By Marcello Cherchi, MD PhD
For patients
Electrocochleography (ECoG) is a test of part of the hearing and balance components of the inner ear. Your doctor may consider checking this when evaluating for certain disorders of hearing and balance. During this test an audiologist or technician will place several surface electrodes on your body, including one in the ear canal, which some people find uncomfortable. During the test you will hear a series of clicks. The test is performed once in each ear. The test takes about 45 minutes. If your eardrum is damaged (such as a perforation), you should not take this test. If you have ear wax, this should be removed before the test; there are otherwise no special preparations for the test. There are no specific after-test instructions.
For clinicians
Overview
Electrocochleography (ECoG) is a far-field short-latency evoked potential test that supposedly assesses inner ear pressure. It is similar to an auditory evoked brainstem response (ABR), except that ECoG focuses on the morphology of wave I, and specifically on the ratio of the summation potential to the compound action potential, called the “SP/AP ratio.” This ratio is elevated in the condition of endolymphatic hydrops (elevated inner ear pressure), which most commonly occurs in Ménière’s disease. ECoG is not particularly sensitive or specific, so its results should not be interpreted in isolation.
Introduction
In theory, electrocochleography (ECoG) assesses inner ear pressure, and is thought to be abnormal in the presence of endolymphatic hydrops (increased pressure in the inner ear).
Physiology and neuroanatomy
Familiarity with the anatomy and physiology of the auditory system is helpful in understanding how ECoG works and how to interpret its results. We provide an overview of the auditory system elsewhere.
Sound, consisting of rhythmically alternating zones of higher and lower air pressure, reaches the tympanic membrane and causes it to move in an oscillating fashion. This oscillation is in turn is transmitted through the ossicular chain to the stapes footplate which, via a piston-like motion, induces fluid waves in the labyrinth. These fluid waves propagate through the cochlea and cause vibration at frequency-specific points along the cochlea, which results in oscillating shearing forces between the basal and tectorial membranes.
That oscillation of the basilar and tectorial membranes causes alternating ionic activity of type 1 (inner) cochlear hair cells whose frequency parallels that of the original auditory stimulus. This alternating current is called the cochlear microphonic (CM).
That same activity (of the type 1 cochlear hair cells) also induces a direct current that reflects the “time-displacement pattern of the cochlear partition in response to the stimulus envelope” (Dallos 1973; Dallos et al. 1972). This (unidirectional) direct current induces a shift in the cochlear microphonic’s electrical baseline, manifesting as the summation potential (SP).
The electrical potential derived from the cochlear microphonic triggers release of neurotransmitters (from the end-organ) into the synaptic cleft between the hair cells and the neurons of the spiral ganglion (the first-order neuron). The post-synaptic potential accumulates and, when it exceeds a specific threshold, triggers depolarization of the post-synaptic neuron. The summed responses of the synchronous firing of several thousand auditory nerve fibers results in an alternating current potential that is termed the compound action potential (AP). The use of the term “action potential” in this audiologic context has a specific meaning here that differs somewhat from what is familiar to neurologists, in that it refers to the aggregate activity of thousands of axons, rather than a single axon.
To summarize:
- The cochlear microphonic reflects the baseline (prior to receiving any acoustic stimulus).
- The summation potential reflects the activity of the type 1 (inner) cochlear hair cells.
- The compound action potential reflects the aggregate activity of firing in the auditory nerve (the first order neurons).
Curthoys and colleagues (Curthoys et al. 2021) provide a nuanced discussion of the cochlear microphonic, summation potential and compound action potential.
The resulting normal ECoG waveform appears as in the Figure below.
The overall waveform (out to 8 msec) is simply that of an auditory-evoked brainstem response (ABR). ECoG focuses on the morphology of the first wave of this response.
Several different parameters of the electrocochleogram have been studied. The most relevant one in clinical practice is the ratio of the summation potential (SP) to the compound action potential (AP), called the “SP/AP ratio,” which can be thought of as the ratio of the electrical activity of the cochlea to that of the auditory nerve.
