By Marcello Cherchi, MD PhD
For patients
Some psychological problems can manifest with the symptom of disequilibrium. Disequilibrium can, in turn, cause or worsen psychological symptoms. In patients with a combination of these symptoms, it is medically reasonable to check several tests of balance function in order to assess whether there is a diagnosable inner ear cause of disequilibrium that might merit its own treatment. In most cases, consultation with psychiatry is helpful in order to “break” the vicious cycle that these symptoms may otherwise establish.
For clinicians
Overview
Disequilibrium can occur in conjunction with psychiatric illness. We refer to this as “psychologic disequilibrium” in order to remain neutral with respect to the direction of causality. Several factors make this topic difficult to study, including the variability of presentation, but there is some evidence that primary otovestibular disorders can provoke psychological symptoms, and evidence that psychiatric disease can cause symptoms of disequilibrium. It is plausible that many cases involve variable overlap and variable directionality of causation. We find explanatory frameworks based on internal modeling compelling. Vestibular testing of patients with anxiety and panic disorder report variable abnormalities, but none is sensitive or specific for these psychiatric diagnoses, and in our view such findings should prompt a search for primary otovestibular disorders. Practically, since psychiatric disease and the symptom of disequilibrium can be mutually reinforcing, we encourage psychiatric consultation with the goal of interrupting this maladaptive positive feedback loop.
Introduction
Although Sigmund Freud (1856 – 1939) is generally known as the founder of psychoanalysis, his training was as a neurologist at the University of Vienna. In 1895 he published a paper entitled, “On the grounds for detaching a particular syndrome from neurasthenia under the description ‘anxiety neurosis’” (Freud 1964 (1895)), in which he stated:
“‘Vertigo’ occupies a prominent place in the group of symptoms of anxiety neurosis. In its mildest form it is best described as ‘giddiness’; in its severer manifestations, as ‘attacks of vertigo’ (with or without anxiety), it must be classed among the gravest symptoms of the neurosis. The vertigo of anxiety neurosis is not rotatory nor does it especially affect certain planes or directions, like Meniere’s vertigo. It belongs to the class of locomotor or co-ordinatory vertigo, as does the vertigo in oculomotor paralysis. It consists in a specific state of discomfort, accompanied by sensations of the ground rocking, of the legs giving way and of its being impossible to stand up any more; while the legs feel as heavy as lead and tremble or the knees bend. This vertigo never leads to a fall.”
Freud was probably not the first to propose the idea of a relationship between psychological factors and the somatic symptom of “vertigo.” In the past few decades there have been numerous other attempts to characterize this relationship, with a variety of nomenclatures referencing a variety of symptoms, putative causes and putative effects.
What framework can we use to approach this issue?
A dichotomous nosology is probably not helpful
As we discuss elsewhere, the various terms subsumed under the concept of disequilibrium have, at best, marginal diagnostic value in themselves. Conceptually we find it helpful to regard the perception of disequilibrium as an “output,” and the underlying etiology of that symptom as the “input.” There is an extraordinary array of disorders (“inputs”) that can lead to the symptom (“output”) of disequilibrium.
During the process of evaluating a patient we prefer to use the relatively neutral phrase “psychologic disequilibrium” to reflect that there may be a relationship between psychological factors and the symptom of disequilibrium, without claiming that the relationship is causal (in either direction). We prefer to avoid the term “psychogenic disequilibrium” because this implies (even before a diagnosis has been established) that psychological factors are the cause (“‑genic”) of the symptom of disequilibrium, when they may ultimately turn out not to be so. We also prefer to avoid the term “psychiatric disequilibrium” (Furman and Jacob 1997) because this implies that the underlying psychological experience is pathological or requires treatment (“‑iatric”), which it may ultimately turn out not to be.
Furthermore, we would concur with authors who caution against imposing a dichotomous nosology on this problem. For example:
- “A categorical classification of dizziness does not fully appreciate how these conditions occur together and interact” (Clark et al. 1994).
- Jacob and Furman believe that it is flawed to regard these symptoms as “either organic [meaning with a detectable physiologic source] or psychogenic but not both” (Jacob and Furman 2001).
- “The traditional dichotomous classification of vestibular symptoms as ‘organic’ or ‘psychogenic’ is unworkable” (Dieterich et al. 2016).
Finally, Dieterich and colleagues (Dieterich et al. 2016) comment that:
“Psychiatric disorders may be the primary causes or secondary complications of vestibular syndromes. Primary psychiatric disorders occur without other preceding vestibular syndromes. Secondary psychiatric disorders develop after the onset of primary vestibular disorders and often outlast their remission. In some cases, psychiatric disorders occur first, but do not manifest vertigo, unsteadiness, or dizziness. Then, with the onset of a vestibular disorder, they increase in severity and contribute to overall morbidity in an interactive manner. Psychiatric disorders also may trigger functional vestibular syndromes such as PPV [phobic postural vertigo] or CSD [chronic subjective dizziness]” (Dieterich et al. 2016).
There are compelling data to suggest that psychological factors (in isolation) can cause the symptom of disequilibrium, and equally compelling data to suggest that the perception of disequilibrium can cause psychological symptoms. A study by Staab and Ruckenstein (Staab and Ruckenstein 2003) concluded:
“These data support the hypothesis that physical neurotologic conditions may trigger psychopathy as often as primary anxiety disorders cause dizziness. A third pattern appears to be equally common wherein physical neurotologic conditions exacerbate preexisting psychiatric illnesses… There is a bidirectional relationship between neurotologic conditions and psychiatric disorders” (Staab and Ruckenstein 2003).
In other words, it is likely that many cases have a mix of directionality.
A more nuanced nosology is appropriate
Furman and Jacob published and revised a “taxonomy” of disequilibrium and psychiatric factors in the context of otoneurology (Furman and Jacob 1997, 2001; Jacob and Furman 2001), selections of which are illustrated in the Figures below.
