By Marcello Cherchi, MD PhD
For patients
Some cases of tinnitus may be related to a problem in the jaw joint (called the temporomandibular joint). In a patient with tinnitus who also has problems with the mouth and/or jaw — such as poor dentition, bruxism (“grinding” of the teeth), or already diagnosed temporomandibular joint dysfunction — consultation with a dentist or maxillofacial surgeon is reasonable.
For clinicians
Overview
Temporomandibular joint disorder (TMJD)-associated tinnitus can affect any demographic; there may be a slight preponderance of younger women; it seems to have an adverse effect on quality of life. The literature makes clear that the association between TMJD and tinnitus is greater than just overlap by chance, and the few available prospective studies suggest that TMJD may be a risk factor for tinnitus; but these observations do not prove causality. Hypotheses regarding a possible causal relationship remain speculative. Generally TMJD-associated tinnitus tends to be in a higher pitch range. Of the few studies that have sought an anatomical explanation for this problem, attention has focused primarily on the configuration of the petrotympanic fissure, the glenoid fossa, and the temporomandibular joint disc. The most commonly attempted management strategy (and currently the best supported) involves a combination of education, physical therapy and a dental appliance (such as a splint or other jaw-repositioning orthotic).
Medical professionals are generally poorly educated about this problem. Practically, in a patient with tinnitus who additionally has oral problems (poor dentition, bruxism, diagnosed temporomandibular joint dysfunction), referral to a dentist or maxillofacial surgeon is reasonable.
Introduction
The relationship between temporomandibular joint dysfunction (TMJD) and tinnitus is controversial. Note that the abbreviation “TMJ” is sometimes used in the literature to refer to the “temporomandibular joint” or to “temporomandibular joint disorder,” whereas TMD generally refers to the latter. To disambiguate the first abbreviation, in this discussion we use the unconventional abbreviation “TMJD” to refer to “temporomandibular joint disorder/dysfunction.”
The association between TMJD and tinnitus
There is substantial literature demonstrating a greater-than-chance association between TMJD and tinnitus.
- A study reported that the, “Prevalence of tinnitus was found to be 8 times higher in participants with TMD (30 of 82 [36.6%]) than in participants without TMD (38 of 869 [4.4%])” (Buergers et al. 2014).
- A study of 200 tinnitus patients with concomitant temporomandibular joint dysfunction reported that “The severity of tinnitus was significantly associated with the severity of chronic pain,” and that “The most prevalent TMD [temporomandibular] subgroups in tinnitus patients… were myofascial pain with limited opening (39.0%), disc displacement with reduction (44.33%), and arthralgia (53.54%)” (Saldanha et al. 2012).
- A study comparing 30 patients (13 females, 17 males, age 18 – 71 years) suffering from TMJD and tinnitus with control subjects reported that, “Increased odds ratios were found for tenderness of the masticatory muscles… TMJ tenderness to dorsal cranial compression,” concluded that, “A relationship between tinnitus and TMD was established… Tinnitus patients seem to suffer especially from myofascial and TMJ pain,” and recommended that, “A screening for TMD should be included in the diagnostic survey for tinnitus patients” (Bernhardt et al. 2004).
- A meta-analysis reported that, “For TMD, a bidirectional association with tinnitus was found; odds ratios ranged from 2.3 (95%CI [1.5, 3.6]) for arthrogenous TMD to 6.7 (95%CI [2.4, 18.8]) for unspecified TMD” (Bousema et al. 2018).
- A study of 325 patients with TMJD found that 33 (11.5%) had tinnitus (Cebi 2020).
- A survey of 1032 patients (338 with TMJD and 694 age-matched controls) reported that, “Tinnitus [was] significantly more prevalent in the TMD group than in… the control group” (Chole and Parker 1992).
- A study of 79 tinnitus patients observed “higher THI [tinnitus handicap inventory scores] was observed in TMD-pain individuals, compared to TMD-free” individuals (Cimino et al. 2022).
- A study of 2482 tinnitus patients (486 with TMJD, 1996 without TMJD), observed that, “The prevalence of TMJ complaints was greater in tinnitus subjects with severe tinnitus (36%) when compared to those with any tinnitus (19%), strongly indicating the contribution of TMJ problems to the severity of tinnitus” (Edvall et al. 2019).
- A study of 100 patients with tinnitus and 100 subjects without tinnitus reported that, “TMD signs and symptoms were detected in 85% of patients with tinnitus and in 55% of controls,” and concluded that, “Tinnitus is associated with TMD” (Hilgenberg et al. 2012).
- A study of 11745 participants with TMJD and dental pain found that, “The prevalence of tinnitus was higher in the subjects with dental pain (21.1%), TMD (22.5%) and both symptoms (31.2%) than subjects without those symptoms (19.6%)” (Kim et al. 2018).
- A systematic literature review concluded that there is a higher prevalence of tinnitus in patients with TMJD than without (Manfredini 2019).
- A study of 250 patients with TMJD found a tinnitus prevalence of 30.4% (Manfredini et al. 2015).
- A study of 108 patients with TMJD reported that 33 (30.6%) were experiencing tinnitus (Mijiritsky et al. 2020).
- A study of 20 tinnitus patients reported that, “19 of these individuals had one or more clinical, electromyographic, and radiographic indications of a temporomandibular disorder” (Morgan 1992).
- A systematic literature review concluded that, “In all of the selected studies, the prevalence of tinnitus was higher in patients with TMDs (35.8% to 60.7%) than in patients without TMDs (9.7% to 26.0%). The odds ratio of suffering from tinnitus among patients with TMDs was 4.45 (95% CI 1.64-12.11. P = 0.003)” (Mottaghi et al. 2019).