In theory, the SP/AP ratio should be elevated in endolymphatic hydrops. The conventional explanation for this is that in endolymphatic hydrops, the cochlea is more flexible (it has been mechanically weakened by distension) and, since the basilar and tectorial membranes are more “floppy,” the activity of vibration will induce greater activity of the hair cells, thereby triggering a larger SP (and hence a larger SP/AP ratio).
The Figures below compare MR imaging of a normal labyrinth (left) to a labyrinth affected by endolymphatic hydrops (right).
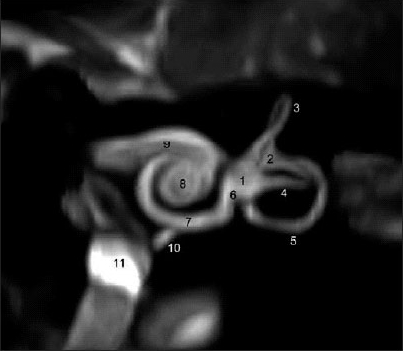 |
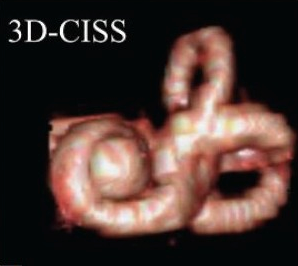 |
This explanation of the elevated SP/AP ratio in endolymphatic hydrops, while conventional, is not universally accepted. Dr. Timothy Hain (http://www.dizziness-and-balance.com/testing/ecog.html) has noted that the although the SP/AP ratio is elevated in endolymphatic hydrops (which is putatively a condition of elevated labyrinthine pressure), it is sometimes also elevated in perilymphatic fistula and superior canal dehiscence — conditions which logically should involve reduced labyrinthine pressure because there is a so-called “third window” (extra hole) that reduces the overall resistance in the system. Dr. Hain points out that these “opposite” circumstances can both cause bowing of Reissner’s membrane which, at least in theory, could provoked excessive hair cell activity (whether the bowing is due to increased or decreased labyrinthine pressure).
Equipment needed
The equipment used for ECoG is identical to that of ABR. The wave analysis is different, focusing on the morphology of wave I.
How to perform the test
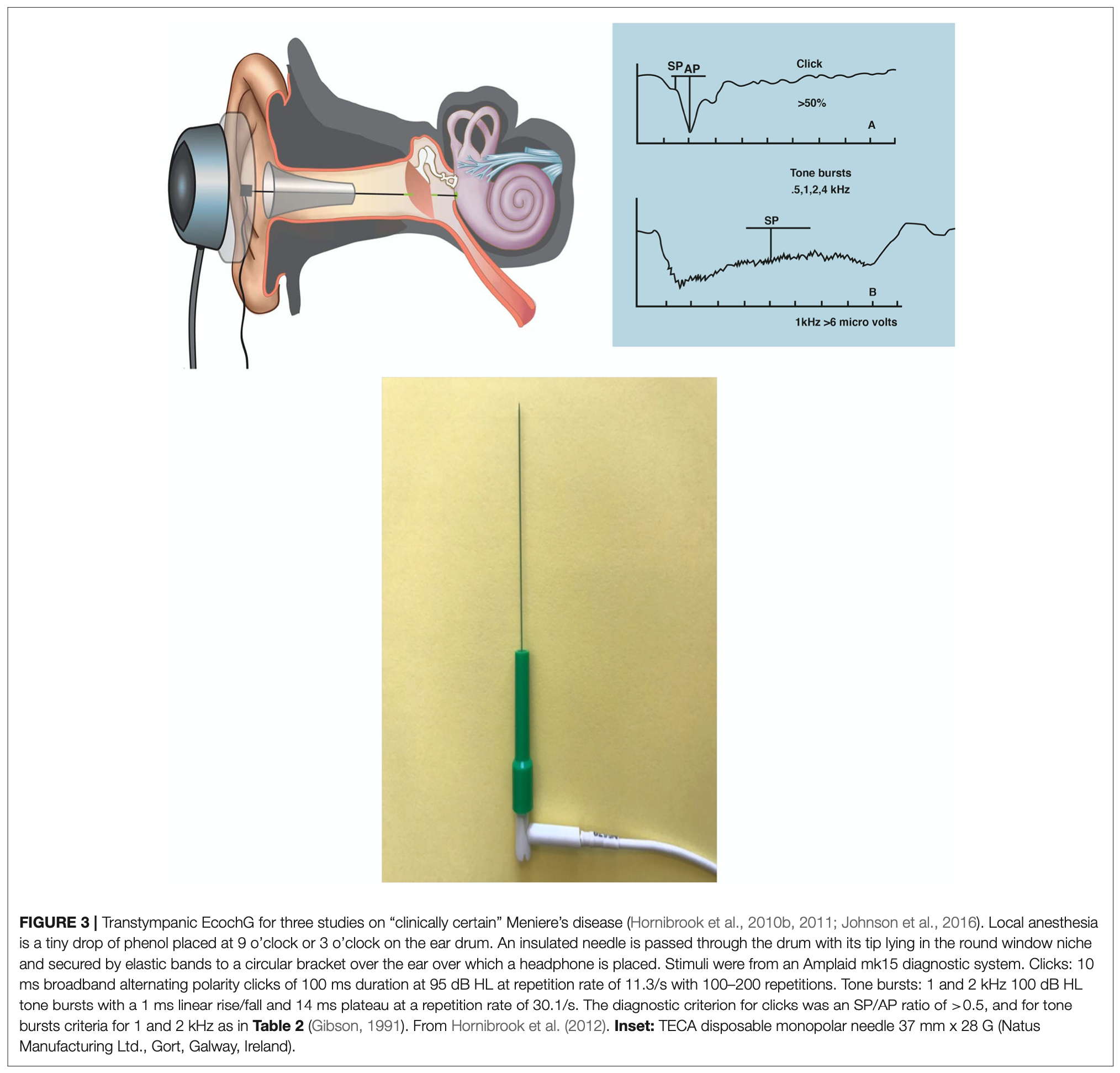