|
Figure 1: A taxonomy of dizziness, focusing on the intersection between otovestibular disorders and psychiatric disorders. From Furman and Jacob (1997). |
Figure 2: A taxonomy of dizziness, focusing on the intersection between otovestibular disorders and psychiatric disorders. From Furman and Jacob (2001). |
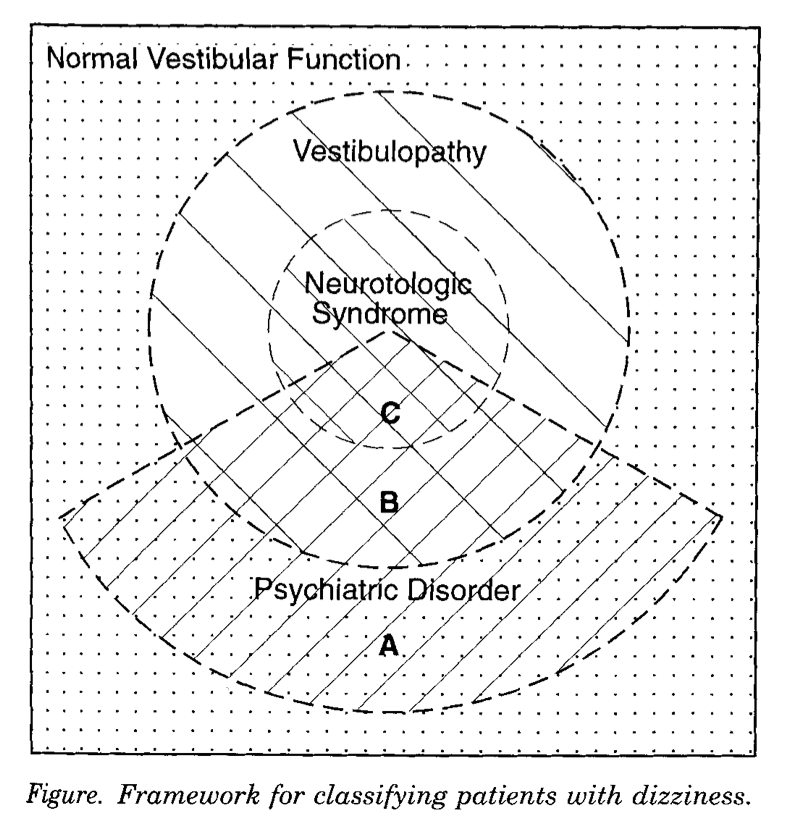
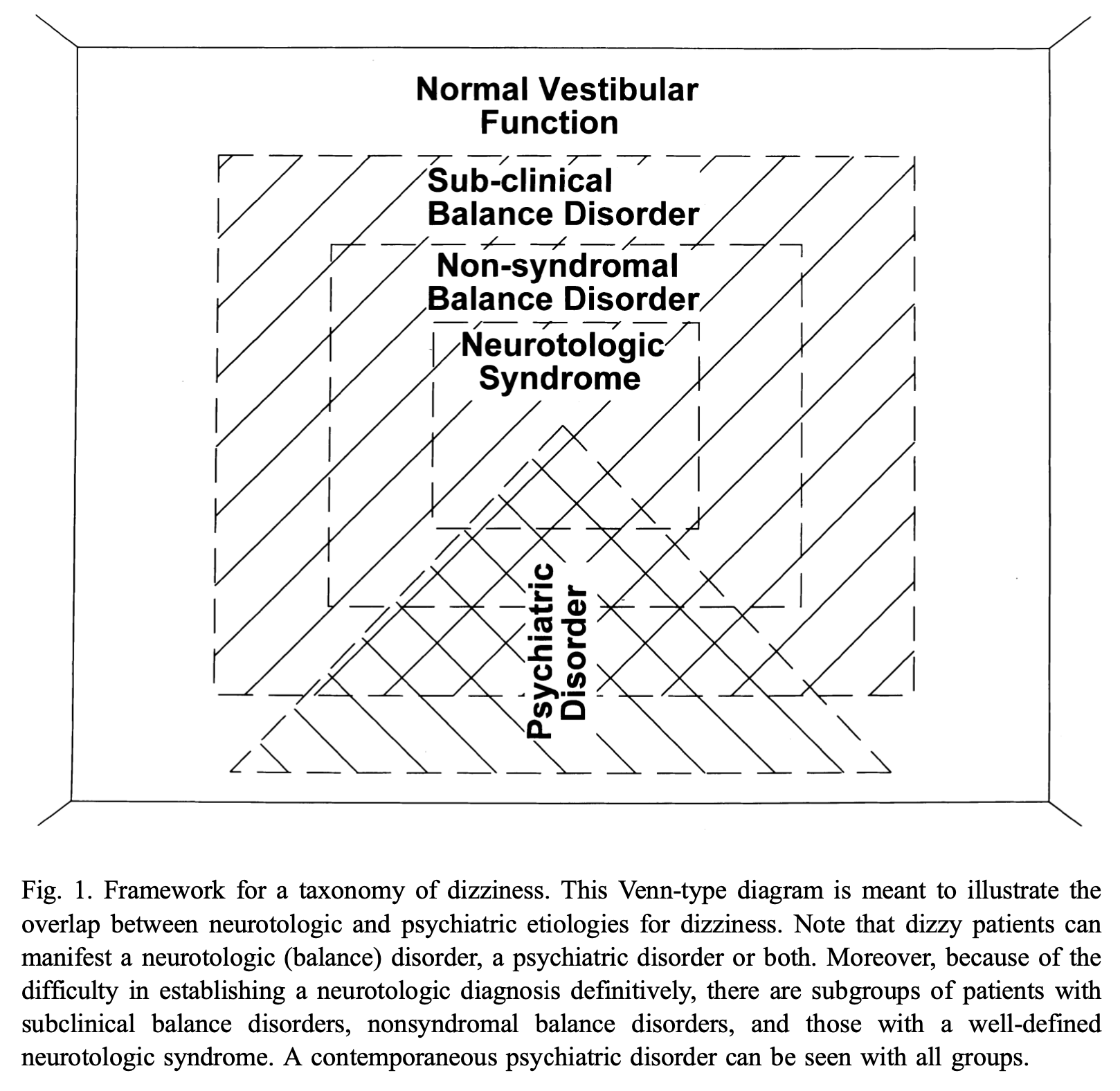
The progression in their thinking was essentially one of increasing granularity of detectable otoneurological conditions. The organization of concentric rectangles in the final iteration (Furman and Jacob 2001) is articulated elsewhere (Jacob and Furman 2001) as follows, progressing from innermost to outermost:
- “Syndromal vestibular disorders, e.g., Ménière’s disease and benign paroxysmal positional vertigo.”
- “Non-syndromal vestibular disorders, i.e., abnormal laboratory vestibular testing, dizziness symptoms, and ancillary testing, e.g., magnetic resonance imaging, which do not fit into a pattern of a specific syndrome.”
- “Subclinical vestibular disorders, i.e., symptoms suggestive of vestibular dysfunction without vestibular laboratory abnormalities.”
- “No vestibular disorder, i.e., medical disorders such as orthostatic hypotension and certain psychiatric disorders.”
Furman and Jacob (Furman and Jacob 2001) offer a alternative graphic representation of these relationships which may be more instructive, as illustrated in the Figures below. They describe this as depicting a, “Framework for interface between balance disorders and psychiatric disorders. The interface between balance disorders and psychiatric disorders is depicted as several levels of interaction ranging from noncoexistant disorders to a complete overlap in pathophysiology” (Furman and Jacob 2001).
