By Marcello Cherchi, MD PhD
For patients
Spontaneous down beat nystagmus is an abnormal eye movement that can occur in association with a number of diseases. In some cases patients may notice their eyes jumping (and this symptom is called “oscillopsia”), while in other cases they may not. If your doctor identifies spontaneous down beat nystagmus, they may consider checking several tests of inner ear function and balance function. In some cases treatment is attempted with drugs, but generally the outcome is poor.
For clinicians
Overview
Spontaneous down beat jerk nystagmus (SDBJN) on primary position of gaze nearly always reflects underlying pathology, can occur in a variety of diseases, some of which are reversible, most of which are not. There are several potential mechanisms (discussed below) that can cause SDBJN. The presentation depends on the underlying cause, though in some cases the nystagmus itself can be experienced as oscillopsia. SDBJN is often evident on face-to-face ocular motor examination; in some cases it may be enhanced in amplitude and/or frequency at the extremes of lateral gaze. In some cases the nystagmus is subtle and can be suppressed by visual fixation, but will be discernible on infrared video oculography. Treatment of SDBJN depends on the underlying cause. In cases due to an irreversible lesion the prognosis is poor, but treatment is sometimes attempted with 4‑aminopyridine (dalfampridine) or 3,4‑diaminopyridine.
Introduction
Spontaneous down beat jerk nystagmus (SDBJN) is an abnormal eye movement in which on primary position of gaze, the patient’s eyes slowly drift up, and then snap back down, and the cycle repeats. If this nystagmus is subtle it may be suppressed by visual fixation.
Pathophysiological mechanism of disease
As with many forms of jerk nystagmus, the pathological eye movement is the slow phase (drift), whereas the fast phase (saccade) is a corrective movement for refixation. This means that in spontaneous down beat jerk nystagmus the pathological eye movement is actually the upward drift. There are several mechanisms by which this can occur.
The first mechanism by which spontaneous upward drift of the eyes can occur is by failure of the inferior rectus to contract (leading to unopposed activity of the superior rectus). As Leigh and Rucker explain:
“Excitatory projections for the vertical vestibulo-ocular reflex from the posterior semicircular canals, which mediate downward eye movements, synapse in the medial vestibular nucleus and then cross dorsally in the medulla beneath the nucleus prepositus hypoglossi to reach the contralateral medial longitudinal fasciculus (MLF). Experimental lesions that damage this pathway cause upward eye drifts and downbeat nystagmus” (Leigh and Rucker 2005).
The reason the “experimental lesions” cause this eye movement is that they interfere with this oligoneuronal circuit:
- Afferent signal from posterior semicircular canal sends an excitatory projection that synapses on a neuron in the medial vestibular nucleus.
- The neuron in medial vestibular nucleus sends ascending excitatory projection that decussates, passes through the contralateral medial longitudinal fasciculus, and synapses in the contralateral oculomotor nucleus.
- Neuron in contralateral oculomotor nucleus projects to the inferior rectus muscle, causes contraction, and leads to a slow downward eye movement.
Interruption anywhere along this pathway will result in reduced contraction of the inferior rectus and, given the unopposed normal tonic stimulation of the superior rectus, the eye will drift upward; this will be followed by a downward corrective saccade. As this cycle repeats, it will manifest as spontaneous down beat jerk nystagmus.