- A meta-analysis of data extracted from 8 papers found that, “In all of the selected studies, the prevalence of tinnitus was higher in patients with TMDs (35.8% to 60.7%) than in patients without TMDs (9.7% to 26.0%). The odds ratio of suffering from tinnitus among patients with TMDs was 4.45 (95% CI 1.64-12.11. P = 0.003)” (Omidvar and Jafari 2019).
- A controlled study of TMJD patients concluded that tinnitus was, “significantly more prevalent in the TMD group than in [the] control group” (Parker and Chole 1995).
- A systematic literature review of tinnitus and TMJD comorbidity concluded that, “The prevalence of tinnitus in patients with TMD varied from 3.7% to 70% (median 42.3%) whereas the prevalence in control groups without TMD varied between 1.7% and 26% (median 12%)” (Skog et al. 2019).
- Data from a study of a mixed population of tinnitus patients (some with TMJD, some without it) was, “retrospectively surveyed to determine which traits or attributes of tinnitus could indicate the possibility of temporomandibular joint dysfunction (TMD) as the cause of tinnitus,” and found that, “No single benchmark standard was discovered that exclusively indicated tinnitus from TMJ origins. However, a total of 10 “TMJ Indicators” were discovered” (Vernon, Griest, Press 1992).
- One study, “compared 30 patients with a confirmed diagnosis of temporomandibular joint dysfunction and tinnitus to a group of 61 patients with tinnitus but without any subjective complaints of TMJ dysfunction with respect to clinical and demographic characteristics,” and concluded that, “Classical risk factors for tinnitus (age, male gender, hearing loss) are less relevant in tinnitus patients with TMJ disorder, suggesting a causal role of TMJ pathology in the generation and maintenance of tinnitus” (Vielsmeier et al. 2011). A subsequent study by Vielsmeier and colleagues reached similar conclusions (Vielsmeier et al. 2012).
A minority of studies failed to identify any relationship between TMJD and tinnitus. For example, Bush (Bush 1987) found no correlation between the two. Demirkol and colleagues (Demirkol, Demirkol et al. 2018) observed that, “gender did show a weak correlation with tinnitus intensity,” but TMJD itself did not. Upton and colleagues studied 989 TMJD patients and found the prevalence of tinnitus to be 7.28%, which was less than estimates of tinnitus of the general population at 10% – 14% (Upton and Wijeyesakere 2004).
Some authors are careful to articulate that the associative relationship does not prove causality. A study of 224 patients (age 18 – 76 years) concluded that, “Painful temporomandibular disorders, high levels of depression, and self reported tinnitus are deeply associated,” noting, “However, this association does not imply a causal relationship” (Fernandes, Goncalves et al. 2013).
Is TMJD a risk factor for developing tinnitus?
Even if the association between TMJD and tinnitus has not been proven as causal, might TMJD be a risk factor for developing tinnitus? A few prospective studies suggest that this may be.
- A prospective study of 191 patients who on examination had pain on palpation of the TMJ and no tinnitus reported that within 5 years, 142 subjects (5.8%) were diagnosed with tinnitus, and concluded that the presence of TMJD was associated with a risk ratio (adjusted for gender, age, school education and frequent headache) of 2.4 (95% confidence interval: 1.6 – 3.7) of developing tinnitus (Bernhardt et al. 2011).