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
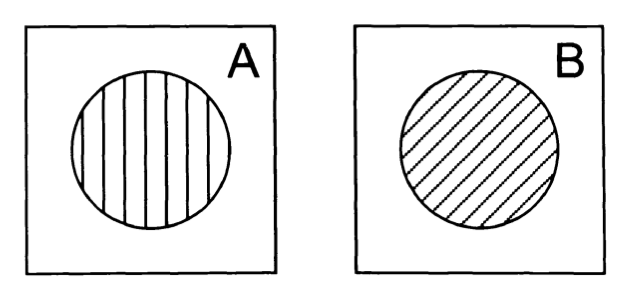
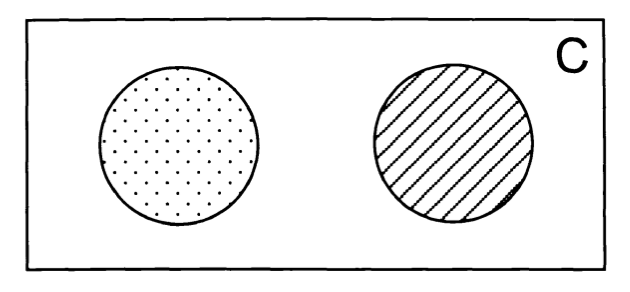
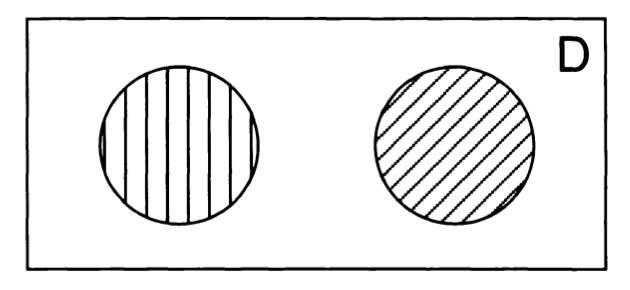
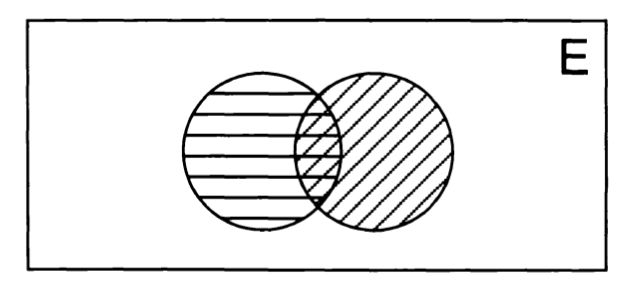
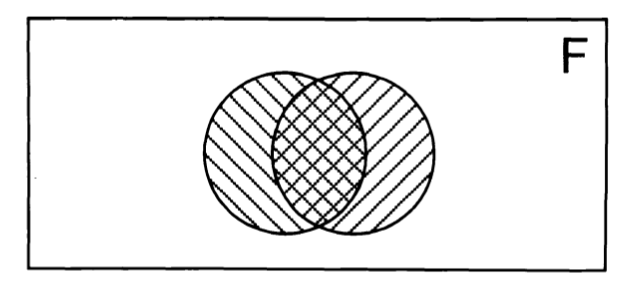
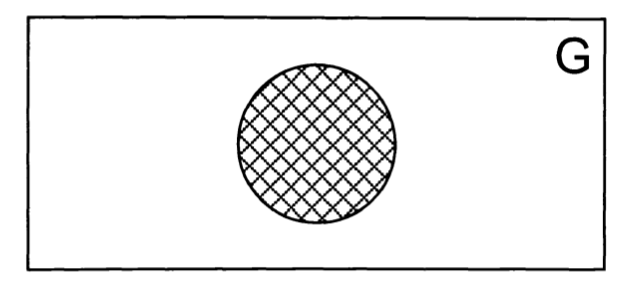
Ultimately these levels are intended to convey a gradation of overlap between symptoms (disequilibrium, psychological symptoms) and pathologies (otovestibular disorders, psychiatric disease) without making claims pertaining to causality. Other investigators have proposed classifications that are similar in spirit (Clark et al. 1994).
The culmination of these gradations of overlap is that by the final point on the scale (corresponding to the outermost space in the Figures presented earlier), there is no detectable otovestibular or other medical pathology that would manifest with a perceived disturbance of disequilibrium, and thus by exclusion the symptom of disequilibrium must be associated exclusively with a psychological process. Is this the point at which terms such as “psychogenic disequilibrium” or “psychiatric disequilibrium” would be appropriate? We would argue that such terms are still inappropriate for two reasons.
First, Furman and Jacob (Furman and Jacob 1997) add the following humbling reminders of the limitations that experience and technology impose on our diagnostic capabilities:
“The diagnosis of a defined neurotologic syndrome depends on the knowledge and expertise of the treating physician and the availability of a vestibular laboratory. The boundary between vestibulopathy and normal vestibular function is similarly fluid, because the probability of uncovering objective findings depends on the composition of the battery of vestibular tests included in the assessment. In particular, negative findings on physical examination and laboratory testing do not guarantee normality. Clinical vestibular tests leave large areas of the vestibular system unexamined” (Furman and Jacob 1997).
In other words, as knowledge and technology advance (Cherchi and Yacovino 2021), it is likely that previously undetectable vestibular pathology will become identifiable. Therefore, we would hesitate to commit to the term “psychogenic” disequilibrium.
Second, not all psychological experiences should be classified as pathological. There are life circumstances in which it is unsurprising to experience emotions compatible with formal diagnoses of depression, anxiety, etc. Therefore, we would hesitate to employ the term “psychiatric” disequilibrium, because would suggest that the emotional experience merits treatment.
Pathophysiological mechanism of disease: consider internal models
Despite everything we have just discussed, there remains the reasonable possibility that there are instances in which the symptom of disequilibrium is due exclusively to psychological factors and nothing else.
Even though we may not yet be in a position to identify such cases with complete confidence, it is certainly plausible that such instances exist, analogous to somatization disorders. So, if this is the case, what is a plausible mechanism?
At a general level, “Vestibular and anxiety disorders are related via both somatopsychic and psychosomatic mechanisms, and also are linked via overlapping neural circuits” (Jacob and Furman 2001), but this concept is so broad that it affords little possibility of any deeper understanding.
The Figure below, originally from Brandt (Brandt 1996) and later modified in Dieterich and Staab (Dieterich et al. 2016), shows an early version of how “phobic postural vertigo” could arise from a mismatch between planned motion (“efference copy”) and perception of actual motion (“afference”).
