By Marcello Cherchi, MD PhD
For patients
When syphilis affects inner ear function (hearing and balance) it is sometimes referred to as otosyphilis. Symptoms of otosyphilis may include hearing loss, tinnitus and disequilibrium. These symptoms can be caused by other diseases (besides syphilis), so your doctor may check several tests of hearing and balance, and may consider checking imaging of the brain (such as a head CT or brain MRI). Treatment of otosyphilis is the same as treatment for syphilis in general, and involves antibiotics (which are usually prescribed by an internist or infectious disease specialist). If the hearing and balance symptoms do not improve with antibiotics, then patients often consider consultation with an audiologist (for the hearing symptoms) and vestibular physical therapist (for the disequilibrium).
For clinicians
Overview
Otosyphilis refers to otovestibular involvement of infection by Treponema pallidum. The incidence of syphilis began to increase during the AIDS epidemic. The proportion of patients with syphilis that go on to develop otosyphilis is unknown. Otosyphilis can manifest at any stage of syphilitic infection. The audiovestibular symptoms (hearing loss, tinnitus, disequilibrium) may be the initial manifestations of the disease. When characterized by audiometry, the hearing loss in otosyphilis is usually (though not always) sensorineural, and can be unilateral, bilateral (symmetrical or asymmetrical) and affect any frequencies; in short, any pattern is possible. Some patients may also have abnormal brainstem auditory evoked responses. Few studies of vestibular testing in otosyphilis patients are available. Imaging may show cranial osteolytic lesions involving the labyrinth (on temporal bone CT), and soft tissue damage or space-occupying intracranial gummas (on brain MRI). The audiovestibular manifestations of otosyphilis may resemble autoimmune inner ear disease or Ménière’s disease. Separately from otosyphilis, neurosyphilis can cause tabes dorsalis (degeneration of the posterior columns of the spinal cord with impairment of vibration and proprioception) associated with sensory ataxia and thus disequilibrium. Treatment of otosyphilis is the same as treatment for syphilis in general. In some patients hearing loss improves, though this improvement may be transient. Vestibular symptoms sometimes respond to treatment. For patients in whom the audiologic and/or vestibular symptoms do not respond to treatment for syphilis, referral to audiology and vestibular physical therapy is medically reasonable.
Introduction
Treponema pallidum is the spirochetal pathogen responsible for syphilis. Syphilis can affect many organ systems, and thus have a variety of manifestations. When syphilis involves the audiovestibular system it is sometimes called “otosyphilis.”
Epidemiology
Syphilis was previously somewhat uncommon in the United States, but its incidence began to increase during the AIDS pandemic in 1980s. Ramchandani and colleagues (Yimtae et al. 2007), citing data from the Centers for Disease Control, state that the rate of early syphilis infection in the united states increased 71% from 2014 – 2018. Increases of this magnitude have led to descriptions of it as a resurgence (Papalini et al. 2017; Theeuwen et al. 2019).
It is not known what percentage of syphilis patients go on to develop otosyphilis. Dombrowski and colleagues (Dombrowski et al. 2015) analyzed a case series of 573 patients with “early or unknown duration syphilis” and found that 22 (3.9%) of patients reported hearing loss, and 15 (2.7%) reported tinnitus.
Otosyphilis can occur at any stage of syphilis infection, but its symptoms are more likely to develop in early stages — meaning primary syphilis, secondary syphilis, and early latent syphilis (Jones-Vanderleest 2022). The otologic (Jones-Vanderleest 2022) and vestibular (Hungerbuhler and Regli 1978) symptoms may be the initial manifestations of the disease.
Pathophysiological mechanism of disease
In syphilis cellular damage occurs both as a result of the pathogen (Treponema pallidum) itself, as well as a series of immunological responses (Carlson et al. 2011) and inflammation.
Clinical presentation
Otosyphilis can present with any combination of hearing loss, tinnitus or disequilibrium, and these may be the initial manifestations of the disease (Hungerbuhler and Regli 1978; Jones-Vanderleest 2022). The Table below, from Yimtae and colleagues (Yimtae et al. 2007), reports the prevalence of these symptoms in a case series of 85 patients.