- A study of health insurance claims in Taiwan reported that, “The crude hazard ratio (HR) of tinnitus in the TMJ disorder cohort was 2.73-fold higher than that in the control patients, with an adjusted HR of 2.62 (95 % CI = 2.29-3.00),” and further that, “We also observed a 3.22-fold significantly higher relative risk of developing tinnitus within the 3-year follow-up period (95 % CI = 2.67-3.89). Patients with TMJ disorder might be at increased risk of tinnitus” (Lee et al. 2016).
Imaging studies on TMJD patients with tinnitus
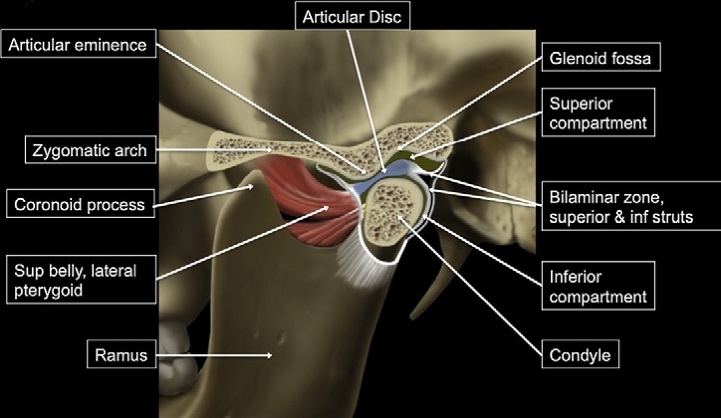
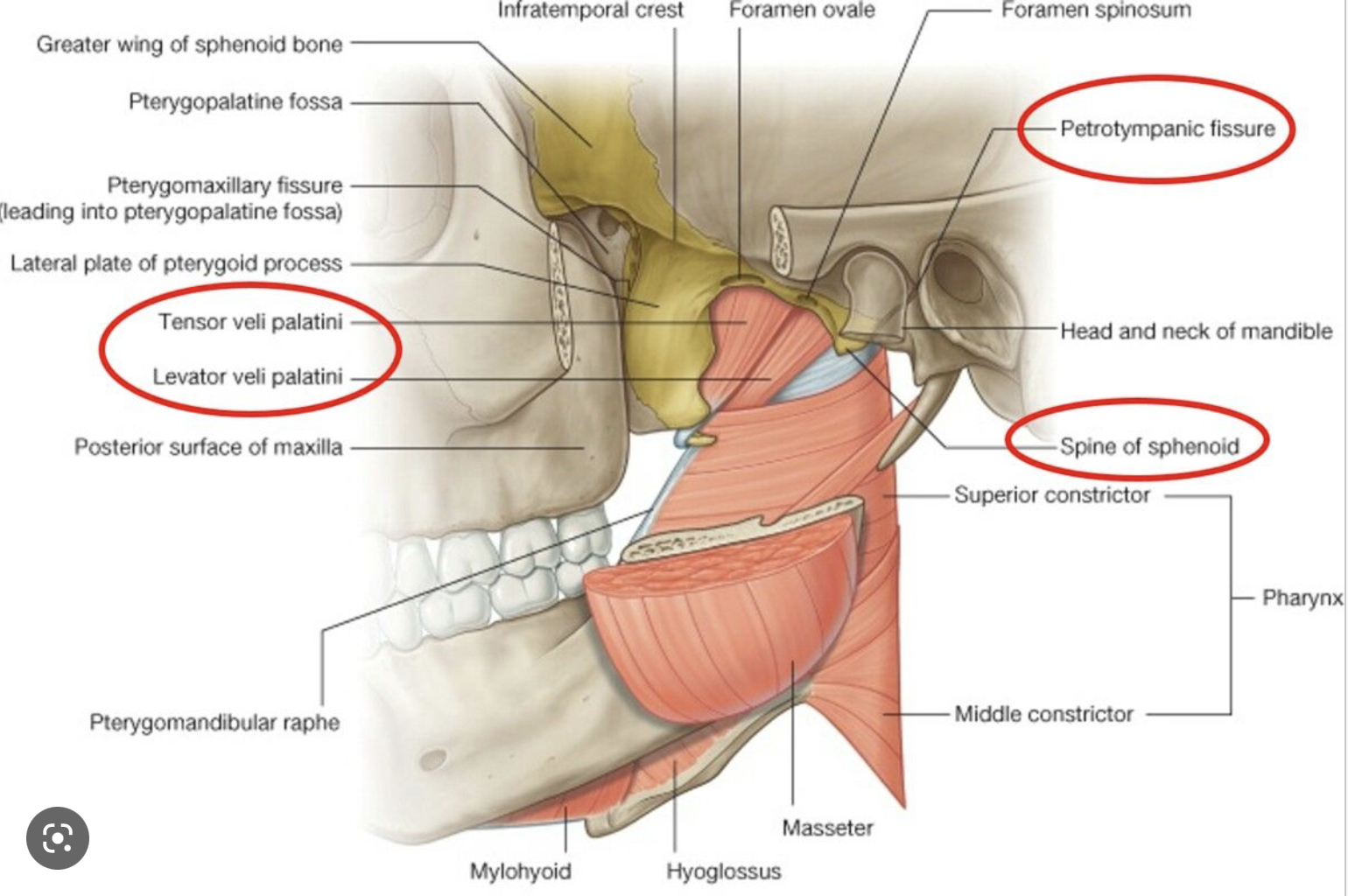
Of the many studies that demonstrate an association between TMJD and tinnitus, very few report on imaging findings that might suggest a structural explanation for the association, but below are several such studies. These focus primarily on the configuration of the petrotympanic fissure, the glenoid fossa, and the temporomandibular joint disc.
The anatomical structures in question are identified in the figures below.
 |
 |
- A cone beam computed tomography study of 100 patients with TMJD (50 with tinnitus, 50 without tinnitus) reported that, “a short, wide petrotympanic fissure (type 1 [wide tubular formation]) might be associated with an increased incidence of tinnitus in patients with TMD” (Cakur and Yasa 2016).
- An imaging study of 331 patients with TMJD and tinnitus found that 33 of the patients (nearly 10%) at petrotympanic fissure configurations, “characterized by a rear (36.59%) or intracranial-cranial (63.41%) condylar displacement of the temporomandibular joint” (Kijak, Szczepek, Margielewicz 2020).
- A study of 82 patients with TMJD (42 patients with tinnitus, 40 patients without tinnitus) found that on CT, “decreased glenoid fossa depth may be associated with an increased incidence of tinnitus” (Koparal et al. 2022).
- An MRI study of 53 patients with TMJD (30 with tinnitus, 23 without tinnitus) reported a higher frequency of disc displacement with reduction in the patients with tinnitus than without tinnitus (Lavinsky et al. 2020).
- An imaging study of 53 patients with unilateral tinnitus and disk displacement, and 82 individuals with disk displacement but no tinnitus found that, “Disk displacement was found to be present in the ipsilateral joint in all 53 patients with unilateral tinnitus, while the contralateral joint was asymptomatic in 50 (94.3%) of them,” and concluded that, “The results of this study revealed a significant correlation between internal derangement of the TMJ and tinnitus” (Ren and Isberg 1995).
TMJ herniation
A few studies, primarily case reports or case series, describe much more dramatic anatomical abnormalities. In these cases, the tinnitus is usually related to mastication with a very disordered temporomandibular joint, typically with herniation.
- A patient with mastication-induced unilateral tinnitus underwent CT which showed that, “the posteromedial bony wall of the glenoid was partially dehiscent” (Choi et al. 2020).
- A patient with tinnitus was reported to have ipsilateral spontaneous herniation of the temporomandibular joint into the external auditory canal (Ertugrul 2018).
- Two patients with clicking tinnitus were found to have temporomandibular joint herniation through the foramen of Huschke (Lim et al. 2019).
Does tinnitus in TMJD have particular characteristics?
There are very few studies characterizing TMJD-associated tinnitus (such as with tinnitus matching). The few studies that do comment that the tinnitus tends to be in a higher frequency range (6 – 9 kHz).
- A study of 20 tinnitus patients (10 with TMJD and 10 without TMJD) observed that in the patients with TMJD the tinnitus, “matched to a 6000 Hz tone or noise,” and these patients, “associated their tinnitus with a single sound,” and concluded that, “tinnitus may occur in patients with TMD, and be of high frequency” (Kanji and Khoza-Shangase 2013).