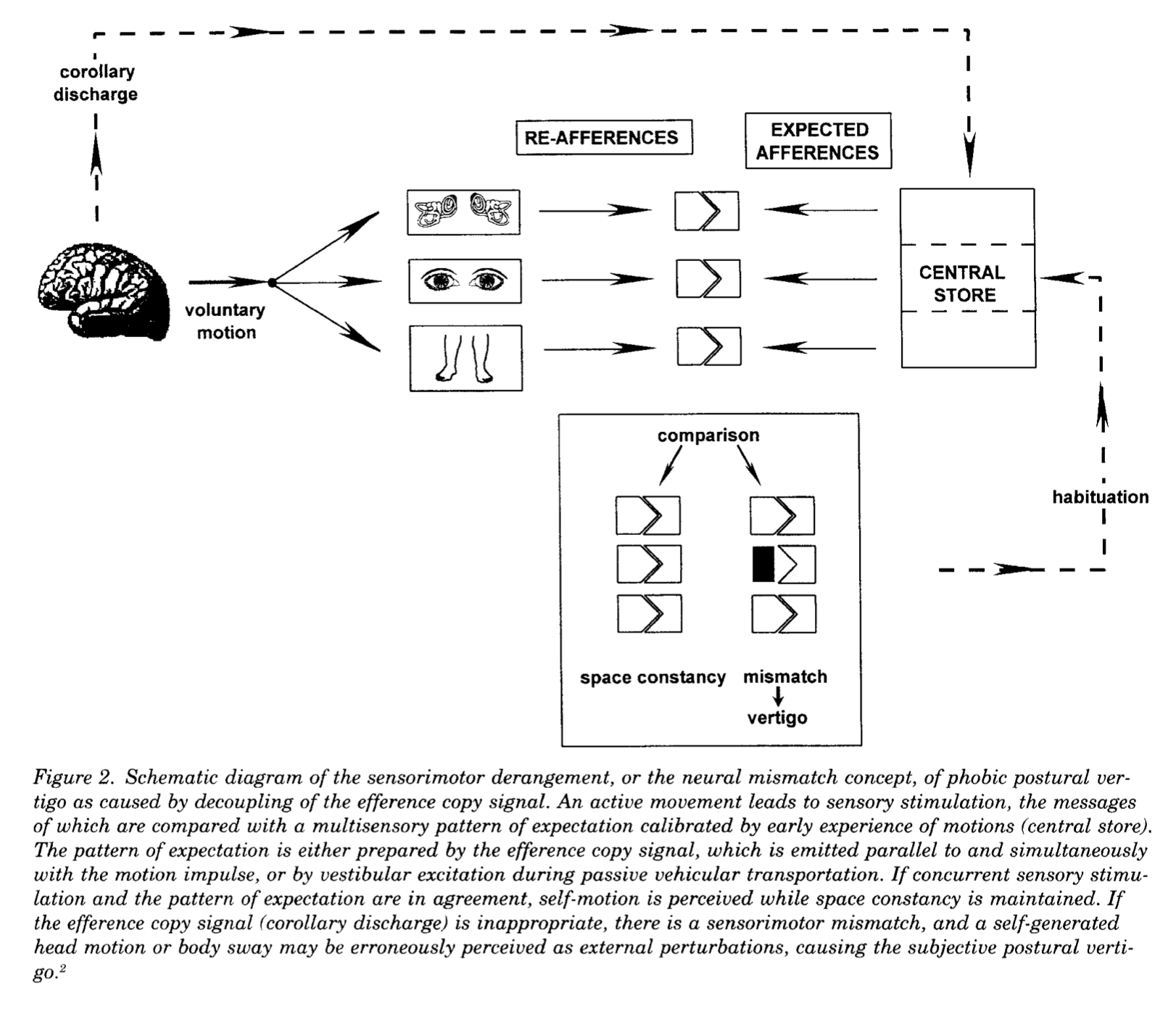
Broadly speaking this idea relies on a movement illusion (in the medical sense), meaning misperception of an actual stimulus.
But what about perception of motion in the absence of any such stimulus? In medical terms this would be classified as a movement hallucination, meaning perception in the absence of any stimulus. Reuten and colleagues (Reuten et al. 2022) construct a persuasive argument for an explanatory model of this. They begin by reviewing data from other research demonstrating that cognitive factors influence vestibular perceptions (Ferre and Haggard 2020; Ferre and Harris 2015; Mast and Ellis 2015), and specifically that perception of actual motion can be modulated by a variety of factors including mental imagery (Mertz et al. 2000; Nigmatullina et al. 2015), expectations (Ellis et al. 2017) and contextual information (D’Amour et al. 2021; Riecke 2009; Wertheim et al. 2001). They reasoned that:
“These studies all concerned experiments with motion stimuli and thus reflect modulations of a percept of self-motion that is elicited by sensory stimulation. Because we are not aware of any study on self-motion perception without a motion stimulus, we performed a study investigating whether cognitive cues can elicit a percept of self-motion in the absence of sensory motion. In specific, we minimized physical (inertial), visual, somatosensory and auditory cues about self-motion” (Reuten et al. 2022).
Their experiments demonstrated that, indeed, it is possible to elicit (using various cognitive cues) perception of motion even in the absence of any true movement (and thus without stimulating any vestibular input). In order to unify findings from previous research (showing that cognitive factors could modulate perception of actual movement) with their own research (showing that cognitive factors could provoke perception of movement in the absence of any such movement), they proposed that the underlying mechanism has to do with internal modeling (Peterka 2018). Reuten and colleagues (Reuten et al. 2022) provide a schematic summary of this idea in the Figure below.