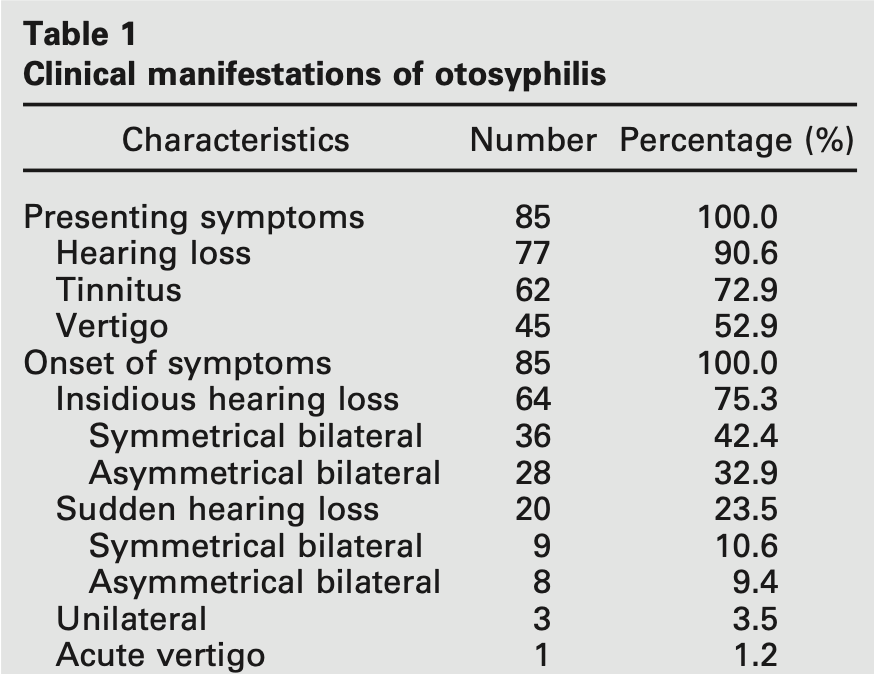
Fayad and Linthicum (Fayad and Linthicum 1999) state that, “Vestibular disturbances could be present in as many as 80% of patients with otosyphilis.”
Mishra and colleagues (Mishra et al. 2008) studied 8 patients with otosyphilis and concomitant HIV infection and reported that all complained of hearing loss, while 7 (88%) complained of tinnitus.
Physical examination
Patients with otosyphilis generally have sensorineural hearing loss, which may be unilateral or bilateral.
Ocular motor examination
There are few reports in the literature of symptomatic otosyphilis patients exhibiting nystagmus. Klemm and Wollina (Klemm and Wollina 2004) described a patient with spontaneous and positional nystagmus.
Testing: auditory
Ramchandani and colleagues (Ramchandani et al. 2020) comment that:
“As a general rule, otosyphilis in adults causes SNHL [sensorineural hearing loss], although conductive hearing loss may be present in those with long-standing disease. Hearing loss can be unilateral or bilateral, often with sudden onset and rapid progression, and those patients who report unilateral impairment may have bilateral disease on audiogram. Bilateral hearing loss may be symmetric or asymmetric and can present in a variety of ways: mild or moderate and low to high frequency with poor or excellent speech discrimination scores. There is not one classic type of presentation” (Ramchandani et al. 2020).
In other words, no pattern of hearing loss is sensitive or specific for otosyphilis.
