures below.
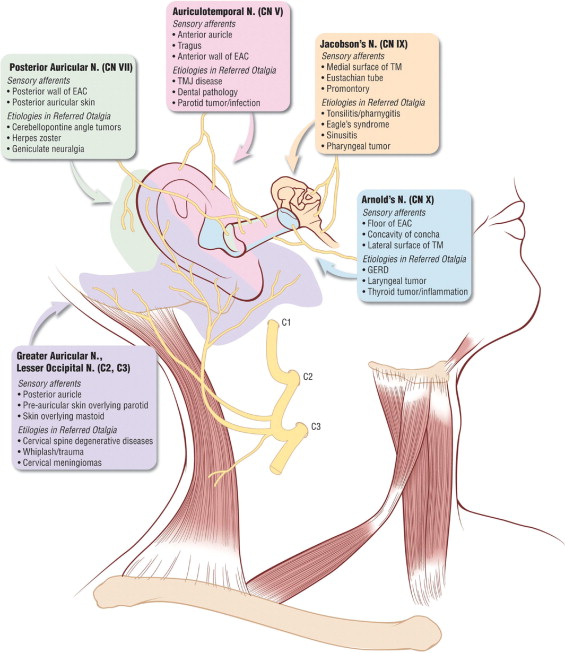 |
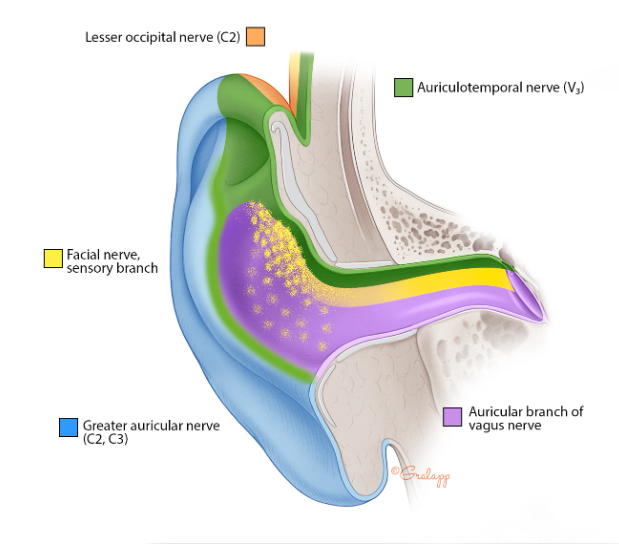
Based on the distributions of sensory innervations depicted in these diagrams, one might suspect that simply identifying the painful area on the ear should enable anatomical localization of the source of otalgia.
However, despite what is shown in the figures above, there is actually considerable variation between individuals in the ear’s somatosensory innervation (Shah and Blevins 2003).
The table below summarizes the anatomy, innervation, and sources of referred pain (Charlett and Coatesworth 2007, Jaber, Leonetti et al. 2008), with pathologies drawn from the statistics of a case series of 123 patients (Charlett and Coatesworth 2007).
|
Part of ear innervated |
Nerve |
Frequency in case series (Charlett and Coatesworth 2007) |
Organs from which referred pain may arise |
Pathologies to consider (with percentage frequency in case series (Charlett and Coatesworth 2007)) |
|
• Tragus • Anterior auricle • Anterior wall of external canal • Anterior portion of the lateral tympanic membrane |
Auriculotemporal nerve (branch of the mandibular division of CN V) and meningeal nerve (branch of the maxillary division of CN V) |
46% |
Temporomandibular joint Dentition Face Mastoid Anterior two-thirds of tongue |
• Temporomandibular joint disease (28%) • Dental disease (9%) • Trigeminal neuralgia (3%) • Mandibular osteomyelitis/tumor (3%) • Parotid infection or tumor (3%) |
|
• Posterior wall of external auditory canal • Posterior lateral surface of tympanic membrane • Posterior skin of auricle |
Posterior auricular nerve (part of tympanic plexus, chorda tympani branch, and an unnamed branch of CN VII) |
2% |
• Vestibular schwannoma (2%) • Herpes zoster affecting facial nerve (1%) |
|
|
• Middle ear • Upper Eustachian tube • Medial surface of tympanic membrane |
Jacobson’s nerve and part of tympanic plexus (CN IX) |
7% |
Nasal cavity Nasopharynx Paranasal sinuses Palatine tonsils Tonsillar fossa Soft palate Oropharynx Posterior one-third of tongue Infratemporal fossa |
• Sinusitis (3%) • Tonsillitis/pharyngitis (2%) • Pharyngeal tumor (1%) • Glossopharyngeal neuroma (1%) A separate case series (n=615) found that 3% of patients with a primary complaint of otalgia had a malignant tumor in the infratemporal fossa (Leonetti, Li et al. 1998). |
|
• Inferior and posterior aspects of the external auditory canal • Concavity of concha • Lateral surface of tympanic membrane |
Inferior branch of Arnold’s nerve (auricular branch of CN X) |
3% |
Thyroid Infratemporal fossa Hypopharynx Larynx Trachea Esophagus Lung Abdominal viscera |
The following can irritate the superior division of the laryngeal nerve (a branch of CN X) and be referred to the ear: • Gastroesophageal (laryngeal/pharyngeal) reflux (2%) • Cricopharyngeal spasm (1%) • Vagal stimulator (1%) Others: • Thyroiditis • Thyroid tumor • Laryngeal carcinoma |
|
• Posterior auricle • Skin overlying the mastoid bone and parotid gland |
Greater auricular nerve (C2 and C3) and lesser occipital nerve (C3) roots of the cervical plexus |
42% |
Cervical spine |
Cervical spine degenerative disease (37%), including: • Osteoarthritis • Cervical facette disease • Spondylosis • Disc herniation • Spinal stenosis Other: • Whiplash (2%) • Cervical meningioma • Arnold-Chiari type I (1%) • Vascular (1%) • Fibromyalgia (1%) • Cervical nerve root cysts (1%) |
According to these data, most referred ear pain arises in cervical spine disease (Jaber, Leonetti et al. 2008), followed closely by temporomandibular joint dysfunction (Hernandez-Nuno de la Rosa, Keith et al. 2022). Bruxism, even in the absence of temporomandibular joint dysfunction, can also provoke otalgia (Kim 2016).
