By Marcello Cherchi, MD PhD
For patients
In a patient who has disequilibrium and no other symptoms, it is unusual for the cause of disequilibrium to be found in the spinal cord. In the rare instances where there is suspicion for this, your doctor may consider checking an imaging study (such as an MRI of the spine) and several blood tests. The management will depend on what disease the workup reveals.
For clinicians
Overview
Somatosensory input and motor output are crucial in maintaining an upright posture and locomotion. When spinal cord damage involves afferent tracts (somatosensory input) and efferent tracts (motor output), it is unsurprising that a patient will experience disequilibrium.
That being said, it is uncommon for a patient exclusively affected by a spinal cord problem to present to an otoneurology practice. There are probably several reasons for this. First, many of the acute pathologies are so severe (e.g., spinal cord section from penetrating injury) that symptoms other than disequilibrium dominate the clinical picture, and such patients are usually under the acute care of other subspecialties (e.g., neurosurgery). Second, the more chronic diseases (e.g., infection, vitamin deficiency) are usually detected and treated by a general neurologist.
Generally, there are two circumstances in which a patient (ultimately found to have exclusively a spinal cord problem) is referred to an otoneurologist.
The first circumstance is when a patient has already been diagnosed with a spinal cord problem. Usually, the practitioners who arrived at the diagnosis are perfectly aware that a spinal cord problem can interfere with a person’s equilibrium, and in this circumstance, referral to otoneurology is usually motivated by the question, “Is there anything else going on besides the already known spinal cord problem that could interfere with this patient’s balance?” In this situation, doing screening testing for otovestibular disease (vestibular evoked myogenic potentials, video head impulse testing, videonystagmography, rotatory chair testing) is reasonable, since having a spinal cord problem does not preclude a patient’s getting more common causes of disequilibrium (such as vestibular neuritis).