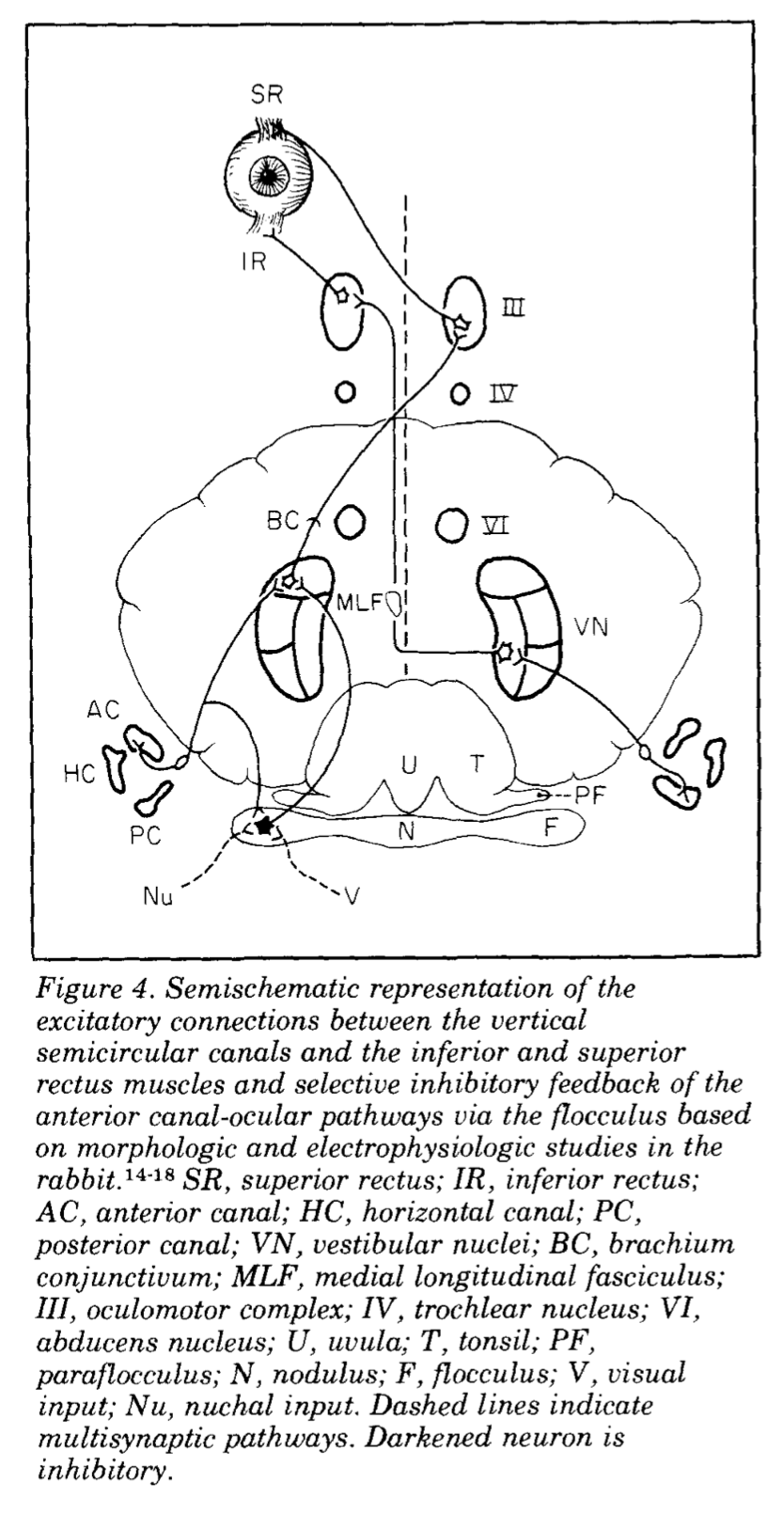
The second mechanism by which spontaneous upward drift of the eyes can occur is by inappropriate contraction of the superior rectus. As Leigh and Rucker explain:
“On the other hand, it appears that excitatory connections from the anterior semicircular canals, which mediate upward eye movements, take different routes; more than one pathway may contribute… The case for the cerebellar flocculus being an important structure in the production of downbeat nystagmus rests on the finding that Purkinje cells send inhibitory projections to the central connections of the anterior semicircular canal but not to the posterior canal. This asymmetry of inhibitory projections accounts for the finding that experimental flocculectomy causes downbeat nystagmus. This lesion disinhibits the projections to the anterior canal but not to the posterior canal, causing the eyes to drift up and producing downbeat nystagmus” (Leigh and Rucker 2005).
The oligoneuronal circuit in question is this:
- Neurons in the superior vestibular nucleus receive several inputs, including:
- An excitatory signal from the ipsilateral anterior semicircular canal.
- An inhibitory signal from the ipsilateral cerebellar flocculus.