Migraine is not localizing in the anatomical sense, but is well known to manifest with otalgia (Teixido, Seymour et al. 2011, Sussman, Zimmerman et al. 2022) or aural fullness (Moshtaghi, Ghavami et al. 2018, Risbud, Muhonen et al. 2021, Celebisoy, Kisabay Ak et al. 2022, Danno, Wolf et al. 2022, Karsan, Nagaraj et al. 2022, Shi, Wang et al. 2022, Tiwari, Maurya et al. 2022).
Practically, cases of otalgia are generally referred to an otolaryngologist specializing in otology. If there is evidence of (or clinical suspicion for) dental disease, then a dental evaluation is also reasonable.
References
Celebisoy N, Kisabay Ak A, Ozdemir HN, Gokcay F, Durmaz GS, Karti DT, Toydemir HE, Yayla V, Colpak Isikay AI, Erkent I, Ozcelik P, Akdal G, Atac C, Bicakci S, Goksu EO, Uyaroglu FG (2022) Vestibular migraine, demographic and clinical features of 415 patients: A multicenter study. Clin Neurol Neurosurg 215: 107201. doi: 10.1016/j.clineuro.2022.107201
Charlett SD, Coatesworth AP (2007) Referred otalgia: a structured approach to diagnosis and treatment. Int J Clin Pract 61: 1015-21. doi: 10.1111/j.1742-1241.2006.00932.x
Danno D, Wolf J, Ishizaki K, Kikui S, Hirata K, Takeshima T (2022) Cranial autonomic symptoms in migraine are related to central sensitization: a prospective study of 164 migraine patients at a tertiary headache center. BMC Neurol 22: 89. doi: 10.1186/s12883-022-02610-8
Hernandez-Nuno de la Rosa MF, Keith DA, Siegel NS, Moreno-Hay I (2022) Is there an association between otologic symptoms and temporomandibular disorders?: An evidence-based review. J Am Dent Assoc 153: 1096-1103. doi: 10.1016/j.adaj.2021.07.029
Hwa TP, Brant JA (2021) Evaluation and Management of Otalgia. Med Clin North Am 105: 813-826. doi: 10.1016/j.mcna.2021.05.004
Jaber JJ, Leonetti JP, Lawrason AE, Feustel PJ (2008) Cervical spine causes for referred otalgia. Otolaryngol Head Neck Surg 138: 479-85. doi: 10.1016/j.otohns.2007.12.043
Jackler RK (2019) Ear surgery illustrated : a comprehensive atlas of otologic microsurgical techniques. Thieme, New York
Janis JE, Rohrich RJ, Gutowski KA (2005) Otoplasty. Plast Reconstr Surg 115: 60e-72e. doi: 10.1097/01.prs.0000156218.93855.c9
Karsan N, Nagaraj K, Goadsby PJ (2022) Cranial autonomic symptoms: prevalence, phenotype and laterality in migraine and two potentially new symptoms. J Headache Pain 23: 18. doi: 10.1186/s10194-022-01389-w
Kim SH (2016) A Case of Bruxism-Induced Otalgia. J Audiol Otol 20: 123-6. doi: 10.7874/jao.2016.20.2.123
Leonetti JP, Li J, Smith PG (1998) Otalgia. An isolated symptom of malignant infratemporal tumors. Am J Otol 19: 496-8.
Moshtaghi O, Ghavami Y, Mahboubi H, Sahyouni R, Haidar Y, Ziai K, Lin HW, Djalilian HR (2018) Migraine-Related Aural Fullness: A Potential Clinical Entity. Otolaryngol Head Neck Surg 158: 100-102. doi: 10.1177/0194599817739255
Risbud A, Muhonen EG, Tsutsumi K, Martin EC, Abouzari M, Djalilian HR (2021) Migraine Features in Patients With Isolated Aural Fullness and Proposal for a New Diagnosis. Otol Neurotol. doi: 10.1097/MAO.0000000000003324
Shah RK, Blevins NH (2003) Otalgia. Otolaryngol Clin North Am 36: 1137-51. doi: 10.1016/s0030-6665(03)00120-8
Shi S, Wang D, Ren T, Wang W (2022) Auditory Manifestations of Vestibular Migraine. Front Neurol 13: 944001. doi: 10.3389/fneur.2022.944001
Sussman S, Zimmerman Z, Chishom T, Reid L, Seyyedi M (2022) Migraine-Associated Otalgia: An Underappreciated Entity. J Audiol Otol 26: 90-96. doi: 10.7874/jao.2021.00465
Taziki MH, Behnampour N (2012) A study of the etiology of referred otalgia. Iran J Otorhinolaryngol 24: 171-6.
Teixido M, Seymour P, Kung B, Lazar S, Sabra O (2011) Otalgia associated with migraine. Otol Neurotol 32: 322-5. doi: 10.1097/MAO.0b013e318200a0c4
Tiwari A, Maurya PK, Qavi A, Kulshreshtha D, Thacker AK, Singh AK (2022) Cranial Autonomic Symptoms in Migraine: An Observational Study. Ann Indian Acad Neurol 25: 654-659. doi: 10.4103/aian.aian_948_21
![]()