- A study of 20 adults with tinnitus and normal hearing reported that, “the average tinnitus pitch reported by the subjects was 8.6 kHz and the average loudness was 14.1 dBSL,” and that “90% of patients had at least one sign or symptom of TMD” (Morais and Gil 2012).
What is the mechanism of TMJD-related tinnitus?
Even if one embraces the conjecture of a causal relationship between TMJD and tinnitus, this still leaves open the question of the mechanism connecting the two. Literature on this point remains speculative.
Salvinelli and colleagues speculate that, “Conceivably, TMJD could irritate auricolo-temporal nerve (ATN), triggering a somatosensory pathway-induced disinhibition of dorsal cochlear nucleus (DCN) activity in the auditory pathway. In genetically-predisposed TMJD patients, signals from cronically stimulated DCNs activating specific cortical neuronal networks, could yield plastic neural changes resulting in tinnitus. Based on current evidence of serotoninergic modulation of neural activity and plasticity in sensory pathways, reduced serotoninergic tone could promote plastic changes underlying tinnitus through diminished filtering of incoming signals” (Salvinelli, Casale et al. 2003).
Demographics
Tinnitus related to TMJD can occur at any age, though some literature reports a slight preponderance among younger women.
A study of 200 tinnitus patients reported that tinnitus related to temporomandibular joint dysfunction “principally affects a younger population (average fifth decade of life) and mainly women (more than 2/3 of the cases)” (Algieri, Leonardi et al. 2017).
Response to treatment
A variety of strategies have been attempted to treat TMJD-related tinnitus. Evidence regarding treatment outcomes is weak. A systemic review and meta-analysis reported that, “The eight treatment studies indicated that treatment of TMD symptoms may have a beneficial effect on severity of tinnitus. However, only one treatment study included a control group, meaning that the overall level of evidence is low” (Skog, Fjellner et al. 2019).
Probably the most common strategy is some combination of a dental appliance such as a splint, physical therapy and education.
- A study of 55 tinnitus patients aged 18 – 60 years who had temporomandibular joint dysfunction were evaluated (by the tinnitus handicap inventory and a visual analog scale of temporomandibular joint dysfunction) before and after treatment for TMD with a splint. The authors observed that, “The characteristics of tinnitus and the degree of response to treatment confirmed the relationship between tinnitus and TMD,” and concluded that, “when the most common causes of tinnitus, such as otologic disorders and neurological diseases are excluded, it is correct to evaluate the functionality of the temporo-mandibular joint and eventually treat its pathology to obtain tinnitus improvement or even resolution” (Attanasio et al. 2015).
- A study of 25 patients with tinnitus and ipsilateral TMJD reported symptomatic improvement with “stomatognathic therapy” (oral splints, physiotherapy) in 11 of 25 patients (44%) (Buergers et al. 2014).
- A study of, “Sixty-one patients with tinnitus attributed to TMD were randomized into the physiotherapy and manual therapy group or physiotherapy alone group,” concluded that, “application of cervico-mandibular manual therapies in combination with exercise and education resulted in better outcomes than application of exercise/education alone in individuals with tinnitus attributed to TMD” (Delgado de la Serna et al. 2020).
- A systematic literature review of 11 studies found, “an overall positive effect of the combination of splint therapy and exercise treatment on tinnitus severity and intensity,” though noted that the quality of evidence is low (Michiels et al. 2019).
- A secondary analysis study of 61 subjects with TMJD-related tinnitus treated with “cervico-mandibular manual therapy into an exercise combined with education program” found that, “baseline tinnitus severity and localized PPT over the temporalis muscle were predictive of clinical outcomes in individuals with TMD-related tinnitus following physical therapy” (Plaza-Manzano et al. 2021).
- A study of 80 patients with TMJD pain and tinnitus were divided into two groups, the first of which underwent “orofacial treatment physical therapy complemented with occlusal splints when needed,” and the second of which served as a control group that received no treatment. The authors observed that, “A significant total effect of orofacial treatment compared with control on the change in tinnitus functional index (TFI) score was found,” and concluded that, “Reduction of TMD pain is a mediating factor in the decrease of tinnitus severity after multidisciplinary orofacial treatment” (van der Wal et al. 2022).
- A study of, “Twenty-five patients presenting with a chief complaint of pain around the temporomandibular joints, along with symptoms of internal derangements, i.e., clicking or crepitus, and concomitant vertigo were treated successfully with jaw repositioning orthotics” (Williamson 1990).
- A study of US Air Force patients with TMJD and various otologic symptoms, all of whom were treated with “dental orthotic and TMD self-care instructions,” found that of the patients with tinnitus, 64% reported “at least moderate symptom improvement of their tinnitus” after “3 months of orthotic wear” (Wright, Syms, Bifano 2000).
Less common strategies include injection of anesthetic or steroids, or use of “low level laser therapy.”
- An observational study reported that, “In treating patients with temporomandibular joint (TMJ) dysfunction it was noticed that tinnitus and vertigo were common in such patients and there was also muscular tension in jaw and neck. During treatment of these patients it was also noted that injection of lidocaine in a jaw muscle (m. pt. lat.) reduced not only their muscular problems but also that the tinnitus was reduced while the local anesthetic was active” (Bjorne 2007).
- A study of 70 patients with tinnitus that had “persisted for one month or longer were treated with an intra-articular injection of the temporomandibular joint with steroids,” and the investigators reported that, “Relief of tinnitus at seven-week follow-up was achieved in 20% of the patients treated with temporomandibular steroids. At 18 months, 50% of the patients successfully treated with temporomandibular steroids for tinnitus still experienced a benefit” (Henk and Mark 2019).