- The neuron in the superior vestibular nucleus sends an excitatory projection through the brachium conjunctivum to synapse on a neuron in the contralateral oculomotor nucleus.
- The neuron in the oculomotor nucleus sends a projection that decussates (to the eye ipsilateral to the original anterior semicircular canal) and synapses on the ipsilateral superior rectus, leading to a slow upward eye movement.
A lesion involving the cerebellar flocculus will reduce or eliminate signaling from its inhibitory projection to the ipsilateral superior vestibular nucleus, with the downstream result of excessive contraction of the superior rectus that will overcome the normal tonic opposing contraction of the inferior rectus, and result in slow upward drift of the eyes, which will then be followed by a downward corrective saccade. As this cycle repeats, it will manifest as spontaneous down beat jerk nystagmus.
These two mechanisms are summarized in the Figure below, from Baloh and Spooner (Baloh and Spooner 1981).
The third mechanism by which spontaneous down beat jerk nystagmus can theoretically occur is with lesions that affect the smooth pursuit system. This mechanism was proposed by Zee and colleagues (Zee et al. 1974) based on a control systems analysis.
Clinical presentation
The clinical presentation will depend on the overall disease context. In general, if spontaneous down beat jerk nystagmus is not suppressed by visual fixation, then the patient may experience oscillopsia.
Physical examination
Findings on the general physical and neurological examination will depend on the underlying etiology of the spontaneous down beat jerk nystagmus.
Ocular motor examination
Spontaneous down beat jerk nystagmus may be evident on face-to-face examination. If the nystagmus is mild, then it may be suppressed by visual fixation, and not be evident on face-to-face examination. In some cases the down beat jerk nystagmus may enhanced (in amplitude and/or frequency) at the extremes of lateral gaze. In other cases the down beat jerk nystagmus may not be spontaneous (i.e., not present on primary position of gaze), but may only appear at the extremes of lateral gaze (in which case it is no longer classified as spontaneous).
