By Marcello Cherchi, MD PhD
For patients
Here are answers to some of the most common questions about retinal imaging.
|
What is this test? |
Retinal imaging involves taking pictures of the back of the eye. This can be done with a special regular light camera (called retinal photography) or infrared light (called optical coherence tomography). |
|
What is this test looking for? |
This test looks for whether the rotational position of the retina is normal or abnormal. |
|
Is this test experimental or investigational? |
This test is approved by the Food and Drug Administration. It is neither experimental nor investigational. |
|
What happens during this test? |
When taking retinal pictures the technician will have you rest your chin and forehead in a head stabilization frame while they take pictures of the back of your eyes through your pupils. One or more pictures may be taken of each eye.
|
|
Is this test uncomfortable? |
Some patients find that the bright light (for retinal photography) can be uncomfortable. Optical coherence tomography is not uncomfortable. |
|
How long does this test take? |
Retinal imaging takes about one minute per eye. |
|
Do I have to prepare for this test? |
There are no specific preparations for this test. Most patients do not need to have their eyes dilated for retinal imaging. |
|
Are there any special instructions for what to do after the test? |
There are no special instructions for what to do after this test. |
For clinicians
Overview
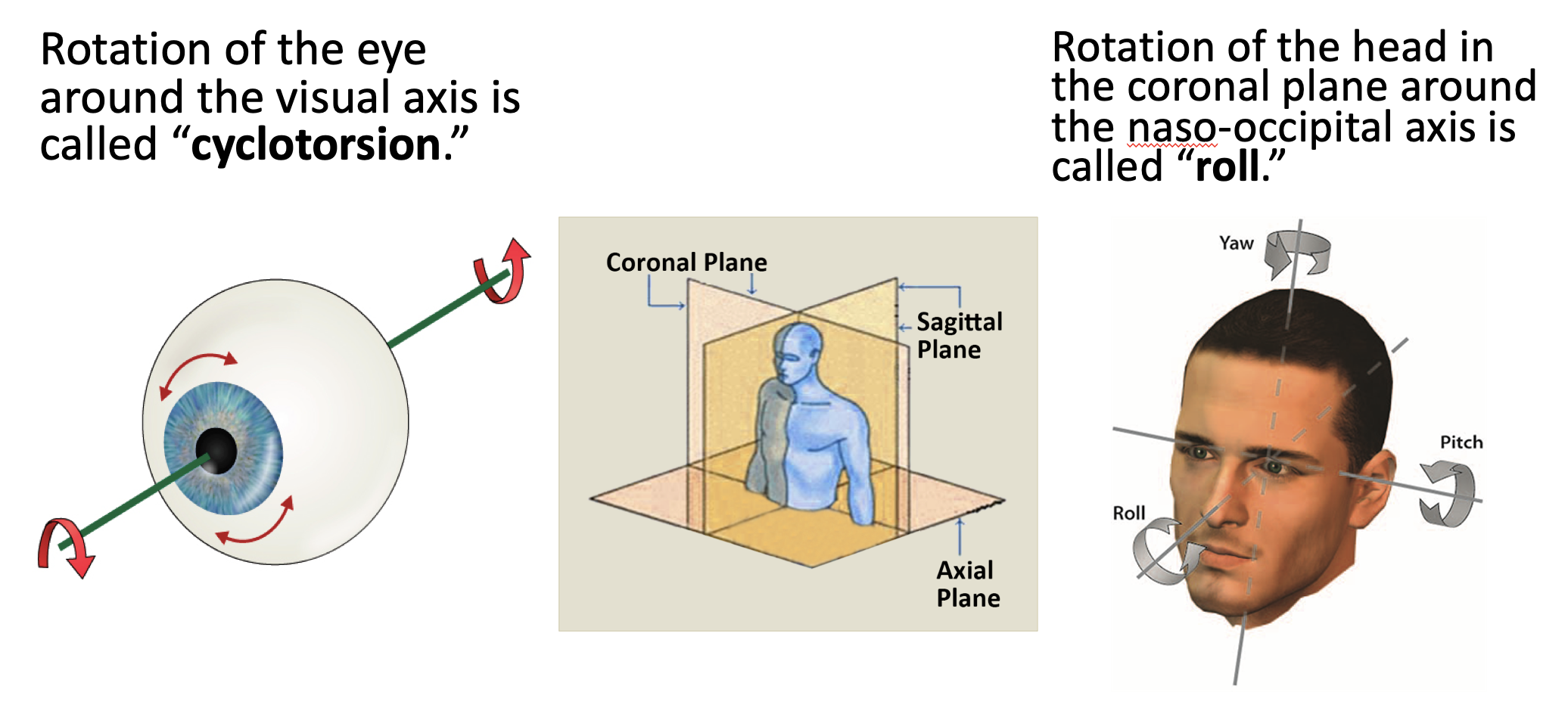
Cyclorotation (rotation of the eyeballs in the coronal plane) occurs in normal states (such as ocular counter-roll) and pathological states (such as vestibular neuritis). Unilateral vestibular weakness (such as vestibular neuritis) affecting utricular pathways can cause ipsilesional cyclodeviation (which can be detected on retinal photography and optical coherence tomography), and asymmetrical cyclotropic nystagmus (which can be detected by scleral search coils and by video oculography).
The Figure below illustrates cyclotorsion and roll.
Introduction
When the head rotates in the coronal (“roll”) plane, reflex eye movements occur.
The Figure below shows normal ocular counter-roll.

In normal ocular counter-rolling:
- When the patient tilts the head to the right:
- The right eye elevates and intorts.
- The left eye depresses and extorts.
- When the patient tilts the head to the left:
- The right eye depresses and extorts.
- The left eye elevates and intorts.
The teleological purpose of these eye movements is to keep the eyes level with the ground despite changes in head orientation.
- The purpose of the ocular elevation/depression is to keep the inter-ocular line parallel to the earth-horizontal plane.
- The purpose of the ocular intorsion/extorsion is to keep the plane of the global equators parallel to the earth-horizontal plane.
In tabular format:
|
Head tilt to right |
Head tilt to left |
|
|
Vertical eye movements. Purpose is to keep inter-ocular line parallel to earth-horizontal plane. |
Right eye elevates. Left eye depresses. |
Right eye depresses. Left eye elevates. |
|
Torsional eye movements. