By Marcello Cherchi, MD PhD
For patients
The eighth cranial nerve (also known as the vestibulo-cochlear nerve) transmits auditory (hearing-related) signals and vestibular (balance-related) signals from the ear to the brain. In some circumstances this nerve can become episodically irritable. The term “vestibular paroxysmia” refers to a condition in which only the vestibular portion of this nerve is involved. The term “vestibulo-cochlear paroxysmia” refers to a condition in which both the vestibular and auditory portions of this nerve are involved. One would think that there should also be a condition corresponding to a situation in which only the cochlear portion of the nerve is involved (“cochlear paroxysmia”); perhaps the closest thing to this is a phenomenon called “typewriter tinnitus.”
Vestibular paroxysmia is the more common of the three conditions. It usually presents with episodes of disequilibrium that are very abrupt in onset (there is no warning), brief (a fraction of a second), and terminates abruptly. The sense of disequilibrium can be in any direction; some patients describe feeling as if they are thrown to the floor (giving rise to the colloquial term, “drop attack”), but it can also manifest as an abrupt spin or shove in any direction. Presumably the specific sensation depends on which part of the vestibular nerve is affected. The frequency of attacks is variable, ranging from dozens per day to a few times per year.
Vestibulo-cochlear paroxysmia is the less common of the three conditions. The vestibular component is similar to that in vestibular paroxysmia, but the episodes are also accompanied by an auditory component — in other words, there is an abrupt-onset, abrupt-offset, and very brief attack of disequilibrium and tinnitus. The tinnitus can present variably, such as a buzzing, humming or ringing.
The least common of the three conditions is cochlear paroxysmia, in the form of “typewriter tinnitus.”
In the majority of cases no clear cause for these diseases can be discerned. Although the original description by neurosurgeon Dr. Peter Jannetta identified cases in which the vestibulo-cochlear nerve was being impinged upon by a blood vessel, subsequent research brought into question whether this mechanism accounted for most, or even any of the cases.
Management of these diseases is symptom-driven. In patients who elect to treat, the management is with small doses of anti-seizure medications — though to be clear, this is not a seizure disorder. When anti-seizure medications are used for treating actual seizure disorders, they are prescribed in relatively high doses because seizures are abnormal electrical activity in large portions of the brain. In contrast, in a condition in which only a single nerve is affected (such as vestibular paroxysmia or vestibulo-cochlear paroxysmia), anti-seizure medications can be used in very small doses.
The anti-seizure medication with which there is the most experience in treatment of vestibular- and vestibulo-cochlear paroxysmia is oxcarbazepine. There is less literature regarding other agents, such as carbamazepine, gabapentin, lacosamide, phenytoin and valproate. There is even modest literature regarding the use of agents other than anti-seizure medications, such as betahistine.
For practitioners
Overview
Vestibular paroxysmia, cochlear paroxysmia and vestibulo-cochlear paroxysmia are conditions in which there appears to be episodic irritability of the vestibular nerve (vestibular paroxysmia), auditory nerve (cochlear paroxysmia) or vestibular and cochlear components of the vestibulo-cochlear nerve (vestibulo-cochlear paroxysmia). The presentation consists of recurrent episodes of abrupt-onset, brief (usually seconds), abrupt-offset, symptoms of disequilibrium (for vestibular paroxysmia), tinnitus (for cochlear paroxysmia) or both (vestibulo-cochlear paroxysmia). The underlying etiology is usually not known. Initial interest in the “vascular cross-compression” theory (the idea that a small artery abuts the vestibulo-cochlear nerve and wears away its myelin or inappropriately stimulates it) faded when it was realized that the presence/absence of such an artery does not correlate well with the presence/absence of symptoms. Ocular motor examination and infrared video oculography are generally normal. Imaging and otovestibular workup are generally unrevealing, though serve to exclude competing diagnoses. First-line medical therapy is oxcarbazepine; other anti-epileptics have been less well-studied. If these fail, if imaging shows vascular cross-compression, and (preferably) if otovestibular testing shows abnormalities ipsilateral to the radiographic vascular cross-compression, then referral for neurosurgical evaluation is reasonable.
Introduction
Vestibular paroxysmia, cochlear paroxysmia and vestibulo-cochlear paroxysmia are conditions in which there appears to be episodic irritability of the vestibular nerve (vestibular paroxysmia), auditory nerve (cochlear paroxysmia) or vestibular and cochlear components of the vestibulo-cochlear nerve (vestibulo-cochlear paroxysmia).
