By Marcello Cherchi, MD PhD
For clinicians
Overview
Staircase saccades comprise a series of small saccades in a single direction. These have been associated with lesions of the superior colliculi and frontal eye fields, and have also been described in some genetically mediated ataxias (ataxia with oculomotor apraxia types 1 and 2), patients with hemispatial neglect, Parkinson’s disease and Whipple’s disease.
Introduction
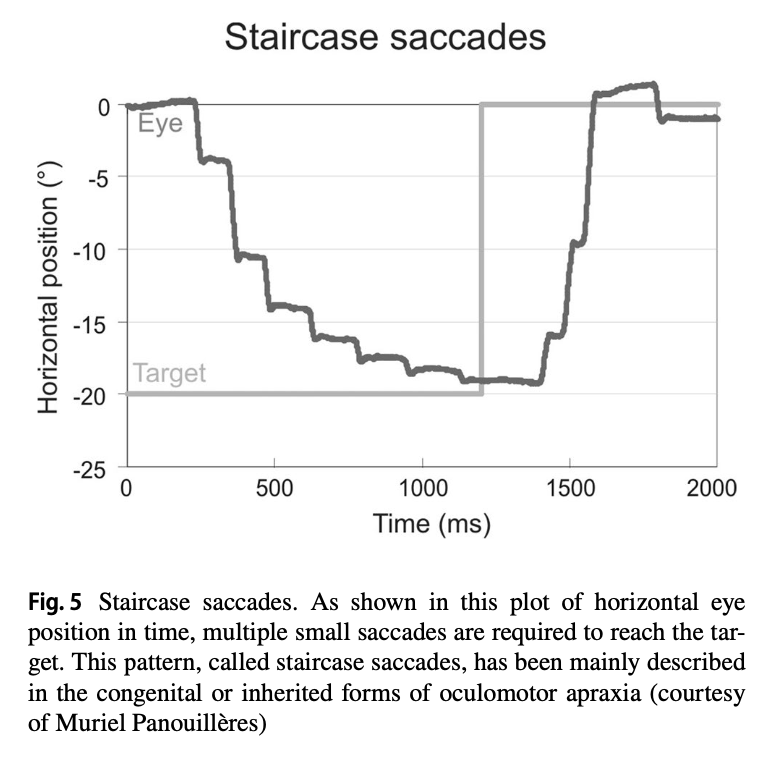
The phrase “staircase saccades” refers to a series of small saccades in a single direction. The phrase describes the appearance of this saccadic pattern on oculographic tracings.
The Figure below, from Tilikete (Froment Tilikete 2022), shows a typical example of staircase saccades on the horizontal tracing of video oculography.
Genetics
Staircase saccades in themselves are not genetically mediated, though there are several genetic ataxias in which staircase saccades occur.
Staircase saccades can be found in ataxia with oculomotor apraxia type 1 (OMIM 208920), an autosomal recessive cerebellar ataxia with hypoalbuminemia resulting from a mutation in the APTX gene on chromosome 9p21.1 which encodes aprataxin (OMIM 606350) (Le Ber et al. 2003).
Staircase saccades can be found in ataxia with oculomotor apraxia type 2 (OMIM 606002), an autosomal recessive spinocerebellar ataxia with axonal neuropathy resulting from a mutation in the SETX gene on chromosome 9q34.13 which encodes senataxin (OMIM 608465) (Panouillères et al. 2013).
Pathophysiological mechanism of disease
Studies in monkeys have shown that staircase saccades can be generated by stimulation in a specific layer of the superior colliculus (Paul and Gnadt 2006; Schiller and Stryker 1972). Studies in monkeys have shown that staircase saccades can be generated by stimulation of the frontal eye field (Robinson and Fuchs 1969), and studies in humans have shown that staircase saccades can result from lesions in the frontal eye fields (Rivaud et al. 1994).
A control systems analysis model proposed by Dell’Osso (Dell’Osso 2019) postulates that the generation of staircase saccades requires two discrete type of dysfunction: (1) transient loss of retinal position information, and (2) a transient change in sampled, reconstructed retinal error. A study in healthy humans emulating these conditions was able to elicit staircase saccades (Rucker et al. 2006). Other proposed models are reviewed by Gancarz and Grossberg (Gancarz and Grossberg 1998).
Ocular motor examination
Staircase saccades are sometimes visible on face-to-face examination.
Testing: vestibular
On tracings of instrumented infrared video oculography, staircase saccades exhibit the appearance described earlier.
