By Marcello Cherchi, MD PhD
For patients
Windmill nystagmus is an acquired abnormal eye movement that usually develops in a person who has significant visual loss in both eyes. The management is treatment (if possible) of the visual loss, so these patients are usually under the care of an ophthalmologist.
For clinicians
Overview
Windmill nystagmus is rare. This is an acquired disorder of ocular motility in which there is spontaneous nystagmus whose direction rotates. Windmill nystagmus usually results from significant bilateral visual loss that has usually been gradually progressive (e.g., macular degeneration, retinitis pigmentosa) though can also be subacute. One case of paraneoplastic windmill nystagmus has been reported in which the patient’s vision was normal and the nystagmus developed over 3 weeks. When windmill nystagmus occurs in the context of visual loss, treatment involves managing the visual loss, and the causes of visual loss usually have a poor prognosis. When windmill nystagmus occurs as a paraneoplastic syndrome, the treatment and prognosis depend on the underlying malignancy.
Introduction
Windmill nystagmus is an abnormal eye movement in which there is spontaneous nystagmus, of which the fast phase direction varies in its horizontal and vertical components, usually in a regular pattern. The vector of the fast phase rotates, and the direction of the rotation (clockwise or counterclockwise) depends on the amplitude and phase relationship between the horizontal and vertical components.
Epidemiology
Windmill nystagmus is rare.
Most described cases have been reported in patients with significant visual limitations. Usually the visual loss is the result of slowly progressive degenerative processes (e.g., retinitis pigmentosa, macular degeneration, etc.) (Choi et al. 2016), though it has also been reported as soon as 3 months after subacute visual loss (Lee et al. 2018a).
Lee and colleagues (Lee et al. 2018b) described windmill nystagmus occurring in paraneoplastic cerebellar degeneration in a patient with small cell lung carcinoma and positive antibodies for anti‑SOX1 and anti‑Hu. In this case the patient complained of unsteadiness that developed over 3 weeks.
Pathophysiological mechanism of disease
The underlying pathophysiological mechanism of windmill nystagmus is unknown. Choi and colleagues emphasize the relevance of low vision:
“The underlying mechanisms [of windmill nystagmus] remain uncertain. An attractive hypothesis is that a malfunction within the visual-motor ‘adaptation’ pathways, and specifically in the mechanisms that normally sense image motion on the retina, leads to the unwanted oscillations. Without such [visual] information, central gaze-holding networks, which are normally finely tuned to the exact ‘gains’ needed to hold gaze stable, become susceptible to the ‘noise’ and drift that is inherent in all neural networks” (Choi et al. 2016).
Choi and colleagues (Choi et al. 2016) comment on the relationship between windmill nystagmus and (horizontal) period alternating nystagmus:
“Windmill nystagmus is characterized by a clock-like rotation of the beating direction. It resembles periodic alternating nystagmus (PAN), which is restricted to the horizontal plane, in that the direction of nystagmus changes in a predictable pattern. In contrast to PAN, however, windmill nystagmus alternates direction in both the horizontal and vertical planes. Thus, windmill nystagmus has been considered a periodic alternating horizontal nystagmus with a superimposed periodic alternating vertical nystagmus, with the periods of the two oscillations being 90 degrees out of phase” (Choi et al. 2016).
They also comment on the relationship between windmill nystagmus and elliptical pendular nystagmus:
“Windmill (jerk) nystagmus is in some respects analogous to circular or elliptical (pendular) nystagmus, though the period of the oscillation of pendular nystagmus is much lower than that of windmill nystagmus. Both represent a summation of simultaneous horizontal and vertical oscillations. The trajectory of the eyes is determined by the amplitude and phase relationships of the horizontal and vertical components. When the two pendular oscillations are either in phase or 180 degrees out of phase, the nystagmus is diagonal. In contrast, the nystagmus is circular when the two components are equal and 90 degrees out of phase, and elliptical when the amplitudes are unequal but still 90 degrees out of phase” (Choi et al. 2016).
Clinical presentation
Most patients present with gradually progressive visual deterioration that has resulted in near blindness.
Physical examination
The most common underlying cause of windmill nystagmus is severe, gradually progressive visual loss, which should be apparent on physical examination.
In the case of windmill nystagmus occurring as a paraneoplastic syndrome (Lee et al. 2018b), the authors reported that the patient was unsteady to the point of being unable to walk unaided.
Ocular motor examination
The Video below, from Lee and colleagues (Lee et al. 2018b), shows windmill nystagmus.
Testing: vestibular
Instrumented oculography is the best way to capture the windmill pattern of nystagmus.