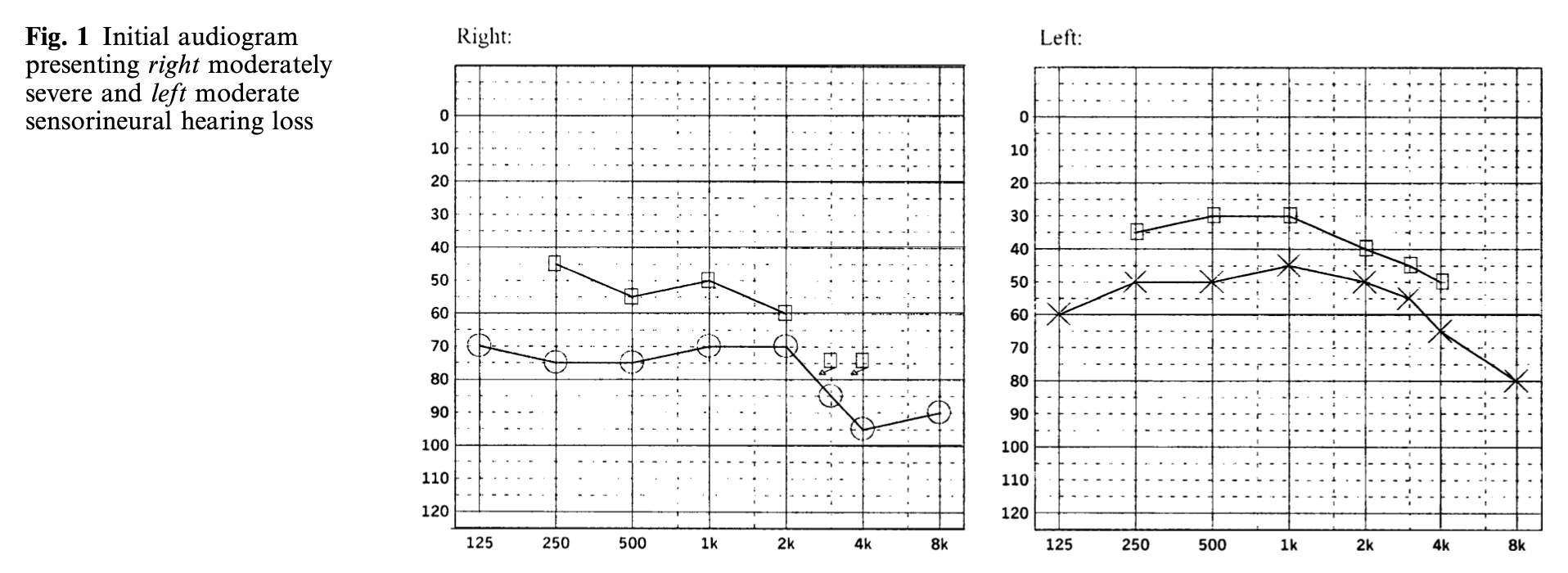
The Figure below, from Song and colleagues (Song et al. 2005), shows audiometry from a case of otosyphilis.
Lowhagen and colleagues (Lowhagen et al. 1983) studied 26 patients with secondary or early latent syphilis and found that 7 (27%) had abnormal brainstem auditory evoked responses.
Testing: vestibular
Very few publications report results of vestibular tests in otosyphilis.
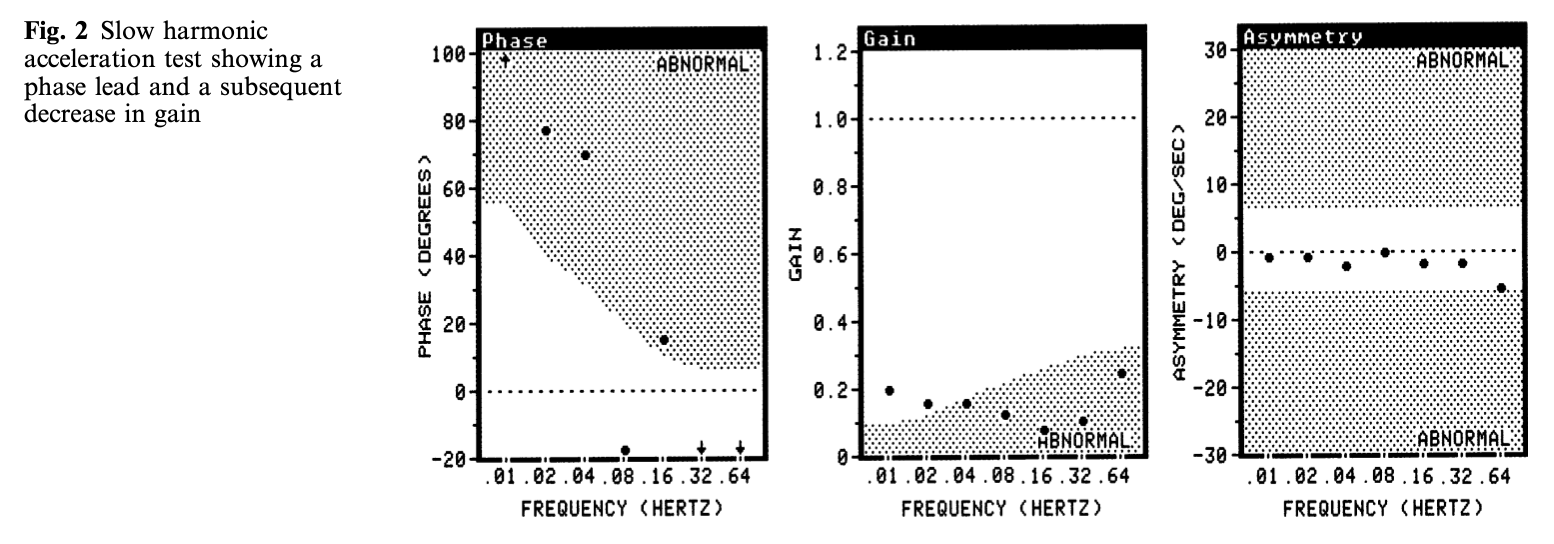
Song and colleagues (Song et al. 2005) reported the case of a patient with bilateral otosyphilitic involvement. They performed rotatory chair testing (see the Figure below) and interpreted the slow harmonic acceleration as showing, “bilateral total vestibular function loss.”