Testing: vestibular
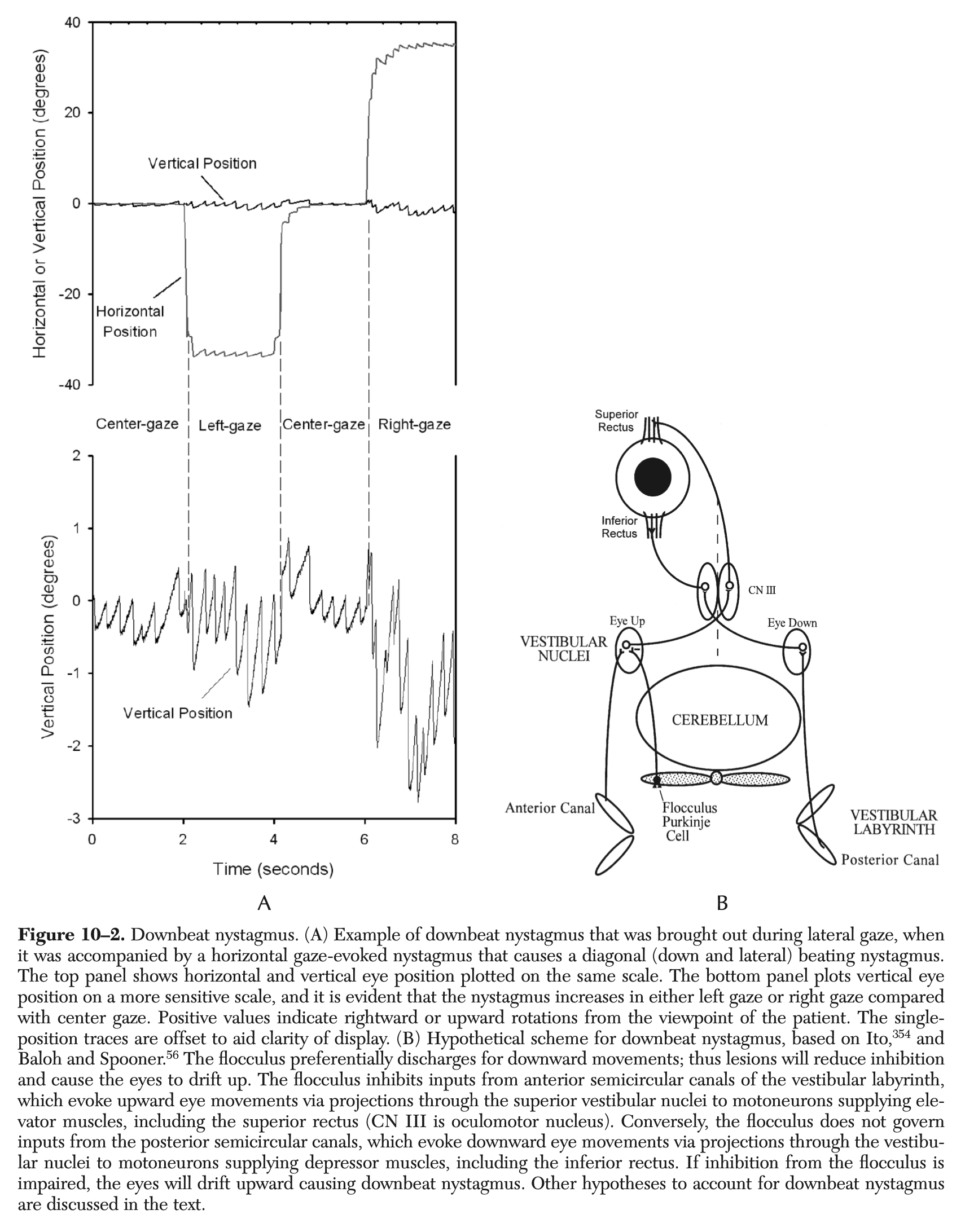
Instrumented oculography, such as infrared videonystagmography, will document spontaneous down beat jerk nystagmus. This nystagmus may augment at the extremes of lateral gaze, as shown in the Figure below from Leigh and Zee (Leigh and Zee 2015).
Differential diagnosis
Spontaneous down beat jerk nystagmus can arise in a variety of disease states. A differential diagnosis of spontaneous down beat jerk nystagmus is listed in the Table below, adapted from Leigh and Zee (Leigh and Zee 2015).
Table: Etiologies of spontaneous down beat jerk nystagmus
- Cerebellar ataxias, including:
- Familial episodic ataxia
- Ataxia telangiectasia
- Celiac disease
- Paraneoplastic degeneration
- Autoimmune states (such as antibodies against glutamic acid decarboxylase)
- Multiple systems atrophy
- Craniocervical anomalies, including:
- Chiari malformation
- Paget’s disease
- Basilar invagination
- Syringobulbia
- Cerebellar infarction
- Brainstem strokes
- Dolichoectasia of the vertebrobasilar artery or compression of the vertebral artery
- Amyotrophic lateral sclerosis
- Multiple sclerosis
- Encephalitis (such as from HTLV1)
- Head trauma
- Heat stroke
- Increased intracranial pressure and hydrocephalus
- Toxic-metabolic etiologies:
- Anticonvulsant medications
- Lithium intoxication
- Acute alcohol intoxication
- Cerebellar degeneration associated with alcohol
- Wernicke’s encephalopathy
- Magnesium depletion
- Amiodarone
- Opioids
- Deficiency of vitamin B12
- Toluene abuse
- Ciguatera-fish poisoning
- Tetanus
- Mitochondrial encephalopathy with lactic acidosis and stroke-like episodes (MELAS)
- Migraine, including vestibular and hemiplegic variants
- Transient manifestation of anterior canal benign paroxysmal positional vertigo
- Transient finding in infants
- Transient finding in children and adults with episodic ataxia type 2
- “Idiopathic” form
Treatment
Treatment of spontaneous down beat jerk nystagmus depends on the underlying etiology. For example, if it is due to medication toxicity, then one may consider discontinuing or reducing the offending medication.