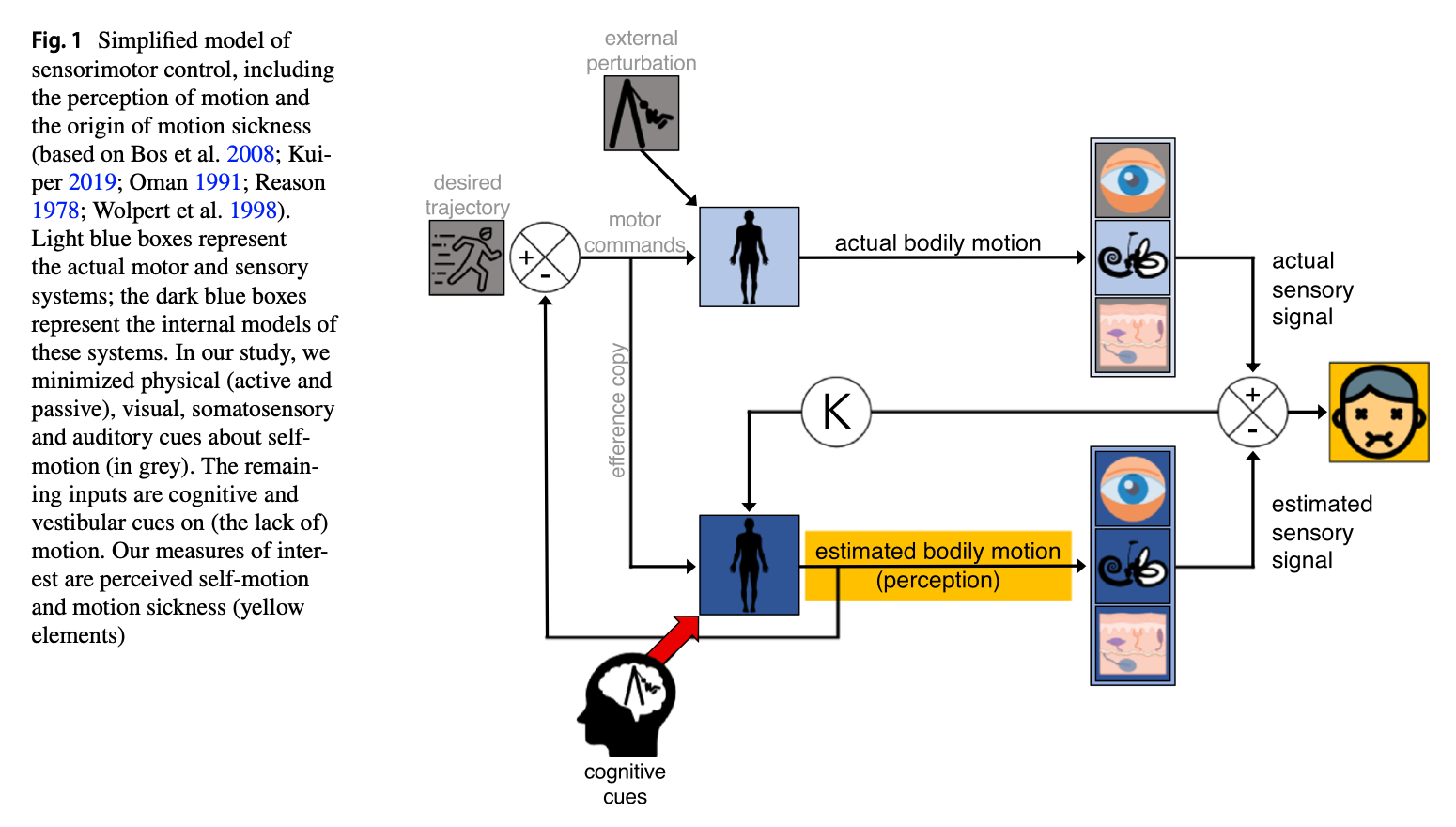
They explain their model as follows:
“The internal model of the bodily dynamics (dark blue box) estimates the bodily motion that would result from the motor commands. This estimation controls our perception of self-motion. Under optimal conditions, it equals the actual self-motion produced by the real body (light blue box). As this prediction lacks the delay and other peculiarities of the sensorimotor system, it is the best input for feedback control of self-motion. To ensure that this estimate is indeed accurate, this signal is fed to the internal model predicting the sensory signals (visual, vestibular, and somatosensory; dark blue). If there is a difference between the resulting integrated estimated and actual sensory signal, their discrepancy will be used to update the internal model and hence the estimated bodily motion… The updating of the internal model is weighted relative to the noise of the actual sensory systems by a gain K. A high uncertainty about those signals is then accounted for by a low gain and, vice versa, a low uncertainty by a high gain. In the current study, we are interested whether not only efference copies but also motion expectations generated by cognitive cues influence the estimated bodily motion. Given that the updating of the internal model is based on a Kalman gain, motion will only be reported when there is a low signal to noise ratio of the senses. If so, cognitive cues could result in the perception of self-motion in the actual absence of motion” (Reuten et al. 2022).
We find this model compelling, as it dovetails with other research regarding internal modeling (Francis and Wonham 1976) as applied to sensorimotor control (Wolpert et al. 1995).
Epidemiology
The epidemiology of psychological disequilibrium has been difficult to estimate. Ardic and Atesci comment on the broad range of estimates: “The ratio of the patients with psychogenic dizziness reported in different studies varies between 9 and 55%” (Ardic and Atesci 2006). This range is likely due to differences in methodology and to the lack of uniformity in definitions between studies.
Additional factors that complicate such estimations include the relative timing of the symptoms, and different assumptions regarding causality. Dieterich and Staab (Dieterich et al. 2016) comment:
“Retrospective, cross-sectional, and prospective studies conducted over three decades suggest that 8–10% of patients with vestibular symptoms have an anxiety or depressive disorder as the primary cause of their ill- ness. One in eight will develop a de novo anxiety or depressive disorder triggered by an acute vestibular disease, and a total of 30–50% will manifest anxiety or depressive morbidity over the course of their vestibular illness. Another 15–20% will primarily manifest the functional vestibular syndromes of PPV [phobic postural vertigo] or CSD [chronic subjective dizziness]. Thus, functional and psychiatric disorders may be primary, secondary, or comorbid problems in many patients presenting for evaluation of vestibular symptoms. In other words, these conditions are common causes, consequences, and complications of vestibular symptoms” (Dieterich et al. 2016).
Clinical presentation
Some researchers conclude that a patient’s description of symptoms alone can successfully discriminate psychological disequilibrium from “otologic” disequilibrium (Clark et al. 1994).