- A prospective study of 46 patients with “bilateral subjective tinnitus with TMDs” were randomly allocated into three groups, one treated with “Low-level laser therapy (LLLT) with an neodymium-doped yttrium aluminum garnet (Nd:YAG) (1064 nm) laser,” a second group treated with “LLLT with a diode laser (810 nm),” and a third group that received placebo treatment,” observed that, “There were statistically significant differences in the Nd:YAG laser (p = 0.001) and 810 nm diode laser groups (p = 0.005), but no difference in the placebo group (p = 0.065),” and concluded that, “Both the Nd:YAG and 810 nm diode lasers were effective for the treatment of subjective tinnitus related to TMDs” (Demirkol et al. 2017).
More invasive approaches include a variety of surgical techniques.
- A retrospective study of 43 patients who underwent arthroscopic surgery for arthrogenous TMJD reported that symptoms (including tinnitus), “resolved within 24 hours of arthroscopic temporomandibular joint surgery indicating that the temporomandibular joint pathology was the perpetuating force behind, if not the cause of, these symptoms resolved within 24 hours of arthroscopic temporomandibular joint surgery indicating that the temporomandibular joint pathology was the perpetuating force behind, if not the cause of, these symptoms” (Steigerwald, Verne, Young 1996).
- A study compared 120 patients with tinnitus and TMJD who underwent treatment to patients on a waiting list (who received no treatment). The study found that, “Eighty percent of the patients had signs of TMD, most commonly myofascial pain. Forty-three percent of the patients reported that their tinnitus was improved at the 2-year follow-up, 39% that it was unchanged, and 17% that it was impaired compared to before the treatment,” whereas, “Twelve percent of the subjects in the control group reported that their tinnitus was improved compared to 2 years previously, 32% that it was unchanged, and 56% that it was impaired. The difference between groups was significant (chi(2): p<0.001),” and concluded that, “The results of this study showed that TMD symptoms and signs are frequent in patients with tinnitus and that TMD treatment has a good effect on tinnitus in a long-term perspective, especially in patients with fluctuating tinnitus.”
Quality of life studies
Most, though not all, studies of TMJD-associated tinnitus report that patients suffering with this combination of problems have a lower quality of life.
- A population-based survey of 5786 subjects reported that, “the odds ratio (OR) for lower quality of life was significantly higher in the group with both TMD and tinnitus compared to the group without TMD and tinnitus” (Kong et al. 2022).
- A quality-of-life study of TMJD patients with tinnitus reported pain (from TMJD) to impair quality of life more than tinnitus (Calderon Pdos et al. 2012).
- A quality of life study of 19 patients with TMJD and tinnitus found that, “Tinnitus reported in patients with TMD caused moderate impact on quality of life and can be seen in the presence of background noise although daily activities can still be performed” (Lacerda et al. 2016).
- A quality-of-life study of 100 patients with, “somatosensory tinnitus” including 85 with TMJD and 15 without TMJD found that, “Subjects with somatosensory tinnitus… do not have a higher quality of life handicap” (Hilgenberg-Sydney et al. 2020).
Miscellaneous
A study of 15 patients with painful TMJD without tinnitus, 27 patients with painful TMJD and with tinnitus, and 13 control subjects, identified “dysregulated psychophysiologic interactions” (as measured by several autonomic function tests) in the group of patients with painful TMD and tinnitus compared to the other groups (Kang and Song 2019).
A case report (Hidaka, Tatewaki et al. 2016) of a 41-year-old man with, “objective tinnitus complicated with transient low-tone hearing loss coinciding with mouth opening,” observed that with the jaw open, audiometry “showed elevations [in hearing thresholds] of approximately 20 dB in the frequencies below 1000 Hz,” and “peak pressure on the tympanogram deviated negatively to ‑200 mm H2O,” which they attributed to the radiographic finding that, “CT showed a connection between the mandibular fossa and middle ear space, as revealed by a gas collection around the joint capsule evaluated in two phases (with and without mouth closing).” The investigators performed a myringotomy and reported that the “ear symptoms resolved.” In other words, in this case, jaw opening altered the morphology of the middle ear space, creating negative middle ear pressure resulting in hearing loss and tinnitus.
A study of 310 normal-hearing tinnitus patients with a history of TMJD and/or neck dysfunction and/or a “positive modulation of tinnitus,” found a, “strong association between history and modulation for the same regions within the same patients; such an association should always be investigated to improve chances of a correct diagnosis of somatosensory tinnitus” (Ralli, Altissimi et al. 2016).
A study of 226 patients with tinnitus that could be modulated by “somatic maneuvers” concluded that, “Our findings in patients with chronic tinnitus and normal hearing suggest that self-reported history for somatic dysfunction and modulation of tinnitus, when occurring simultaneously in the TMJ region, can be useful to preliminarily identify patients with TMJ disorders” (Ralli, Greco et al. 2018).
Based on results from the previous studies, Ralli and colleagues hypothesize that, “In some individuals, tinnitus can be modulated by specific maneuvers of the temporomandibular joint, head and neck, eyes, and limbs. Neuroplasticity seems to play a central role in this capacity for modulation, suggesting that abnormal interactions between the sensory modalities, sensorimotor systems, and neurocognitive and neuroemotional networks may contribute to the development of somatosensory tinnitus” (Ralli, Greco et al. 2017).
Medical professionals are often unaware of a relationship between TMJD and tinnitus
Despite the literature support for evidence of an association between TMJD and tinnitus, many medical practitioners are unaware of this.
- A survey of 54 dental surgeons concluded that, “There is a need to inform dentists about the interrelationship between temporomandibular joint disorders and tinnitus” (Martins et al. 2016).
- A survey of 37 primary health care dentists “indicated insufficient knowledge… on the interrelationship between temporomandibular dysfunction and tinnitus” (Martins et al. 2019).