Originally ECoG was performed by placing a transtympanic electrode adjacent to the round window (Ruben et al. 1961), as illustrated in the Figure below, from Hornibrook (Hornibrook 2017). The advantage of this approach was that it was possible to collect more robust responses. The disadvantage of this approach is that it was an invasive procedure requiring at least local anesthesia.
Later approaches, using sensitive electrodes and signal averaging, were able to elicit useful ECoG responses non-invasively by placing electrodes on the tympanic membrane itself (Attias et al. 2008; Mullatti et al. 1999).
The technique for performing ECoG involves:
- The acoustic stimulus is similar to that used in brainstem ABRs. A variety of protocols (different parameter combinations of click, tone burst, frequency, duration, etc.) have been explored.
- Electrode placement:
- Primary (+): Ear canal or tympanic membrane.
- Secondary (-): Contralateral earlobe or mastoid.
- Common: Nasion.
What this test assesses
In theory, ECoG assesses inner ear pressure.
How to interpret the test results
Even when ECoG is done properly, the test does not have a very impressive sensitivity or specificity. Therefore, as with virtually any test in medicine, the result must be interpreted in the context of whatever else is known about the patient. When interpreting an ECoG, it is especially helpful to have a recent audiogram.
Ideally a clinical laboratory should establish its own normative reference range for the SP/AP ratio. Those that do not do so often use a default SP/AP ratio of 0.50.
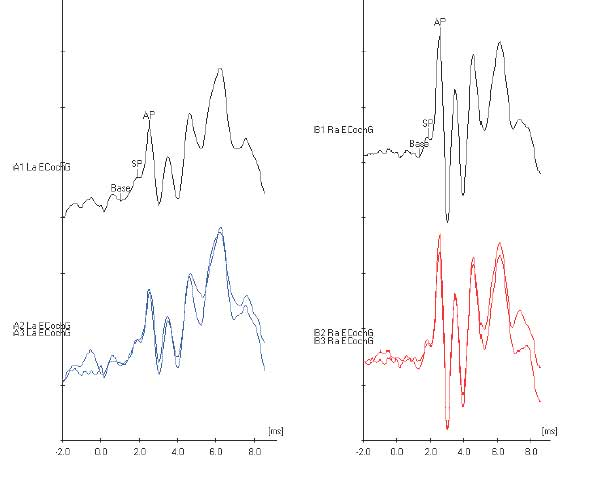
The Figure below shows an ECoG in which the left ear has a normal SP/AP ratio, and the right ear has an elevated SP/AP ratio.