For cases of spontaneous down beat jerk nystagmus resulting from irreversible lesions, treatment options are poor. In cases due to cerebellar lesions, Leigh and Rucker offer the following rationale for pharmacologic intervention:
“The cerebellum inhibits vestibular circuits mediating upward, but not downward, eye movements. Consequently, impaired cerebellar inhibition could cause uninhibited upward drifts of the eyes, which evoke corrective rapid downward movements: downbeat nystagmus. Potassium channels are abundant on cerebellar Purkinje cells—the output neurons from cerebellar cortex—and a related agent, 4‑aminopyridine, is reported to increase the discharge of these neurons by affecting the slowly depolarizing potential. Enhancement of Purkinje cell activity due to 3,4-diaminopyridine could restore to normal levels the inhibitory influence of the cerebellar cortex upon vertical vestibular eye movements. Studies are under way to determine the long-term effects of these drugs on nystagmus and its visual consequences, and to compare 3,4‑diaminopyridine and 4-aminopyridine; the latter penetrates the blood-brain barrier better, has a longer half-life, and is generally better tolerated” (Leigh and Rucker 2005).
The types of studies to which they are alluding include a placebo-controlled study of 3,4‑diaminopyridine (Strupp et al. 2003) and a crossover study of 4‑aminopyridine and 3,4‑diaminopyridine (Polman et al. 1994).
In the United States he drug 4‑aminopyridine, also called dalfampridine, is FDA approved, whereas 3,4‑diaminopyridine is not and must be obtained through compounding pharmacies.
In some cases of spontaneous down beat jerk nystagmus, the nystagmus diminishes or disappears on convergence. In such cases, non-pharmacologic treatment with base-out prism lenses may be helpful (Hertle 2000; Lavin et al. 1983; Parker et al. 2025).
Prognosis
The prognosis of spontaneous down beat jerk nystagmus due to irreversible lesions is poor.
References
Baloh RW, Spooner JW (1981) Downbeat nystagmus: a type of central vestibular nystagmus. Neurology 31: 304-10. doi: 10.1212/wnl.31.3.304
Hertle RW (2000) Examination and refractive management of patients with nystagmus. Surv Ophthalmol 45: 215-22. doi: 10.1016/s0039-6257(00)00153-3
Lavin PJ, Traccis S, Dell’Osso LF, Abel LA, Ellenberger C, Jr. (1983) Downbeat nystagmus with a pseudocycloid waveform: improvement with base-out prisms. Ann Neurol 13: 621-4. doi: 10.1002/ana.410130607
Leigh JR, Rucker JC (2005) Nystagmus and related ocular motility disorders. In: Miller NR, Newman NJ (eds) Walsh & Hoyt’s Clinical Neuro-Ophthalmology, 6th edition edn, vol 1. Lippincott Williams & Wilkins, 530 Walnut Street, Philadelphia, Pennsylvania 19106 USA; 351 West Camden Street, Baltimore, Maryland 21201-2436 USA, pp 1133-1173
Leigh RJ, Zee DS (2015) The neurology of eye movements, 5th edition. edn. Oxford University Press, Oxford ; New York
Parker TM, Jauregui R, Grossman SN, Galetta SL (2025) Downbeat Nystagmus: Case Report, Updated Review, Therapeutics, and Neurorehabilitation. Brain Sci 15. doi: 10.3390/brainsci15080859
Polman CH, Bertelsmann FW, de Waal R, van Diemen HA, Uitdehaag BM, van Loenen AC, Koetsier JC (1994) 4-Aminopyridine is superior to 3,4-diaminopyridine in the treatment of patients with multiple sclerosis. Arch Neurol 51: 1136-9. doi: 10.1001/archneur.1994.00540230074016
Strupp M, Schuler O, Krafczyk S, Jahn K, Schautzer F, Buttner U, Brandt T (2003) Treatment of downbeat nystagmus with 3,4-diaminopyridine: a placebo-controlled study. Neurology 61: 165-70. doi: 10.1212/01.wnl.0000078893.41040.56
Zee DS, Friendlich AR, Robinson DA (1974) The mechanism of downbeat nystagmus. Arch Neurol 30: 227-37. doi: 10.1001/archneur.1974.00490330035006
![]()