Clinical history
This condition was described by neurosurgeon, Dr. Peter Jannetta (Jannetta 1975, Jannetta, Moller et al. 1984). Symptoms can be vestibular alone (vestibular) or vestibular and auditory (vestibulo-cochlear), and present as episodes with abrupt onset (without prodrome) that are very brief and terminate abruptly. A study of 22 patients (Ihtijarevic, Van Ombergen et al. 2019) listed a mean age of onset of 49 ± 17 years (range 15 – 80 years), with 15 females (69%) and 7 males (31%). The same study listed the following symptoms:
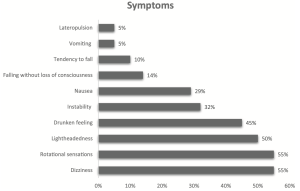
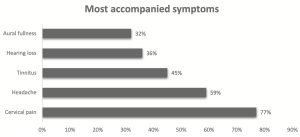
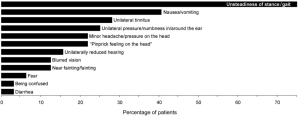
Hufner and colleagues (Hufner, Barresi et al. 2008) reported symptoms as follows:
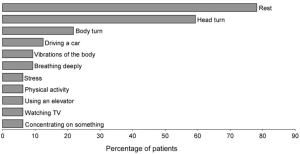
Ihtijarevic and colleagues (Ihtijarevic, Van Ombergen et al. 2019) stated that in 77% of patients the symptoms were triggered by positional changes (in 55% by head movements; in 27% by rolling over in bed); and in 27% the symptoms occurred spontaneously. Hufner and colleagues (Hufner, Barresi et al. 2008) provided a more detailed list of apparent triggers:
Our own clinical experience is that in most patients the episodes occur without any discernible trigger.
Earlier descriptions characterize the episodes as extremely brief, on the order of a fraction of a second. Subsequent studies of larger number of patients listed durations ranging from seconds to minutes (Ihtijarevic, Van Ombergen et al. 2019).
Cochlear paroxysmia manifests as “typewriter tinnitus” (Levine 2006), and probably reflects similarly brief bursts of abnormal signaling.
Etiology
The original descriptions by Dr. Peter Jannetta (Jannetta 1975) attributed vestibular paroxysmia to “vascular cross compression” of the vestibular nerve by a loop of the anterior inferior cerebellar artery, though subsequent literature described vascular cross compression by other blood vessels as well, such as the posterior inferior cerebellar artery, a vertebral artery or a vein (Best, Gawehn et al. 2013), or the superior cerebellar artery (Ryu, Yamamoto et al. 1998). This was thought to be analogous to some cases of trigeminal neuralgia, another condition in which a cranial nerve (the trigeminal nerve) is sometimes found to have vascular impingement (Gronseth, Cruccu et al. 2008).
Although some radiologic literature concluded that there was a correlation between vascular cross compression and audio-vestibular symptoms (McCabe and Harker 1983, Jannetta, Moller et al. 1984, Herzog, Bailey et al. 1997, McDermott, Dutt et al. 2003, Nowe, De Ridder et al. 2004, De Ridder, De Ridder et al. 2005, Shinn, Bush et al. 2009, Wuertenberger and Rosahl 2009, Moosa, Fezeu et al. 2015), other literature found no such correlation (Parnes, Shimotakahara et al. 1990, Reisser and Schuknecht 1991, Makins, Nikolopoulos et al. 1998, van der Steenstraten, de Ru et al. 2007, Gorrie, Warren et al. 2010, Hoekstra, Prijs et al. 2015).
Since some patients whose clinical history is compatible with vestibular paroxysmia have no evidence of vascular impingement, and since some asymptomatic individuals have vascular impingement, this brought into question the hypothesis of a purely vascular etiology of this disease, and in fact, the Barany Society consensus document states, “The role of imaging in the diagnosis and identification of the affected side is not clear because of the high rate of blood vessels close to the 8th cranial nerve in healthy subjects” (Strupp, Lopez-Escamez et al. 2016).
Although there is some logic to the hypothesis of vascular cross compression, there are certainly other neural pathologies that can damage axons and/or Schwann cells (from demyelination, infection, ischemia, and others) that presumably could provoke episodic irritability of the nerve.