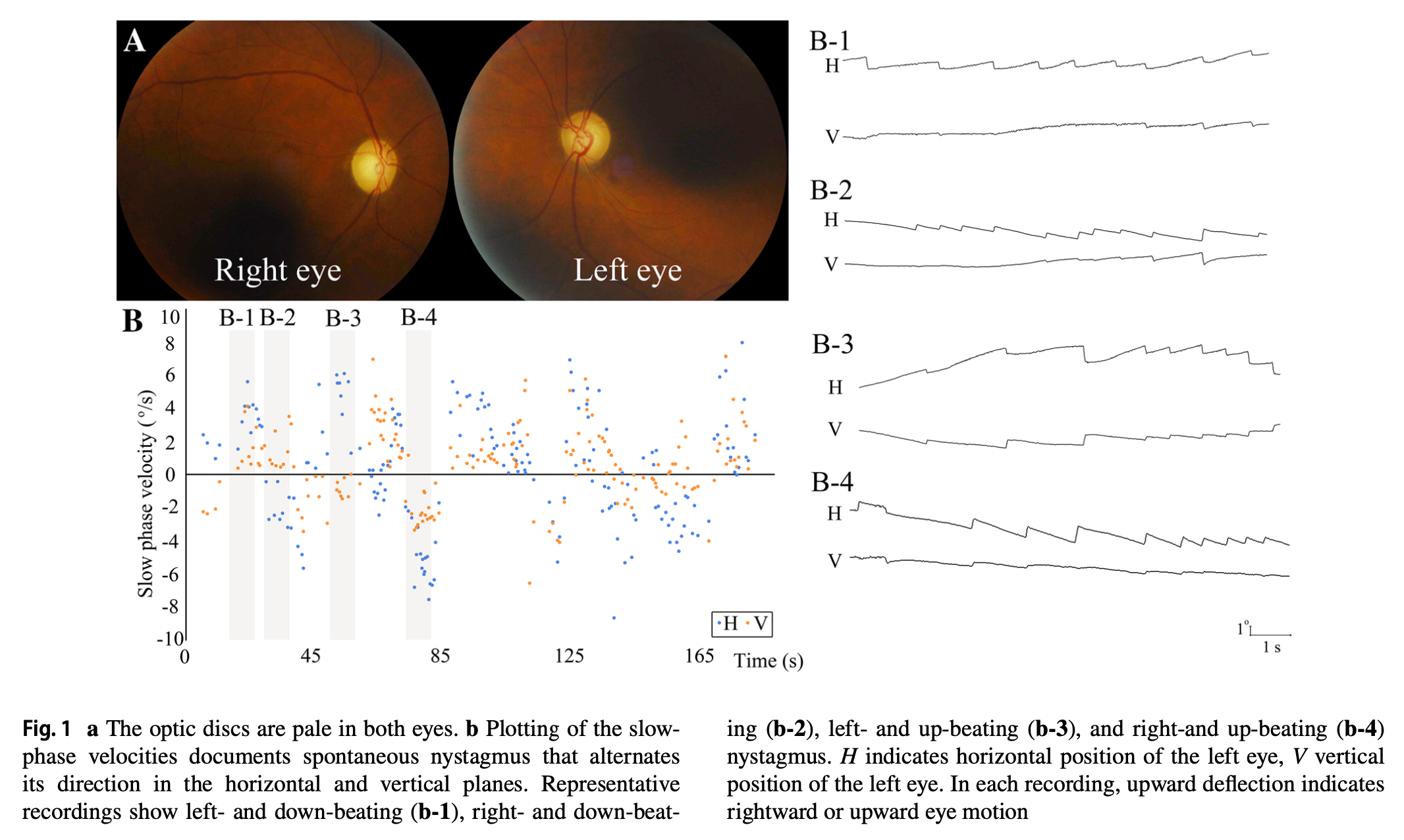
The Figure below, from Choi and colleagues (Choi et al. 2016), shows plots of the horizontal and vertical components of windmill nystagmus, as well as tracings of the nystagmus.

The Figure below, from Lee and colleagues (Lee et al. 2018a), shows plots of the horizontal and vertical components of windmill nystagmus, as well as tracings of the nystagmus.
Differential diagnosis
Most cases of windmill nystagmus appear in patients with gradual but relentlessly progressive bilateral visual loss (e.g., macular degeneration, retinitis pigmentosa). In such cases, an ophthalmologist should be involved in the patient’s care.
Windmill nystagmus of subacute onset (weeks) has also been reported as a paraneoplastic syndrome in a patient with normal vision. Therefore if windmill nystagmus develops subacutely in a patient with otherwise normal vision, a neoplastic workup should be undertaken.
Treatment
When windmill nystagmus is the result of visual loss, management is treatment (where possible) of the visual loss.
When windmill nystagmus occurs as a paraneoplastic syndrome, management is treatment of the underlying cancer.
Prognosis
In cases where windmill nystagmus is the result of visual loss, the prognosis of the visual loss itself is poor because of the underlying causes (macular degeneration, retinitis pigmentosa).
In cases where windmill nystagmus is the result of a paraneoplastic syndrome, the prognosis depends on the underlying malignancy. In the case reported by Lee and colleagues (Lee et al. 2018b), the windmill nystagmus improved after chemotherapy and radiotherapy.
References
Choi KD, Shin HK, Kim JS, Kim SH, Choi JH, Kim HJ, Zee DS (2016) Variants of windmill nystagmus. J Neurol 263: 1375-81. doi: 10.1007/s00415-016-8152-x
Lee SU, Jo SY, Kim HJ, Choi JY, Kim JS (2018a) Windmill nystagmus in a patient with subacute visual loss. J Neurol 265: 2737-2739. doi: 10.1007/s00415-018-9015-4
Lee SU, Kim HJ, Oh SW, Song EY, Choi JY, Kim JS (2018b) Pearls & Oy-sters: Windmill nystagmus in paraneoplastic cerebellar degeneration. Neurology 91: e1831-e1833. doi: 10.1212/WNL.0000000000006477
![]()