Other authors are more cautious in this regard. For example, Dieterich and collagues (Dieterich et al. 2016) comment that:
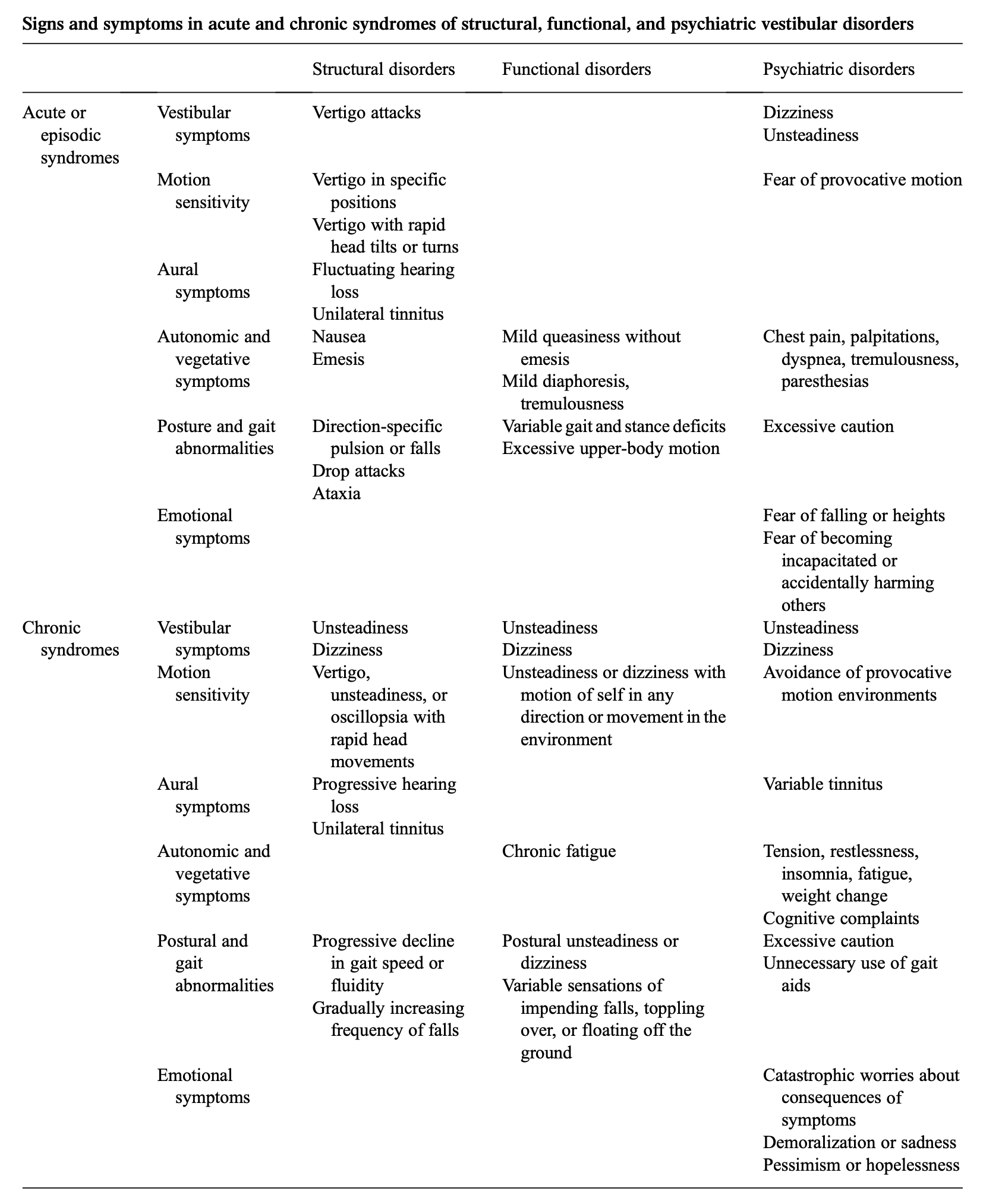
“The clinical history is paramount because functional and psychiatric vestibular disorders are diagnosed by history. There are no single pathognomonic symptoms for these illnesses, but key elements of clinical history are more common in structural versus functional versus psychiatric syndromes. Combinations of symptoms and their temporal associations are keys to properly making (i.e., ruling in) diagnoses. Importantly, however, the existence of features in one category does not exclude disorders in other categories from consideration. High rates of comorbidity make it impossible to use the presence of one set of features to eliminate (i.e., rule out) other illnesses” (Dieterich et al. 2016).
To this end, Dieterich and colleagues (Dieterich et al. 2016) offer the following Table comparing symptom tendencies in “structural disorders,” “functional disorders” and “psychiatric disorders.”
Finally, the clinician should bear in mind that these symptoms are protean:
“Patients’ dominant symptoms may change over time as one disorder begets another, so it is important to follow the temporal evolution of their illnesses. Misattribution of all symptoms to the initial illnesses may incorrectly keep the focus of diagnostic evaluations and treatment on those conditions, even if they have remitted” (Dieterich et al. 2016).
Testing: vestibular
Several studies have exposed patients with anxiety to various optic stimuli and identified increased sway on static posturography compared to healthy controls (Jacob et al. 1995; Redfern et al. 2007).
Several studies have explored vestibular tests in patients with panic disorder. Hoffman and colleagues studied vestibular autorotation tests in 19 patients diagnosed with panic disorder and reported asymmetries in vestibulo-ocular reflex gain in 100% of patients (Hoffman et al. 1994). Jacob and colleagues (Jacob et al. 1996) studied patients with variable combinations of panic disorder, anxiety, depression and agoraphobia and reported that, “Vestibular abnormalities were common in all the groups but most prevalent in the patients with panic disorder with moderate to severe agoraphobia.” Jacob and colleagues (Jacob et al. 1997) studied computerized dynamic posturography in patients with variable combinations of panic disorder, anxiety, depression and agoraphobia and reported that, “Agoraphobics rely on proprioceptive cues for maintenance of upright balance.” Jacob and colleagues (Jacob et al. 1985) studied several vestibular tests in 21 patients (8 with panic disorder, 13 with agoraphobia and panic attacks) and reported that 67% exhibited positional or spontaneous nystagmus, 56% exhibited abnormal calorics, 35% exhibited abnormalities on rotational testing and 32% exhibited abnormal results on posturography. In a subsequent study Jacob and colleagues (Jacob et al. 1989) studied several vestibular tests in 8 patients with panic disorder and reported that 6 (75%) had abnormal results on computerized dynamic posturography, 4 (50%) had unilateral caloric weakness, and 2 (25%) showed directional preponderance on rotational testing. Sklare and colleagues (Sklare et al. 1990) studied 17 patients diagnosed with panic disorder (with and without agoraphobia) and reported that 71% exhibited abnormalities on electronystagmography, though other studies did not find such abnormalities (Swinson et al. 1993). Some of the vestibular studies in patients with panic disorder we find surprising and difficult to interpret. For example, it does not seem plausible that purely psychological factors could cause significant caloric asymmetry; common causes of unilateral vestibular weakness (such as vestibular neuritis) should probably be entertained, irrespective of any psychiatric diagnoses.
In any case, the various vestibular test result abnormalities found in patients with anxiety and panic disorder (with and without agoraphobia) are neither sensitive nor specific to these conditions, and in our view such findings should prompt consideration of primary otovestibular disorders.
Differential diagnosis
Psychological dizziness as we have defined it here is different from diagnoses such as phobic postural vertigo (Brandt 1996; Brandt et al. 1994), space and motion discomfort (Jacob et al. 1993), visually-induced dizziness (Steenerson et al. 2022), chronic subjective dizziness (Staab 2012) and persistent postural perceptual dizziness (Staab et al. 2017).