Physical examination
Given the sporadic and brief nature of the symptoms, it is difficult for a clinician to examine a patient during an episode, but some investigators have been able to capture this.
- Young and colleagues (Young et al. 2019) observed a patient during an episode of vestibular paroxysmia and described a “flurry” of nystagmus (horizontal and torsional) coterminous with the patient’s symptoms.
- Choi and colleagues (Choi et al. 2018) described a patient with spontaneous baseline horizontal nystagmus that reversed direction during episodes of vestibular paroxysmia.
- Imai and colleagues (Imai et al. 2025) studied 21 patients whose clinical histories were compatible with vestibular paroxysmia, and in whom there was either radiological evidence of neurovascular cross-compression, or there were unilateral cranial nerve symptoms. They gave these patients portable eye movement recording devices, which they used during episodes. The researchers found that 6 patients exhibited nystagmus during episodes of vestibular paroxysmia; in all 6 of these the nystagmus beat toward the presumably affected ear; in 3 (of the 6) patients there was occasionally nystagmus beating toward the unaffected ear; in 1 (of the 6) patients there was sometimes nystagmus that began beating toward the unaffected ear and then shifted to beating toward the affected ear; in 1 (of the 6) patients there was sometimes nystagmus that began beating toward the affected ear and then shifted to beating toward the unaffected ear.
The more common scenario is for a clinician to be examining a patient inter-ictally. In cases that Ihtijarevic and colleagues (Ihtijarevic, Van Ombergen et al. 2019) classify as “definite vestibular paroxysmia,” 50% of patients have “persistent horizontal” nystagmus, 17% have “persistent clockwise/counterclockwise” nystagmus, 8% have “persistent up/downbeating nystagmus,” and 25% exhibit no nystagmus. Our own experience is that patients generally have no nystagmus, or minimal horizontal nystagmus.
Testing
In view of the proposed pathophysiology, one would expect to find detectable abnormalities in audiologic and vestibular testing in patients with vestibular and vestibulo-cochlear paroxysmia. Indeed, a broad variety of audiologic and vestibular tests have been studied in these patients, including audiometry, vestibular evoked myogenic potentials, bedside and video head impulse testing, fundoscopy, static and dynamic subjective visual vertical, caloric testing, video oculography (head-shaking nystagmus, gaze-evoked nystagmus, hyperventilation-induced nystagmus), and brainstem auditory evoked potentials (Hufner, Barresi et al. 2008, Best, Gawehn et al. 2013, Choi, Choi et al. 2018, Young, Jonker et al. 2019), and many report lateralizing abnormalities.
However, it should be borne in mind that patients with clinical histories convincing for vestibular and vestibulo-cochlear paroxysmia can also have normal otovestibular workups (Markowski, Gierek et al. 2011).
Treatment
Jannetta and colleagues reported many patients in whom the symptoms of vestibular paroxysmia were reduced or eliminated by microvascular decompression (Jannetta, Moller et al. 1984, Moller, Moller et al. 1986, Moller 1990, Moller, Moller et al. 1993, Moller 1997), and other neurosurgeons also attempted this technique (Ryu, Yamamoto et al. 1998). However, as discussed earlier, there are patients with clinical histories compatible with vestibular paroxysmia who have no radiographic evidence of vascular cross compression.
Consequently, most practitioners will first attempt medical (pharmacologic) therapy. The drug with which there is the most clinical experience is oxcarbazepine (Hufner, Barresi et al. 2008, Strupp, Dieterich et al. 2016, Bayer, Bremova et al. 2018). There is less experience with carbamazepine (Hufner, Barresi et al. 2008, Strupp, Dieterich et al. 2016), gabapentin (Russell and Baloh 2009, Strupp, Dieterich et al. 2016), valproate (Strupp, Dieterich et al. 2016), phenytoin (Strupp, Dieterich et al. 2016), lacosamide (Strupp, Elger et al. 2019) and betahistine (Xue, Xiang et al. 2018).
In patients who do not respond to reasonable attempts at pharmacologic therapy, who have strong radiographic evidence of vascular impingement on the vestibulocochlear nerve, and (preferably) have objective otovestibular deficits ipsilateral to that vascular impingement, referral to neurosurgery is reasonable.