Testing: other
A diagnosis of syphilis is usually secured by checking treponemal tests (e.g., fluorescent treponemal antibody absorption) and non-treponemal tests (venereal disease research laboratory).
Imaging
Otosyphilis can cause cranial osteolytic lesions that involve the labyrinth. The Figure below, from Hosseini and colleagues (Hosseini et al. 2021), shows images from a temporal bone CT of such a case.
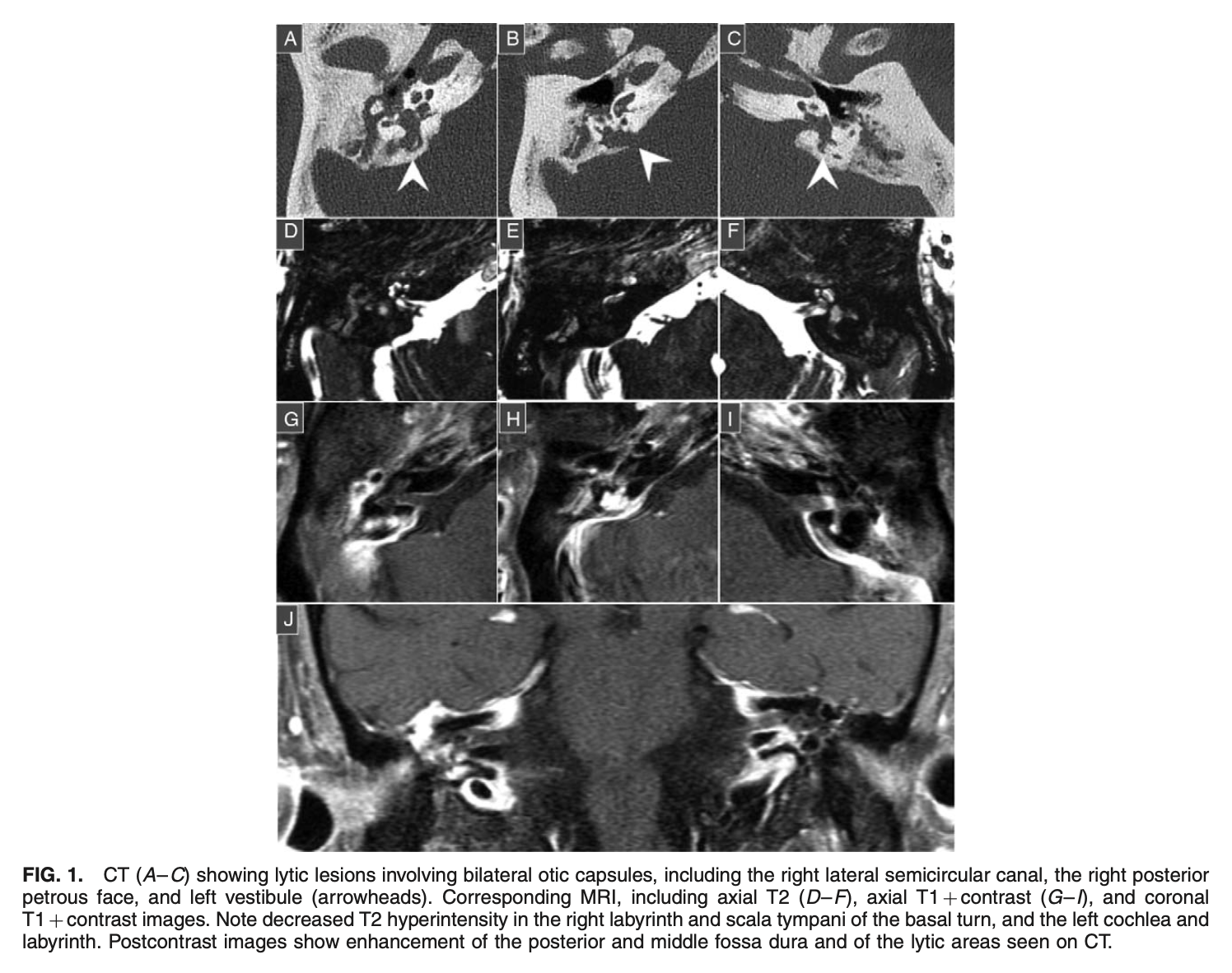
Similar CT findings are reported in other cases in the literature (Ogungbemi et al. 2014; Sonne et al. 2002).
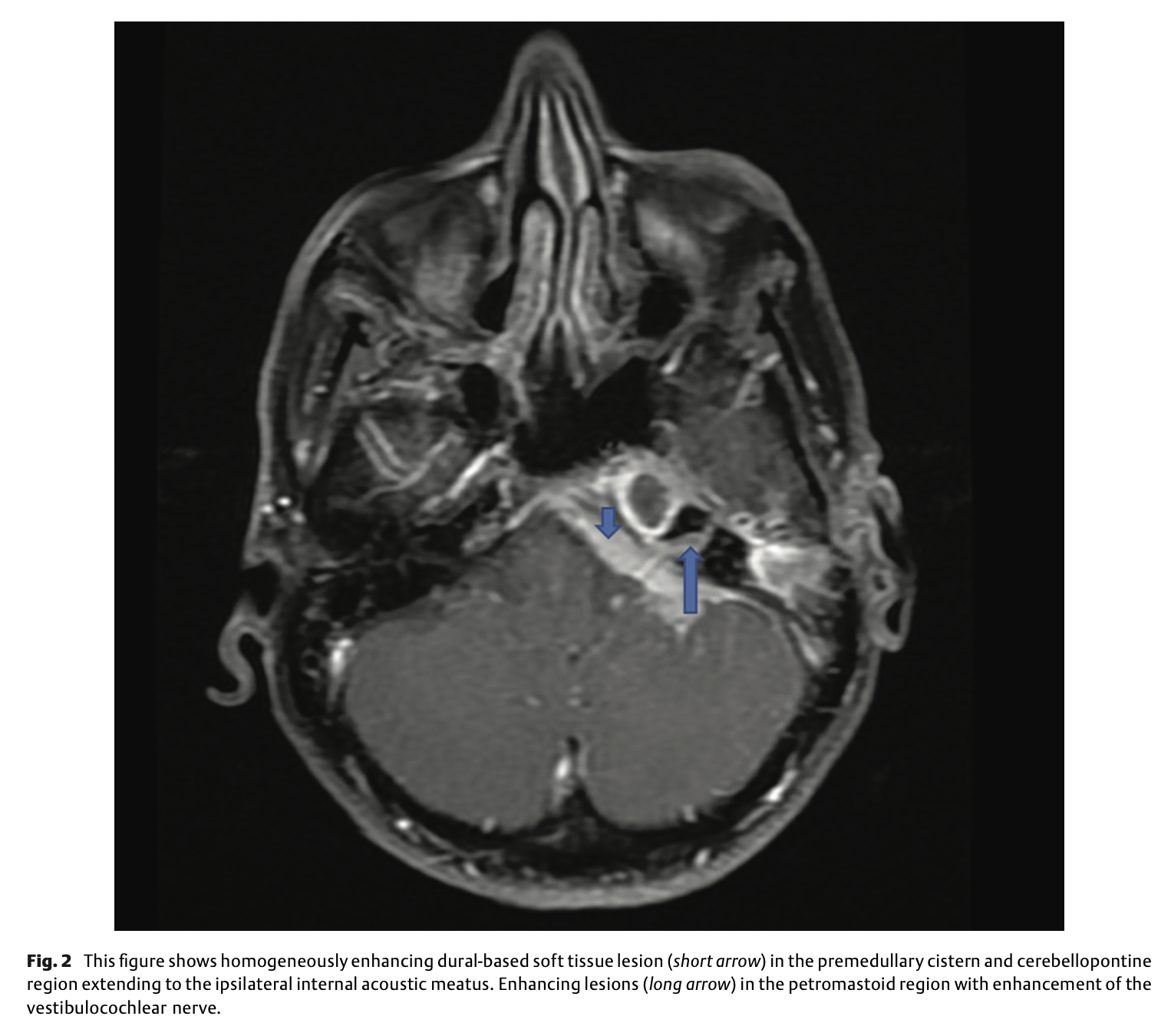
Otosyphilis can also manifest as a space-occupying intracranial gumma (Little et al. 1995) impinging on audiovestibular structures. The Figure below, from Chandrasekharan and colleagues (Chandrasekharan et al. 2022), shows an axial MRI of such a case.