Although the otoneurologist and neuro-otologist are tasked with diagnosing and managing disequilibrium, in psychological disequilibrium there may also be a diagnosable psychiatric condition that merits management.
Dieterich and colleagues offer the following list of, “Psychiatric disorders that may cause of contribute to vestibular symptoms, ranked by likelihood of doing so” (Dieterich et al. 2016):
- Anxiety and phobic disorders.
- Traumatic stress and obsessive-compulsive disorders (via associated panic attacks and chronic anxiety).
- Depressive disorders.
- Somatic symptom disorder/bodily distress disorder.
- Dissociative disorders (including depersonalization/derealization syndromes).
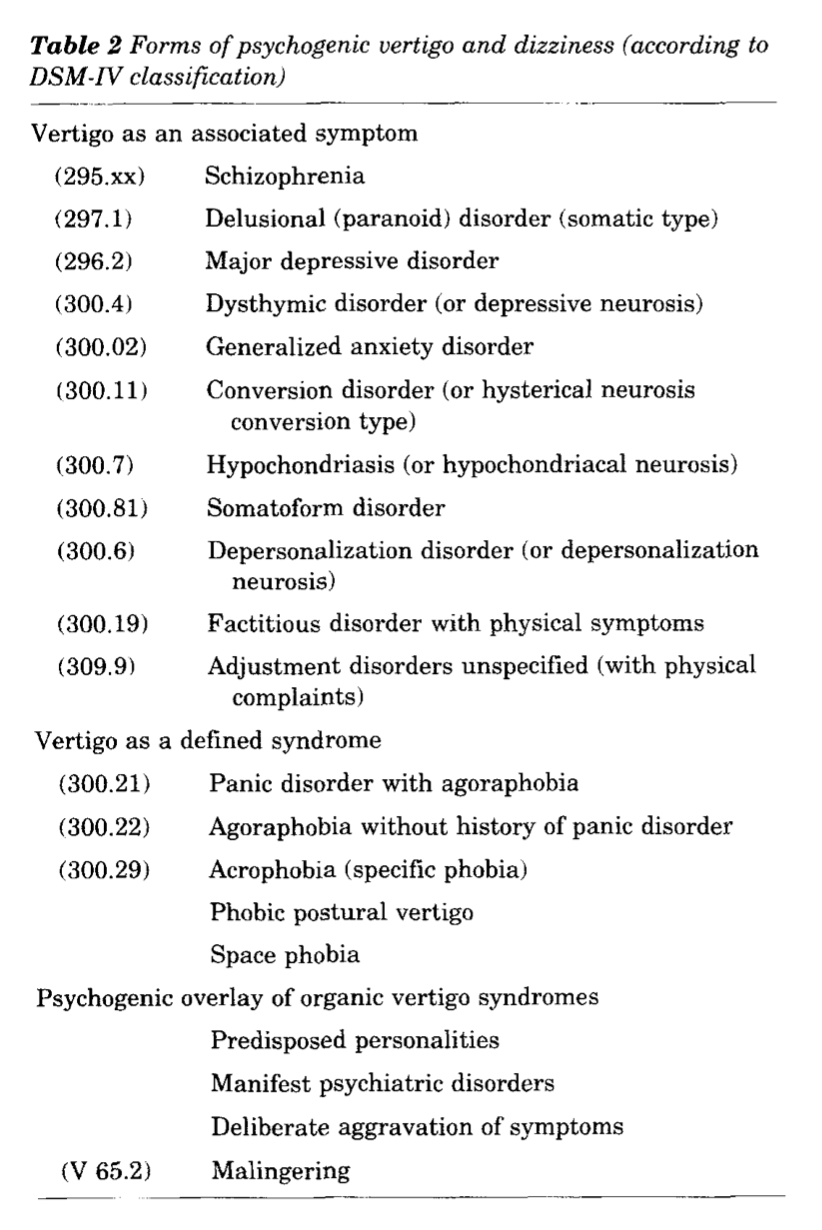
In the Table below, Brandt (Brandt 1996) provides a more detailed, though unprioritized list of psychiatric diagnoses in association with which symptoms of disequilibrium (“vertigo and dizziness”) can occur.
Treatment
It is generally reasonable to consider psychiatric consultation. The rationale for this comes from the potential for mutual reinforcement that psychological symptoms and symptoms of disequilibrium can have on each other. As Jacob and Furman (Jacob and Furman 2001) comment:
“We have seen that psychological factors can exacerbate vestibular symptoms, and that vestibular dysfunction may result in anxiety. In fact, it is likely that vestibular symptoms and anxiety are mutually enhancing, leading to chronicity of both the vestibular and psychiatric symptoms” (Jacob and Furman 2001).
Thus, whether psychological factors are the exclusive cause of the symptom of disequilibrium, or psychological responses occur during the disequilibrium or following the disequilibrium, psychiatric consultation may help to “break” the maladaptive positive feedback loop (“vicious cycle”) of mutually amplifying symptoms.
In our experience the main barrier to this intervention is patients’ reluctance to view any component of their symptoms as “psychological.” We find this regrettable as many patients probably miss an opportunity for improvement.
Prognosis
Prognosis depends on the success of psychological and/or psychiatric intervention.