References
Algieri GMA, Leonardi A, Arangio P, Vellone V, Paolo CD, Cascone P (2017) Tinnitus in Temporomandibular Joint Disorders: Is it a Specific Somatosensory Tinnitus Subtype? Int Tinnitus J 20: 83-87. doi: 10.5935/0946-5448.20160016
Attanasio G, Leonardi A, Arangio P, Minni A, Covelli E, Pucci R, Russo FY, De Seta E, Di Paolo C, Cascone P (2015) Tinnitus in patients with temporo-mandibular joint disorder: Proposal for a new treatment protocol. J Craniomaxillofac Surg 43: 724-7. doi: 10.1016/j.jcms.2015.02.009
Bernhardt O, Gesch D, Schwahn C, Bitter K, Mundt T, Mack F, Kocher T, Meyer G, Hensel E, John U (2004) Signs of temporomandibular disorders in tinnitus patients and in a population-based group of volunteers: results of the Study of Health in Pomerania. J Oral Rehabil 31: 311-9. doi: 10.1046/j.1365-2842.2003.01249.x
Bernhardt O, Mundt T, Welk A, Koppl N, Kocher T, Meyer G, Schwahn C (2011) Signs and symptoms of temporomandibular disorders and the incidence of tinnitus. J Oral Rehabil 38: 891-901. doi: 10.1111/j.1365-2842.2011.02224.x
Bjorne A (2007) Assessment of temporomandibular and cervical spine disorders in tinnitus patients. Prog Brain Res 166: 215-9. doi: 10.1016/S0079-6123(07)66019-1
Bousema EJ, Koops EA, van Dijk P, Dijkstra PU (2018) Association Between Subjective Tinnitus and Cervical Spine or Temporomandibular Disorders: A Systematic Review. Trends Hear 22: 2331216518800640. doi: 10.1177/2331216518800640
Buergers R, Kleinjung T, Behr M, Vielsmeier V (2014) Is there a link between tinnitus and temporomandibular disorders? J Prosthet Dent 111: 222-7. doi: 10.1016/j.prosdent.2013.10.001
Bush FM (1987) Tinnitus and otalgia in temporomandibular disorders. J Prosthet Dent 58: 495-8. doi: 10.1016/0022-3913(87)90282-4
Cakur B, Yasa Y (2016) Correlation Between Tinnitus and Petrotympanic Fissure Status Among Patients With Temporomandibular Joint Dysfunction. J Oral Maxillofac Surg 74: 47-52. doi: 10.1016/j.joms.2015.07.020
Calderon Pdos S, Hilgenberg PB, Rossetti LM, Laurenti JV, Conti PC (2012) Influence of tinnitus on pain severity and quality of life in patients with temporomandibular disorders. J Appl Oral Sci 20: 170-3. doi: 10.1590/s1678-77572012000200008
Cebi AT (2020) Presence of tinnitus and tinnitus-related hearing loss in temporomandibular disorders. Cranio: 1-5. doi: 10.1080/08869634.2020.1829290
Choi JW, Nahm H, Shin JE, Kim CH (2020) Temporomandibular joint herniation into the middle ear: A rare cause of mastication-induced tinnitus. Radiol Case Rep 15: 125-127. doi: 10.1016/j.radcr.2019.10.032
Chole RA, Parker WS (1992) Tinnitus and vertigo in patients with temporomandibular disorder. Arch Otolaryngol Head Neck Surg 118: 817-21. doi: 10.1001/archotol.1992.01880080039010
Cimino R, Bucci R, Ambrosio A, Carrabba L, Corrado B, Simeon V, Michelotti A (2022) Temporomandibular disorders, neck disability, and oral parafunctions in tinnitus patients: A cross-sectional epidemiological study from Southern Italy. Cranio 40: 485-493. doi: 10.1080/08869634.2020.1781499
Delgado de la Serna P, Plaza-Manzano G, Cleland J, Fernandez-de-Las-Penas C, Martin-Casas P, Diaz-Arribas MJ (2020) Effects of Cervico-Mandibular Manual Therapy in Patients with Temporomandibular Pain Disorders and Associated Somatic Tinnitus: A Randomized Clinical Trial. Pain Med 21: 613-624. doi: 10.1093/pm/pnz278
Demirkol N, Demirkol M, Usumez A, Sari F, Akcaboy C (2018) The potential etiologic factors influencing tinnitus intensity in patients with temporomandibular disorders. Cranio 36: 360-365. doi: 10.1080/08869634.2017.1363344
Demirkol N, Usumez A, Demirkol M, Sari F, Akcaboy C (2017) Efficacy of Low-Level Laser Therapy in Subjective Tinnitus Patients with Temporomandibular Disorders. Photomed Laser Surg 35: 427-431. doi: 10.1089/pho.2016.4240
Edvall NK, Gunan E, Genitsaridi E, Lazar A, Mehraei G, Billing M, Tullberg M, Bulla J, Whitton J, Canlon B, Hall DA, Cederroth CR (2019) Impact of Temporomandibular Joint Complaints on Tinnitus-Related Distress. Front Neurosci 13: 879. doi: 10.3389/fnins.2019.00879
Ertugrul S (2018) Rare Cause of Tinnitus: Spontaneous Temporomandibular Joint Herniation Into the External Auditory Canal. J Craniofac Surg 29: e521-e522. doi: 10.1097/SCS.0000000000004579
Fernandes G, Goncalves DA, de Siqueira JT, Camparis CM (2013) Painful temporomandibular disorders, self reported tinnitus, and depression are highly associated. Arq Neuropsiquiatr 71: 943-7. doi: 10.1590/0004-282X20130191
Henk K, Mark K (2019) Temporomandibular steroids in patients with tinnitus: Only on indication. Int Tinnitus J 23: 10-16. doi: 10.5935/0946-5448.20190003
Hidaka H, Tatewaki Y, Sakamoto M, Kobayashi T, Yuasa Y, Yuasa R, Nomura K, Yamauchi D, Katori Y (2016) Transient Hearing Loss and Objective Tinnitus Induced by Mouth Opening: A Rare Connection Between the Temporomandibular Joint and Middle Ear Space. Otol Neurotol 37: e217-21. doi: 10.1097/MAO.0000000000001078
Hilgenberg PB, Saldanha AD, Cunha CO, Rubo JH, Conti PC (2012) Temporomandibular disorders, otologic symptoms and depression levels in tinnitus patients. J Oral Rehabil 39: 239-44. doi: 10.1111/j.1365-2842.2011.02266.x
Hilgenberg-Sydney PB, Saldanha ADD, Lopes AC, Conti PCR (2020) Audiological Evaluation of Patients With Somatosensory Tinnitus Attributed to Temporomandibular Disorders. Am J Audiol 29: 930-934. doi: 10.1044/2020_AJA-20-00133
Kang JH, Song SI (2019) Autonomic and Psychologic Risk Factors for Development of Tinnitus in Patients with Chronic Temporomandibular Disorders. J Oral Facial Pain Headache 33: 362-370. doi: 10.11607/ofph.2237
Kanji A, Khoza-Shangase K (2013) Clinical signs and symptoms of tinnitus in temporomandibular joint disorders: a pilot study comparing patients and non-patients. S Afr J Commun Disord 60: 16-20.