Histopathology
Very few temporal bone studies of patients with otosyphilis have been published (Fayad and Linthicum 1999).
Differential diagnosis
Otosyphilis can present similarly to autoimmune inner ear disease (Garcia-Berrocal et al. 2006) and Ménière’s disease (Fayad and Linthicum 1999).
Note that syphilis can impair equilibrium through other mechanisms besides labyrinthine involvement. In particular, neurosyphilis can cause tabes dorsalis (degeneration of the posterior columns of the spinal cord) which impairs large fiber sensation (vibration and proprioception), leading to a sensory ataxia.
Treatment
Treatment of otosyphilis is treatment of syphilis itself. Treatment is usually supervised by an internist or infectious disease specialist, and commonly involves intramuscular penicillin with oral probenecid, or intravenous penicillin (Ramchandani et al. 2020).
Prognosis
Treatment of syphilis may reverse hearing loss in some cases of otosyphilis (Etemady-Deylamy and Abate 2022; He et al. 2022; Sarsak et al. 2023), though this has not been studied systematically.
Traidl and colleagues (Traidl et al. 2021), citing data from Yimtae and colleagues (Traidl et al. 2021), state that, “in a retrospective analysis of 206 patients only 6.6% revealed an improvement of the hearing symptoms after treatment.” In some cases the improvement in hearing is not sustained (Dobbin and Perkins 1983).
The Figure below, from Etemady-Deylamy and Abate (Etemady-Deylamy and Abate 2022), shows improvement in left-sided sensorineural hearing loss on audiometry from before treatment (left panel) and after treatment (right panel).