References
Ardic FN, Atesci FC (2006) Is psychogenic dizziness the exact diagnosis? Eur Arch Otorhinolaryngol 263: 578-81. doi: 10.1007/s00405-006-0013-2
Brandt T (1996) Phobic postural vertigo. Neurology 46: 1515-9. doi: 10.1212/wnl.46.6.1515
Brandt T, Huppert D, Dieterich M (1994) Phobic postural vertigo: a first follow-up. J Neurol 241: 191-5. doi: 10.1007/BF00863767
Cherchi M, Yacovino DA (2021) Dysfunction along the continuum of vestibulocochlear anatomy, and the corresponding spectrum of clinical presentation: how little we know, and what else we need to learn. Hearing, Balance and Communication: 1-12. doi: 10.1080/21695717.2021.1975984
Clark MR, Sullivan MD, Fischl M, Katon WJ, Russo JE, Dobie RA, Voorhees R (1994) Symptoms as a clue to otologic and psychiatric diagnosis in patients with dizziness. J Psychosom Res 38: 461-70. doi: 10.1016/0022-3999(94)90107-4
D’Amour S, Harris LR, Berti S, Keshavarz B (2021) The role of cognitive factors and personality traits in the perception of illusory self-motion (vection). Atten Percept Psychophys 83: 1804-1817. doi: 10.3758/s13414-020-02228-3
Dieterich M, Staab JP, Brandt T (2016) Functional (psychogenic) dizziness. Handb Clin Neurol 139: 447-468. doi: 10.1016/B978-0-12-801772-2.00037-0
Ellis AW, Klaus MP, Mast FW (2017) Vestibular cognition: the effect of prior belief on vestibular perceptual decision making. J Neurol 264: 74-80. doi: 10.1007/s00415-017-8471-6
Ferre ER, Haggard P (2020) Vestibular cognition: State-of-the-art and future directions. Cogn Neuropsychol 37: 413-420. doi: 10.1080/02643294.2020.1736018
Ferre ER, Harris LR (2015) Introduction to Vestibular Cognition Special Issue: Progress in Vestibular Cognition. Multisens Res 28: 393-6. doi: 10.1163/22134808-00002508
Francis BA, Wonham WM (1976) The internal model principle of control theory. Automatica 12: 457-465. doi: 10.1016/0005-1098(76)90006-6
Freud S (1964 (1895)) On the grounds for detaching a particular syndrome from neurasthenia under the description ‘anxiety neurosis’. The standard edition of the complete psychological works of Sigmund Freud, vol 3. Hogarth Press, London
Furman JM, Jacob RG (1997) Psychiatric dizziness. Neurology 48: 1161-6. doi: 10.1212/wnl.48.5.1161
Furman JM, Jacob RG (2001) A clinical taxonomy of dizziness and anxiety in the otoneurological setting. J Anxiety Disord 15: 9-26. doi: 10.1016/s0887-6185(00)00040-2
Hoffman DL, O’Leary DP, Munjack DJ (1994) Autorotation test abnormalities of the horizontal and vertical vestibulo-ocular reflexes in panic disorder. Otolaryngol Head Neck Surg 110: 259-69. doi: 10.1177/019459989411000302
Jacob RG, Furman JM (2001) Psychiatric consequences of vestibular dysfunction. Curr Opin Neurol 14: 41-6. doi: 10.1097/00019052-200102000-00007
Jacob RG, Furman JM, Durrant JD, Turner SM (1996) Panic, agoraphobia, and vestibular dysfunction. Am J Psychiatry 153: 503-12. doi: 10.1176/ajp.153.4.503
Jacob RG, Furman JM, Durrant JD, Turner SM (1997) Surface dependence: a balance control strategy in panic disorder with agoraphobia. Psychosom Med 59: 323-30. doi: 10.1097/00006842-199705000-00016
Jacob RG, Lilienfeld SO, Furman JMR, Durrant JD, Turner SM (1989) Panic disorder with vestibular dysfunction: Further clinical observations and description of space and motion phobic stimuli. Journal of Anxiety Disorders 3: 117-130. doi: https://doi.org/10.1016/0887-6185(89)90006-6
Jacob RG, Moller MB, Turner SM, Wall C, 3rd (1985) Otoneurological examination in panic disorder and agoraphobia with panic attacks: a pilot study. Am J Psychiatry 142: 715-20. doi: 10.1176/ajp.142.6.715
Jacob RG, Redfern MS, Furman JM (1995) Optic flow-induced sway in anxiety disorders associated with space and motion discomfort. Journal of Anxiety Disorders 9: 411-425.
Jacob RG, Woody SR, Clark DB, Lilienfeld SO, Hirsch BE, Kucera GD, Furman JM, Durrant JD (1993) Discomfort with space and motion: A possible marker of vestibular dysfunction assessed by the situational characteristics questionnaire. Journal of Psychopathology and Behavioral Assessment 15: 299-324. doi: 10.1007/BF00965035
Mast FW, Ellis AW (2015) Internal Models, Vestibular Cognition, and Mental Imagery: Conceptual Considerations. Multisens Res 28: 443-60. doi: 10.1163/22134808-00002503
Mertz S, Belkhenchir S, Lepecq JC (2000) Evidence of imagined passive self-motion through imagery-perception interaction. Acta Psychol (Amst) 105: 57-78. doi: 10.1016/s0001-6918(00)00048-2
Nigmatullina Y, Arshad Q, Wu K, Seemungal BM, Bronstein AM, Soto D (2015) How imagery changes self-motion perception. Neuroscience 291: 46-52. doi: 10.1016/j.neuroscience.2015.01.021
Peterka RJ (2018) Sensory integration for human balance control. Handb Clin Neurol 159: 27-42. doi: 10.1016/B978-0-444-63916-5.00002-1
Redfern MS, Furman JM, Jacob RG (2007) Visually induced postural sway in anxiety disorders. J Anxiety Disord 21: 704-16. doi: 10.1016/j.janxdis.2006.09.002
Reuten AJC, Smeets JBJ, Martens MH, Bos JE (2022) Self-motion perception without sensory motion. Exp Brain Res 240: 2677-2685. doi: 10.1007/s00221-022-06442-3
Riecke BE (2009) Cognitive and higher-level contributions to illusory self-motion perception ("vection") : Does the possibility of actual motion affect vection?(Spatio-temporal integration of multimodal sensations,Symposium 2 at the 27th Annual Meeting). The Japanese Journal of Psychonomic Science 28: 135-139. doi: 10.14947/psychono.KJ00005878681
Sklare DA, Stein MB, Pikus AM, Uhde TW (1990) Dysequilibrium and audiovestibular function in panic disorder: symptom profiles and test findings. Am J Otol 11: 338-41.
Staab JP (2012) Chronic subjective dizziness. Continuum (Minneap Minn) 18: 1118-41. doi: 10.1212/01.CON.0000421622.56525.58
Staab JP, Eckhardt-Henn A, Horii A, Jacob R, Strupp M, Brandt T, Bronstein A (2017) Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): Consensus document of the committee for the Classification of Vestibular Disorders of the Barany Society. J Vestib Res 27: 191-208. doi: 10.3233/VES-170622
Staab JP, Ruckenstein MJ (2003) Which comes first? Psychogenic dizziness versus otogenic anxiety. Laryngoscope 113: 1714-8. doi: 10.1097/00005537-200310000-00010
Steenerson KK, Hoskin J, Fife TD (2022) Visually induced dizziness. Curr Opin Neurol 35: 113-117. doi: 10.1097/WCO.0000000000001022
Swinson RP, Cox BJ, Rutka J, Mai M, Kerr S, Kuch K (1993) Otoneurological functioning in panic disorder patients with prominent dizziness. Compr Psychiatry 34: 127-9. doi: 10.1016/0010-440x(93)90057-b
Wertheim AH, Mesland BS, Bles W (2001) Cognitive suppression of tilt sensations during linear horizontal self-motion in the dark. Perception 30: 733-41. doi: 10.1068/p3092
Wolpert DM, Ghahramani Z, Jordan MI (1995) An internal model for sensorimotor integration. Science 269: 1880-2. doi: 10.1126/science.7569931
![]()