Kijak E, Szczepek AJ, Margielewicz J (2020) Association between Anatomical Features of Petrotympanic Fissure and Tinnitus in Patients with Temporomandibular Joint Disorder Using CBCT Imaging: An Exploratory Study. Pain Res Manag 2020: 1202751. doi: 10.1155/2020/1202751
Kim YH, Park YG, Han KD, Vu D, Cho KH, Lee SY (2018) Prevalence of tinnitus according to temporomandibular joint disorders and dental pain: The Korean National Population-based Study. J Oral Rehabil 45: 198-203. doi: 10.1111/joor.12604
Kong GS, Lee SH, Park KS, Cho JH, Kim KW, Ha IH (2022) Association of temporomandibular disorders and tinnitus with health-related quality of life: A cross-sectional study using the Fifth Korea National Health and Nutrition Examination Survey. J Oral Rehabil 49: 283-294. doi: 10.1111/joor.13287
Koparal M, Sirik M, Yavuz GY, Ege B (2022) Evaluation of the relationship between temporomandibular joint disorders and tinnitus with computed tomography. J Stomatol Oral Maxillofac Surg 123: e199-e205. doi: 10.1016/j.jormas.2022.06.015
Lacerda AB, Facco C, Zeigelboim BS, Cristoff K, Stechman JN, Fonseca VR (2016) The impact of tinnitus on the quality of life in patients with temporomandibular dysfunction. Int Tinnitus J 20: 24-30. doi: 10.5935/0946-5448.20160005
Lavinsky D, Lavinsky J, Setogutti ET, Rehm DDS, Lavinsky L (2020) The Role of Magnetic Resonance Imaging of the Temporomandibular Joint to Investigate Tinnitus in Adults with Temporomandibular Joint Disorder: A Comparative Study. Int Arch Otorhinolaryngol 24: e68-e72. doi: 10.1055/s-0039-1688840
Lee CF, Lin MC, Lin HT, Lin CL, Wang TC, Kao CH (2016) Increased risk of tinnitus in patients with temporomandibular disorder: a retrospective population-based cohort study. Eur Arch Otorhinolaryngol 273: 203-8. doi: 10.1007/s00405-015-3491-2
Lim KH, Jung JY, Rhee J, Choi J (2019) Temporomandibular joint herniation through the foramen of Huschke with clicking tinnitus. Eur Ann Otorhinolaryngol Head Neck Dis 136: 497-499. doi: 10.1016/j.anorl.2018.05.014
Manfredini D (2019) Tinnitus in Temporomandibular Disorders patients: any clinical implications from research findings? Evid Based Dent 20: 30-31. doi: 10.1038/s41432-019-0012-y
Manfredini D, Olivo M, Ferronato G, Marchese R, Martini A, Guarda-Nardini L (2015) Prevalence of tinnitus in patients with different temporomandibular disorders symptoms. Int Tinnitus J 19: 47-51. doi: 10.5935/0946-5448.20150008
Martins PF, Stechman JN, Marques JM, Martins SK, Cristoff KE, Sampaio RS, Massi G, Hummig W (2016) Tinnitus and temporomandibular disorders: the knowledge of professionals for primary health care in the city of Curitiba. Int Tinnitus J 20: 18-23. doi: 10.5935/0946-5448.20160004
Martins PFA, Stechman-Neto J, Cristoff KE, Ravazzi G, Goncalves FM, Sampaio RS (2019) Temporomandibular dysfunction and tinnitus the knowledge of the dental surgeon in primary health care. Int Tinnitus J 23: 125-132. doi: 10.5935/0946-5448.20190022
Michiels S, Nieste E, Van de Heyning P, Braem M, Visscher C, Topsakal V, Gilles A, Jacquemin L, De Hertogh W (2019) Does Conservative Temporomandibular Therapy Affect Tinnitus Complaints? A Systematic Review. J Oral Facial Pain Headache 33: 308-317. doi: 10.11607/ofph.2055
Mijiritsky E, Winocur E, Emodi-Perlman A, Friedman-Rubin P, Dahar E, Reiter S (2020) Tinnitus in Temporomandibular Disorders: Axis I and Axis II Findings According to the Diagnostic Criteria for Temporomandibular Disorders. J Oral Facial Pain Headache 34: 265-272. doi: 10.11607/ofph.2611
Morais AA, Gil D (2012) Tinnitus in individuals without hearing loss and its relationship with temporomandibular dysfunction. Braz J Otorhinolaryngol 78: 59-65. doi: 10.1590/S1808-86942012000200010
Morgan DH (1992) Tinnitus of TMJ origin: a preliminary report. Cranio 10: 124-9. doi: 10.1080/08869634.1992.11677900
Mottaghi A, Menendez-Diaz I, Cobo JL, Gonzalez-Serrano J, Cobo T (2019) Is there a higher prevalence of tinnitus in patients with temporomandibular disorders? A systematic review and meta-analysis. J Oral Rehabil 46: 76-86. doi: 10.1111/joor.12706