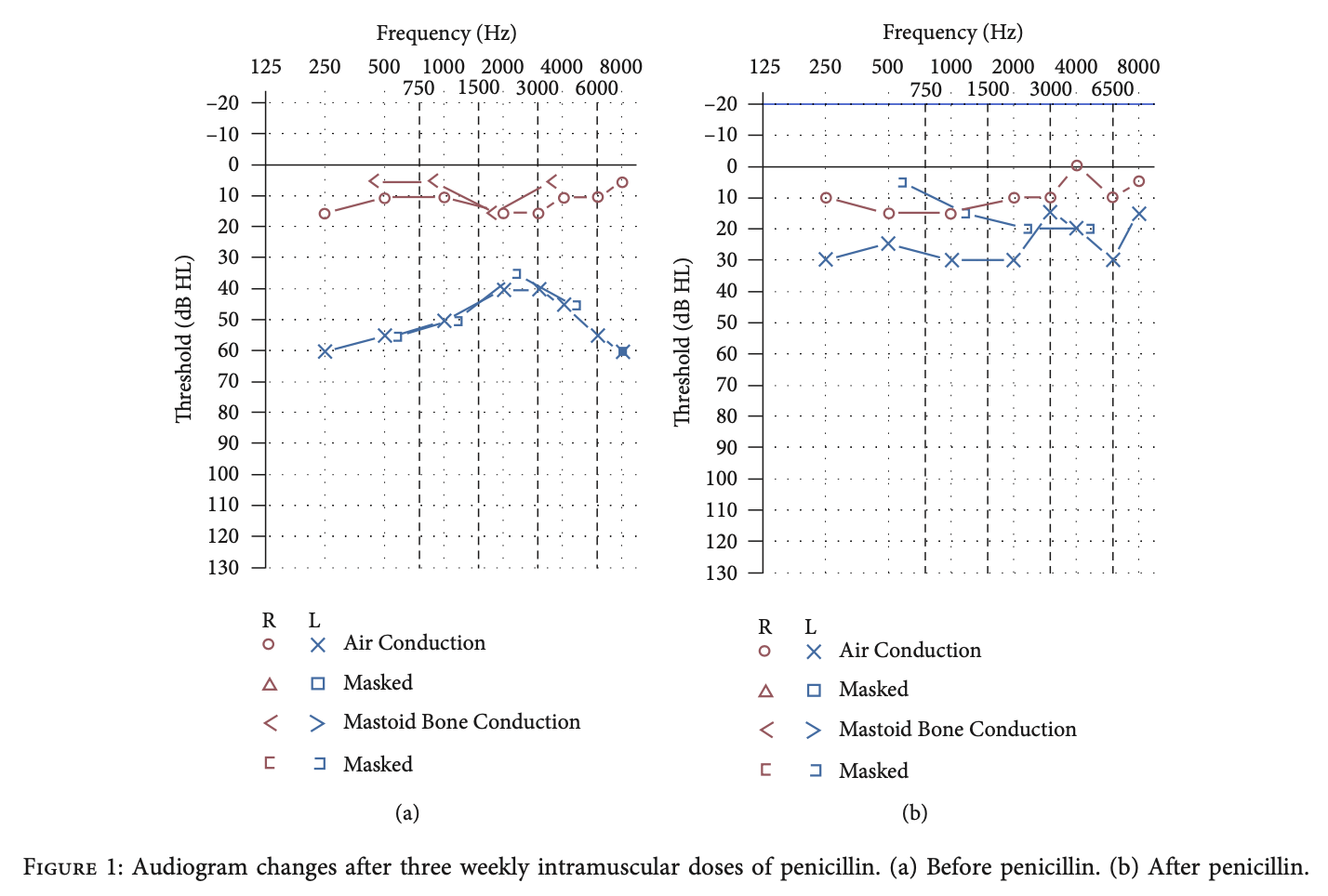
In the case described by Etemady-Deylamy and Abate (Etemady-Deylamy and Abate 2022), the patient also presented with “vertigo,” and this had resolved at 6 months after treatment.
Klemm and Wollina (Klemm and Wollina 2004) described a patient with spontaneous and positional nystagmus that completely remitted after treatment.
References
Carlson JA, Dabiri G, Cribier B, Sell S (2011) The immunopathobiology of syphilis: the manifestations and course of syphilis are determined by the level of delayed-type hypersensitivity. Am J Dermatopathol 33: 433-60. doi: 10.1097/DAD.0b013e3181e8b587
Chandrasekharan R, Kulkarni C, Pullara SK, Moorthy S (2022) Magnetic Resonance Imaging in Otosyphilis: A Rare Manifestation of Neurosyphilis. Indian J Radiol Imaging 32: 278-284. doi: 10.1055/s-0042-1744523
Dobbin JM, Perkins JH (1983) Otosyphilis and hearing loss: response to penicillin and steroid therapy. Laryngoscope 93: 1540-3. doi: 10.1288/00005537-198312000-00003
Dombrowski JC, Pedersen R, Marra CM, Kerani RP, Golden MR (2015) Prevalence Estimates of Complicated Syphilis. Sex Transm Dis 42: 702-4. doi: 10.1097/OLQ.0000000000000368
Etemady-Deylamy A, Abate G (2022) Otosyphilis with Clinical and Serologic Responses with Weekly Intramuscular Penicillin: A Case Report and Literature Review. Case Rep Infect Dis 2022: 3152383. doi: 10.1155/2022/3152383
Fayad JN, Linthicum FH, Jr. (1999) Temporal bone histopathology case of the month: otosyphilis. Am J Otol 20: 259-60.