References
Bayer O, Bremova T, Strupp M, Hufner K (2018) A randomized double-blind, placebo-controlled, cross-over trial (Vestparoxy) of the treatment of vestibular paroxysmia with oxcarbazepine. J Neurol 265: 291-298. doi: 10.1007/s00415-017-8682-x
Best C, Gawehn J, Kramer HH, Thomke F, Ibis T, Muller-Forell W, Dieterich M (2013) MRI and neurophysiology in vestibular paroxysmia: contradiction and correlation. J Neurol Neurosurg Psychiatry 84: 1349-56. doi: 10.1136/jnnp-2013-305513
Choi SY, Choi JH, Choi KD (2018) The nystagmus of vestibular paroxysmia. J Neurol 265: 1711-1713. doi: 10.1007/s00415-018-8920-x
De Ridder D, De Ridder L, Nowe V, Thierens H, Van de Heyning P, Moller A (2005) Pulsatile tinnitus and the intrameatal vascular loop: why do we not hear our carotids? Neurosurgery 57: 1213-7; discussion 1213-7.
Gorrie A, Warren FM, 3rd, de la Garza AN, Shelton C, Wiggins RH, 3rd (2010) Is there a correlation between vascular loops in the cerebellopontine angle and unexplained unilateral hearing loss? Otol Neurotol 31: 48-52. doi: 10.1097/MAO.0b013e3181c0e63a
Gronseth G, Cruccu G, Alksne J, Argoff C, Brainin M, Burchiel K, Nurmikko T, Zakrzewska JM (2008) Practice parameter: the diagnostic evaluation and treatment of trigeminal neuralgia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the European Federation of Neurological Societies. Neurology 71: 1183-90. doi: 10.1212/01.wnl.0000326598.83183.04
Herzog JA, Bailey S, Meyer J (1997) Vascular loops of the internal auditory canal: a diagnostic dilemma. Am J Otol 18: 26-31.
Hoekstra CE, Prijs VF, van Zanten GA (2015) Diagnostic yield of a routine magnetic resonance imaging in tinnitus and clinical relevance of the anterior inferior cerebellar artery loops. Otol Neurotol 36: 359-65. doi: 10.1097/MAO.0000000000000279
Hufner K, Barresi D, Glaser M, Linn J, Adrion C, Mansmann U, Brandt T, Strupp M (2008) Vestibular paroxysmia: diagnostic features and medical treatment. Neurology 71: 1006-14. doi: 10.1212/01.wnl.0000326594.91291.f8
Ihtijarevic B, Van Ombergen A, Celis L, Maes LK, Wuyts FL, Van de Heyning PH, Van Rompaey V (2019) Symptoms and signs in 22 patients with vestibular paroxysmia. Clin Otolaryngol. doi: 10.1111/coa.13356
Imai T, Tanaka A, Kimura N, Nakajima T, Kitahara T, Mikami S (2025) Nystagmus Patterns in Patients with Vestibular Paroxysmia: Insights From Portable Eye Movement Recording. Otol Neurotol 46: 1129-1136. doi: 10.1097/MAO.0000000000004612
Jannetta PJ (1975) Neurovascular cross-compression in patients with hyperactive dysfunction symptoms of the eighth cranial nerve. Surg Forum 26: 467-9.
Jannetta PJ, Moller MB, Moller AR (1984) Disabling positional vertigo. N Engl J Med 310: 1700-5. doi: 10.1056/NEJM198406283102604
Levine RA (2006) Typewriter tinnitus: a carbamazepine-responsive syndrome related to auditory nerve vascular compression. ORL J Otorhinolaryngol Relat Spec 68: 43-6; discussion 46-7. doi: 10.1159/000090490
Makins AE, Nikolopoulos TP, Ludman C, O’Donoghue GM (1998) Is there a correlation between vascular loops and unilateral auditory symptoms? Laryngoscope 108: 1739-42. doi: 10.1097/00005537-199811000-00027
Markowski J, Gierek T, Kluczewska E, Witkowska M (2011) Assessment of vestibulocochlear organ function in patients meeting radiologic criteria of vascular compression syndrome of vestibulocochlear nerve–diagnosis of disabling positional vertigo. Med Sci Monit 17: CR169-73. doi: 10.12659/msm.881452
McCabe BF, Harker LA (1983) Vascular loop as a cause of vertigo. Ann Otol Rhinol Laryngol 92: 542-3. doi: 10.1177/000348948309200602
McDermott AL, Dutt SN, Irving RM, Pahor AL, Chavda SV (2003) Anterior inferior cerebellar artery syndrome: fact or fiction. Clin Otolaryngol Allied Sci 28: 75-80.