The second circumstance, which is rare, is when an undiagnosed patient with disequilibrium presents to an otoneurologist and has no detectable pathology above the foramen magnum. In this circumstance, it is reasonable to keep a spinal cord disorder on the differential diagnosis. In some cases physical examination (e.g., dissociated hemisensory loss below a cord level) or history (e.g., radiation portal for cancer includes the spinal cord) may narrow the differential diagnosis significantly. In other cases these are still insufficient, and a reasonable workup may include:
- MRI without and with contrast of the entire spinal column. This is to catch disease such as a syrinx, demyelination (multiple sclerosis), tumor (spinal column meningioma, intramedullary tumor), compression (e.g., intervertebral disc, aneurysm), and so forth.
- Serological workup as appropriate, which may include tests for neurosyphilis (RPR, FTA), vitamin B12, copper, HTLV1, HIV, poliovirus and West Nile virus.
Introduction
In a patient whose sole complaint is disequilibrium, it is unusual for the etiology to be an exclusively spinal cord problem.
For purposes of the discussion below, we exclude cervicogenic vertigo, which is addressed elsewhere.
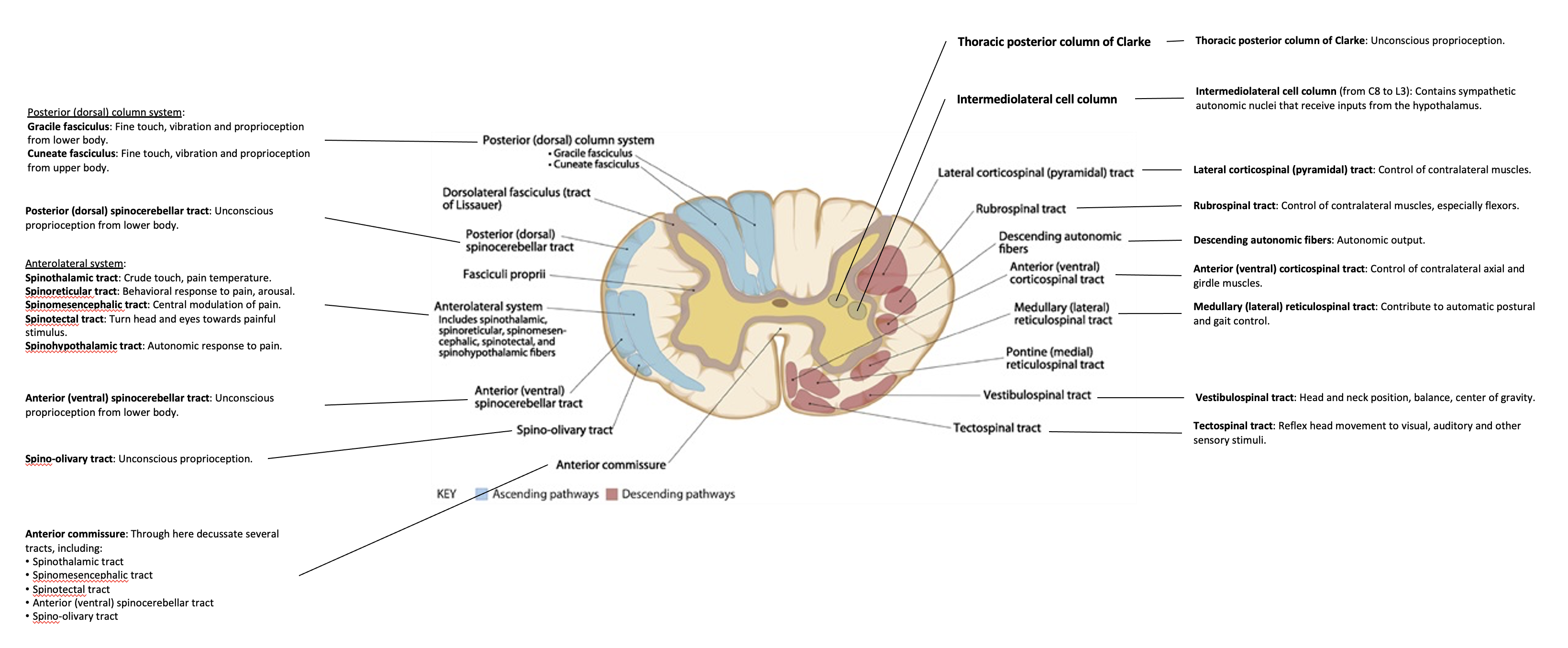
Anatomy
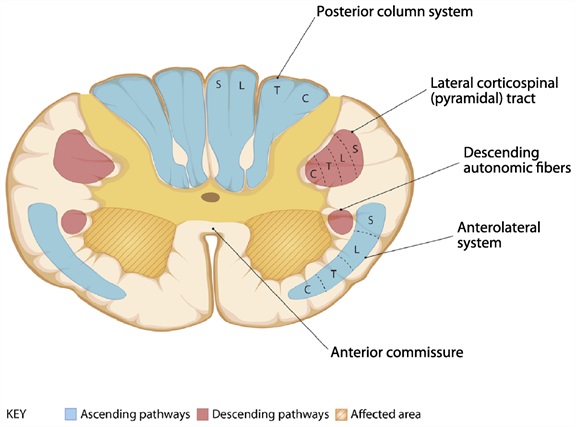
The Figure below, adapted from Cho (Cho 2015), reviews general spinal cord anatomy.
Pathophysiology
Although any part of the spinal cord can be damaged, there are some general patterns that may be helpful in diagnosis. We review these here.
The Figure below, adapted from Cho (Cho 2015), reviews deficits and etiologies of hemicord syndrome.
 |
Hemicord (Brown-Sequard) syndrome:
Etiologies:
|
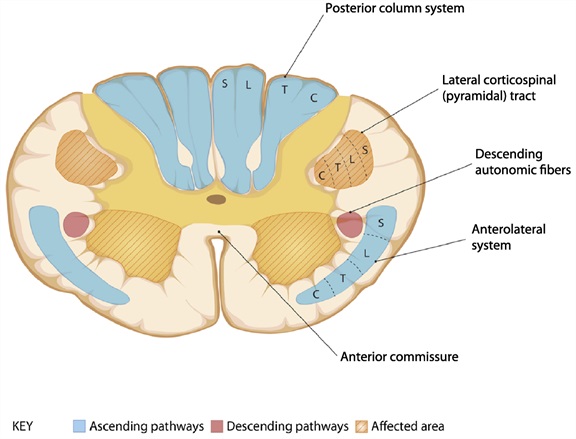
The Figure below, adapted from Cho (Cho 2015), reviews deficits and etiologies of central cord syndrome.