Omidvar S, Jafari Z (2019) Association Between Tinnitus and Temporomandibular Disorders: A Systematic Review and Meta-Analysis. Ann Otol Rhinol Laryngol 128: 662-675. doi: 10.1177/0003489419842577
Parker WS, Chole RA (1995) Tinnitus, vertigo, and temporomandibular disorders. Am J Orthod Dentofacial Orthop 107: 153-8. doi: 10.1016/s0889-5406(95)70130-3
Plaza-Manzano G, Delgado-de-la-Serna P, Diaz-Arribas MJ, Rodrigues-de-Souza DP, Fernandez-de-Las-Penas C, Alburquerque-Sendin F (2021) Influence of Clinical, Physical, Psychological, and Psychophysical Variables on Treatment Outcomes in Somatic Tinnitus Associated With Temporomandibular Pain: Evidence From a Randomized Clinical Trial. Pain Pract 21: 8-17. doi: 10.1111/papr.12919
Ralli M, Altissimi G, Turchetta R, Mazzei F, Salviati M, Cianfrone F, Orlando MP, Testugini V, Cianfrone G (2016) Somatosensory Tinnitus: Correlation between Cranio-Cervico-Mandibular Disorder History and Somatic Modulation. Audiol Neurootol 21: 372-382. doi: 10.1159/000452472
Ralli M, Greco A, Boccassini A, Altissimi G, Di Paolo C, Falasca V, De Virgilio A, Polimeni A, Cianfrone G, de Vincentiis M (2018) Subtyping patients with somatic tinnitus: Modulation of tinnitus and history for somatic dysfunction help identify tinnitus patients with temporomandibular joint disorders. PLoS One 13: e0202050. doi: 10.1371/journal.pone.0202050
Ralli M, Greco A, Turchetta R, Altissimi G, de Vincentiis M, Cianfrone G (2017) Somatosensory tinnitus: Current evidence and future perspectives. J Int Med Res 45: 933-947. doi: 10.1177/0300060517707673
Ren YF, Isberg A (1995) Tinnitus in patients with temporomandibular joint internal derangement. Cranio 13: 75-80. doi: 10.1080/08869634.1995.11678048
Saldanha AD, Hilgenberg PB, Pinto LM, Conti PC (2012) Are temporomandibular disorders and tinnitus associated? Cranio 30: 166-71. doi: 10.1179/crn.2012.026
Salvinelli F, Casale M, Paparo F, Persico AM, Zini C (2003) Subjective tinnitus, temporomandibular joint dysfunction, and serotonin modulation of neural plasticity: causal or casual triad? Med Hypotheses 61: 446-8. doi: 10.1016/s0306-9877(03)00194-4
Skog C, Fjellner J, Ekberg E, Haggman-Henrikson B (2019) Tinnitus as a comorbidity to temporomandibular disorders-A systematic review. J Oral Rehabil 46: 87-99. doi: 10.1111/joor.12710
Steigerwald DP, Verne SV, Young D (1996) A retrospective evaluation of the impact of temporomandibular joint arthroscopy on the symptoms of headache, neck pain, shoulder pain, dizziness, and tinnitus. Cranio 14: 46-54. doi: 10.1080/08869634.1996.11745949
Upton LG, Wijeyesakere SJ (2004) The incidence of tinnitus in people with disorders of the temporomandibular joint. Int Tinnitus J 10: 174-6.
van der Wal A, Michiels S, Van de Heyning P, Gilles A, Jacquemin L, Van Rompaey V, Braem M, Visscher CM, Topsakal V, Truijen S, De Hertogh W (2022) Reduction of Somatic Tinnitus Severity is Mediated by Improvement of Temporomandibular Disorders. Otol Neurotol 43: e309-e315. doi: 10.1097/MAO.0000000000003446
Vernon J, Griest S, Press L (1992) Attributes of tinnitus that may predict temporomandibular joint dysfunction. Cranio 10: 282-7; discussion 287-8. doi: 10.1080/08869634.1992.11677924
Vielsmeier V, Kleinjung T, Strutz J, Burgers R, Kreuzer PM, Langguth B (2011) Tinnitus with temporomandibular joint disorders: a specific entity of tinnitus patients? Otolaryngol Head Neck Surg 145: 748-52. doi: 10.1177/0194599811413376
Vielsmeier V, Strutz J, Kleinjung T, Schecklmann M, Kreuzer PM, Landgrebe M, Langguth B (2012) Temporomandibular joint disorder complaints in tinnitus: further hints for a putative tinnitus subtype. PLoS One 7: e38887. doi: 10.1371/journal.pone.0038887
Williamson EH (1990) Interrelationship of internal derangements of the temporomandibular joint, headache, vertigo, and tinnitus: a survey of 25 patients. Cranio 8: 301-6. doi: 10.1080/08869634.1990.11678328
Wright EF, Syms CA, 3rd, Bifano SL (2000) Tinnitus, dizziness, and nonotologic otalgia improvement through temporomandibular disorder therapy. Mil Med 165: 733-6.
![]()