Differential diagnosis
Given the pathophysiological mechanisms described earlier, the finding of staircase saccades should raise suspicion for a lesion in the superior colliculi and/or frontal eye fields, though the differential diagnosis is somewhat broader.
- Lesions of the superior colliculi.
- Lesions in the frontal eye fields (Rivaud et al. 1994).
- Shaikh and colleagues (Shaikh et al. 2011) reported staircase saccades in Parkinson’s disease.
- Girotti and colleagues (Girotti et al. 1983) report that in patients with unilateral neglect, saccades in the neglected hemifield either exhibited lengthened reaction time or a staircase saccadic pattern.
- Shaikh and Ghasia (Shaikh and Ghasia 2017) reported staircase saccades in a patient with Whipple’s disease.
- Ataxia with oculomotor apraxia type 1 (Le Ber et al. 2003).
- Ataxia with oculomotor apraxia type 2 (Panouillères et al. 2013).
Treatment and prognosis
There is no known treatment for staircase saccades resulting from static lesions (e.g., strokes or demyelination in the superior colliculi or frontal eye fields) or genetically mediated ataxias. In patients with Parkinson’s disease or Whipple’s disease exhibiting staircase saccades, it is unknown whether treatment for those diseases alters the course of this ocular motor finding.
References
Dell’Osso LF (2019) Ocular Motor System Control Models and the Cerebellum: Hypothetical Mechanisms. Cerebellum 18: 605-614. doi: 10.1007/s12311-018-1001-y
Froment Tilikete C (2022) How to assess eye movements clinically. Neurological Sciences 43: 2969-2981. doi: 10.1007/s10072-022-05981-5
Gancarz G, Grossberg S (1998) A neural model of the saccade generator in the reticular formation. Neural Netw 11: 1159-1174. doi: 10.1016/s0893-6080(98)00096-3
Girotti F, Casazza M, Musicco M, Avanzini G (1983) Oculomotor disorders in cortical lesions in man: the role of unilateral neglect. Neuropsychologia 21: 543-53. doi: 10.1016/0028-3932(83)90010-6
Le Ber I, Moreira MC, Rivaud-Pechoux S, Chamayou C, Ochsner F, Kuntzer T, Tardieu M, Said G, Habert MO, Demarquay G, Tannier C, Beis JM, Brice A, Koenig M, Durr A (2003) Cerebellar ataxia with oculomotor apraxia type 1: clinical and genetic studies. Brain 126: 2761-72. doi: 10.1093/brain/awg283
Panouillères M, Frismand S, Sillan O, Urquizar C, Vighetto A, Pélisson D, Tilikete C (2013) Saccades and eye-head coordination in ataxia with oculomotor apraxia type 2. Cerebellum 12: 557-67. doi: 10.1007/s12311-013-0463-1
Paul K, Gnadt JW (2006) Activity of omnipause neurons during “staircase saccades” elicited by persistent microstimulation of the superior colliculus. Vision Res 46: 3430-42. doi: 10.1016/j.visres.2006.05.014
Rivaud S, Müri RM, Gaymard B, Vermersch AI, Pierrot-Deseilligny C (1994) Eye movement disorders after frontal eye field lesions in humans. Exp Brain Res 102: 110-20. doi: 10.1007/bf00232443
Robinson DA, Fuchs AF (1969) Eye movements evoked by stimulation of frontal eye fields. J Neurophysiol 32: 637-48. doi: 10.1152/jn.1969.32.5.637
Rucker JC, Dell’Osso LF, Garbutt S, Jacobs JB (2006) “Staircase” saccadic intrusions plus transient yoking and neural integrator failure associated with cerebellar hypoplasia: a model simulation. Semin Ophthalmol 21: 229-43. doi: 10.1080/08820530601006767
Schiller PH, Stryker M (1972) Single-unit recording and stimulation in superior colliculus of the alert rhesus monkey. J Neurophysiol 35: 915-24. doi: 10.1152/jn.1972.35.6.915
Shaikh AG, Ghasia FF (2017) Novel Eye Movement Disorders in Whipple’s Disease-Staircase Horizontal Saccades, Gaze-Evoked Nystagmus, and Esotropia. Front Neurol 8: 321. doi: 10.3389/fneur.2017.00321
Shaikh AG, Xu-Wilson M, Grill S, Zee DS (2011) ‘Staircase’ square-wave jerks in early Parkinson’s disease. Br J Ophthalmol 95: 705-9. doi: 10.1136/bjo.2010.179630
![]()