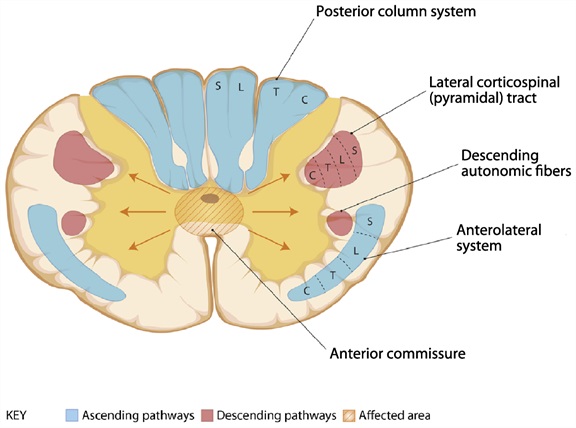 |
Central cord syndrome, small lesion:
Central cord syndrome, large lesion:
Etiologies:
|
The Figure below, adapted from Cho (Cho 2015), reviews deficits and etiologies of posterior column syndrome.
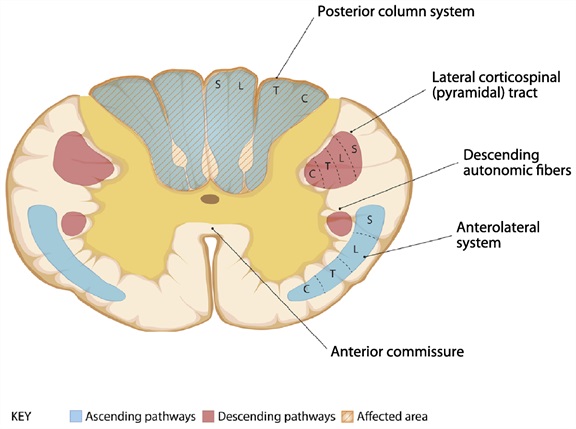 |
Posterior column syndrome:
Etiologies:
|
The Figure below, adapted from Cho (Cho 2015), reviews deficits and etiologies of posteriorlateral cord syndrome.
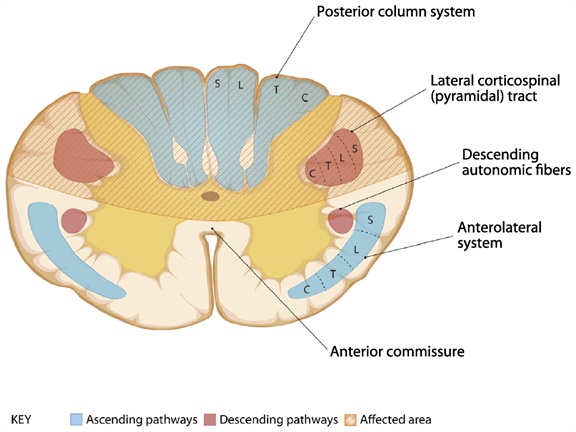 |
Posterolateral column syndrome:
Etiologies:
|
The Figure below, adapted from Cho (Cho 2015), reviews deficits and etiologies of anterior horn syndrome.
 |
Anterior horn syndrome:
Etiologies:
|
The Figure below, adapted from Cho (Cho 2015), reviews deficits and etiologies of combined anterior horn and corticospinal tract syndrome.
 |
Combined anterior horn and corticospinal tract syndrome:
Etiologies:
|
The Figure below, adapted from Cho (Cho 2015), reviews deficits and etiologies of anterior cord syndrome.
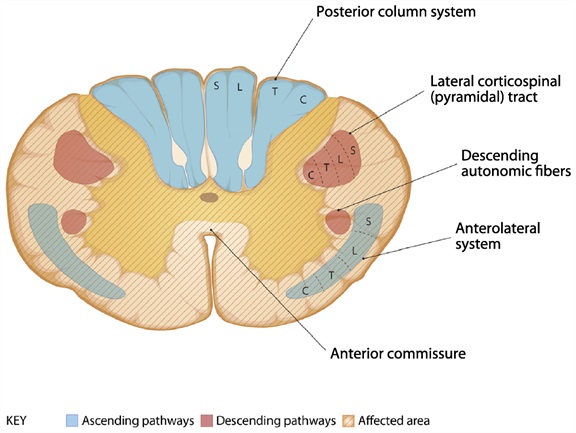 |
Anterior cord syndrome:
Etiologies:
|
References
Cho, T. A. (2015). “Spinal cord functional anatomy.” Continuum (Minneap Minn) 21(1 Spinal Cord Disorders): 13-35.
![]()