Moller MB (1990) Results of microvascular decompression of the eighth nerve as treatment for disabling positional vertigo. Ann Otol Rhinol Laryngol 99: 724-9. doi: 10.1177/000348949009900911
Moller MB (1997) Selection criteria and treatment of patients with disabling positional vertigo. Stereotact Funct Neurosurg 68: 270-3. doi: 10.1159/000099938
Moller MB, Moller AR, Jannetta PJ, Jho HD, Sekhar LN (1993) Microvascular decompression of the eighth nerve in patients with disabling positional vertigo: selection criteria and operative results in 207 patients. Acta Neurochir (Wien) 125: 75-82. doi: 10.1007/BF01401831
Moller MB, Moller AR, Jannetta PJ, Sekhar L (1986) Diagnosis and surgical treatment of disabling positional vertigo. J Neurosurg 64: 21-8. doi: 10.3171/jns.1986.64.1.0021
Moosa S, Fezeu F, Kesser BW, Ramesh A, Sheehan JP (2015) Sudden unilateral hearing loss and vascular loop in the internal auditory canal: case report and review of literature. J Radiosurg SBRT 3: 247-255.
Nowe V, De Ridder D, Van de Heyning PH, Wang XL, Gielen J, Van Goethem J, Ozsarlak O, De Schepper AM, Parizel PM (2004) Does the location of a vascular loop in the cerebellopontine angle explain pulsatile and non-pulsatile tinnitus? Eur Radiol 14: 2282-9. doi: 10.1007/s00330-004-2450-x
Parnes LS, Shimotakahara SG, Pelz D, Lee D, Fox AJ (1990) Vascular relationships of the vestibulocochlear nerve on magnetic resonance imaging. Am J Otol 11: 278-81.
Reisser C, Schuknecht HF (1991) The anterior inferior cerebellar artery in the internal auditory canal. Laryngoscope 101: 761-6. doi: 10.1288/00005537-199107000-00012
Russell D, Baloh RW (2009) Gabapentin responsive audiovestibular paroxysmia. J Neurol Sci 281: 99-100. doi: 10.1016/j.jns.2009.03.018
Ryu H, Yamamoto S, Sugiyama K, Nozue M (1998) Neurovascular compression syndrome of the eighth cranial nerve. What are the most reliable diagnostic signs? Acta Neurochir (Wien) 140: 1279-86.
Shinn JB, Bush ML, Jones RO (2009) Correlation of central auditory processing deficits and vascular loop syndrome. Ear Nose Throat J 88: E34-7.
Strupp M, Dieterich M, Brandt T, Feil K (2016a) Therapy of Vestibular Paroxysmia, Superior Oblique Myokymia, and Ocular Neuromyotonia. Curr Treat Options Neurol 18: 34. doi: 10.1007/s11940-016-0417-2
Strupp M, Elger C, Goldschagg N (2019) Treatment of vestibular paroxysmia with lacosamide. Neurology: Clinical Practice 9: 539-541. doi: 10.1212/cpj.0000000000000610
Strupp M, Lopez-Escamez JA, Kim JS, Straumann D, Jen JC, Carey J, Bisdorff A, Brandt T (2016b) Vestibular paroxysmia: Diagnostic criteria. J Vestib Res 26: 409-415. doi: 10.3233/VES-160589
van der Steenstraten F, de Ru JA, Witkamp TD (2007) Is microvascular compression of the vestibulocochlear nerve a cause of unilateral hearing loss? Ann Otol Rhinol Laryngol 116: 248-52. doi: 10.1177/000348940711600404
Wuertenberger CJ, Rosahl SK (2009) Vertigo and tinnitus caused by vascular compression of the vestibulocochlear nerve, not intracanalicular vestibular schwannoma: review and case presentation. Skull Base 19: 417-24. doi: 10.1055/s-0029-1220209
Xue H, Xiang W, Yu Y, Liu G, Chong Y, Zhou J (2018) Randomized trial of betahistine mesilate tablets as augmentation for oxcarbazepine and carbamazepine in treating vestibular paroxysmia. Drug Des Devel Ther 12: 837-843. doi: 10.2147/DDDT.S158888
Young AS, Jonker B, Welgampola MS (2019) Vestibular paroxysmia presenting with irritative nystagmus. Neurology 92: 723-724. doi: 10.1212/WNL.0000000000007273
![]()