Garcia-Berrocal JR, Gorriz C, Ramirez-Camacho R, Trinidad A, Ibanez A, Rodriguez Valiente A, Gonzalez JA (2006) Otosyphilis mimics immune disorders of the inner ear. Acta Otolaryngol 126: 679-84. doi: 10.1080/00016480500491994
He S, Messner AH, Mirani G (2022) Otosyphilis: A Rare Cause of Reversible Hearing Loss in a Teenage Male. Cureus 14: e23468. doi: 10.7759/cureus.23468
Hosseini DK, Aaron KA, Alyono JC (2021) Hearing Loss Due to Otosyphilis: Imaging Case of the Month. Otol Neurotol 42: e1634-e1635. doi: 10.1097/MAO.0000000000003244
Hungerbuhler JP, Regli F (1978) Cochleovestibular involvement as the first sign of syphilis. J Neurol 219: 199-204. doi: 10.1007/BF00314535
Jones-Vanderleest JG (2022) Neurosyphilis, Ocular Syphilis, and Otosyphilis: Detection and Treatment. Am Fam Physician 106: 122-123.
Klemm E, Wollina U (2004) Otosyphilis: report on six cases. J Eur Acad Dermatol Venereol 18: 429-34. doi: 10.1111/j.1468-3083.2004.00939.x
Little JP, Gardner G, Acker JD, Land MA (1995) Otosyphilis in a patient with human immunodeficiency virus: internal auditory canal gumma. Otolaryngol Head Neck Surg 112: 488-92. doi: 10.1016/S0194-59989570292-X
Lowhagen GB, Rosenhall U, Andersson M, Blomstrand C, Lindholm L, Roupe G (1983) Central nervous system involvement in early syphilis. Part II. Correlation between auditory brain stem responses (ABR) and cerebrospinal fluid abnormalities. Acta Derm Venereol 63: 530-5.
Mishra S, Walmsley SL, Loutfy MR, Kaul R, Logue KJ, Gold WL (2008) Otosyphilis in HIV-coinfected individuals: a case series from Toronto, Canada. AIDS Patient Care STDS 22: 213-9. doi: 10.1089/apc.2007.0019
Ogungbemi A, Dudau C, Morley S, Beale T (2014) Computed tomography features of luetic osteitis (otosyphilis) of the temporal bone. J Laryngol Otol 128: 185-8. doi: 10.1017/S0022215113003575
Papalini C, Cagini C, Ricci G, Pasticci MB (2017) Ocular and oto-syphilis: not a thing of the past. Infection 45: 725-726. doi: 10.1007/s15010-017-1019-y
Ramchandani MS, Litvack JR, Marra CM (2020) Otosyphilis: A Review of the Literature. Sex Transm Dis 47: 296-300. doi: 10.1097/OLQ.0000000000001155
Sarsak EW, Omer WE, Al Bishawi AA, Maslamani MA, Abdulmajed AAB (2023) Otosyphilis: A rare case of reversible hearing loss in a young man with secondary syphilis. IDCases 31: e01666. doi: 10.1016/j.idcr.2022.e01666
Song JJ, Lee HM, Chae SW, Hwang SJ (2005) Bilateral otosyphilis in a patient with HIV infection. Eur Arch Otorhinolaryngol 262: 972-4. doi: 10.1007/s00405-005-0934-1
Sonne JE, Zeifer B, Linstrom C (2002) Manifestations of otosyphilis as visualized with computed tomography. Otol Neurotol 23: 806-7. doi: 10.1097/00129492-200209000-00033
Theeuwen H, Whipple M, Litvack JR (2019) Otosyphilis: Resurgence of an Old Disease. Laryngoscope 129: 1680-1684. doi: 10.1002/lary.27635
Traidl S, Angela Y, Stender A, Kulberg A, Tronnier M, Prenzler NK, Wattjes MP, Kapp A, Stangel M, Schacht V, Werfel T (2021) A rare case of neuro- and otosyphilis in secondary syphilis. J Eur Acad Dermatol Venereol 35: e823-e826. doi: 10.1111/jdv.17512
Yimtae K, Srirompotong S, Lertsukprasert K (2007) Otosyphilis: a review of 85 cases. Otolaryngol Head Neck Surg 136: 67-71. doi: 10.1016/j.otohns.2006.08.026
![]()