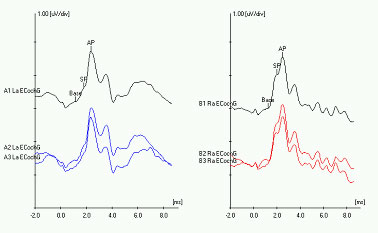
Figure 5: Electrocochleography showing a normal response on the left ear (left panel, blue tracing), and an elevated SP/AP ratio on the right ear (right panel, red tracing). From http://www.dizziness-and-balance.com/testing/ecog.html (accessed 2/5/2016).
Limitations
In ECoG, the electrode is closer to the base of the cochlea than to any other part of the cochlea, which means that will more easily detect cochlear activity towards the basal end — in other words, higher frequencies. This is the reason why, in order for ECoG to be useful, the patient must have some degree of intact high frequency hearing; generally, hearing around 4 kHz should be no worse than 50 dB.
For patients with Ménière’s disease (at least in the early stages), this hearing requirement is usually met because their hearing loss primarily involves the lower frequencies. However, in advanced Ménière’s disease, or in people who have other causes of high frequency hearing loss (such as presbycusis), the ECoG may not yield useful results.
Contraindications
Patients with a recent injury of the external ear, or otitis externa, may be unable to tolerate instrumentation of the external auditory canal.
Pitfalls
ECoG is a difficult procedure for a variety of reasons, including:
- Electrode placement can be challenging
- The signal is difficult to elicit and is of low amplitude
- There is often artifact and a poor signal-to-noise ratio
For these reasons, the test should be performed by a seasoned technician or experienced audiologist.
There are several potential sources of error in performing ECoG, including:
- Mechanical failures – the headphones can, and do, burn out.
- Improper technique, or an inexperienced technician/audiologist.
- Electrical interference with inadequately shielded equipment.
- Significant high frequency hearing loss. (This is one of the reasons why a recent audiogram should be available.)
When is the test indicated
ECoG is indicated for cases of suspected endolymphatic hydrops, which in clinical practice usually is from Ménière’s disease.
Diseases that may be diagnosed by this test
The finding of an elevated SP/AP ratio on ECoG suggests endolymphatic hydrops. In clinical practice the most common cause of endolymphatic hydrops is Ménière’s disease; other causes (e.g., otosyphilis) are rare. This is why ECoG is sometimes referred to as a “Ménière’s test,” though that is technically only partially correct.
References
Attias J, Nageris B, Ralph J, Vajda J, Rappaport ZH (2008) Hearing preservation using combined monitoring of extra-tympanic electrocochleography and auditory brainstem responses during acoustic neuroma surgery. Int J Audiol 47: 178-84. doi: 10.1080/14992020701802422
Curthoys IS, Grant JW, Pastras CJ, Frohlich L, Brown DJ (2021) Similarities and Differences Between Vestibular and Cochlear Systems – A Review of Clinical and Physiological Evidence. Front Neurosci 15: 695179. doi: 10.3389/fnins.2021.695179
Dallos P (1973) The auditory periphery; biophysics and physiology. Academic Press, New York
Dallos P, Schoeny ZG, Cheatham MA (1972) Cochlear summating potentials. Descriptive aspects. Acta Otolaryngol Suppl 302: 1-46
Hornibrook J (2017) a section of the journal Frontiers in Neuroscience Tone Burst Electrocochleography for the Diagnosis of Clinically Certain Meniere’s Disease. Frontiers in Human Neuroscience 11:301: 9 pages. doi: 10.3389/fnins.2017.00301
Mullatti N, Coakham HB, Maw AR, Butler SR, Morgan MH (1999) Intraoperative monitoring during surgery for acoustic neuroma: benefits of an extratympanic intrameatal electrode. J Neurol Neurosurg Psychiatry 66: 591-9. doi: 10.1136/jnnp.66.5.591
Ruben RJ, Bordley JE, Lieberman AT (1961) Cochlear potentials in man. Laryngoscope 71: 1141-64. doi: 10.1288/00005537-196110000-00001
![]()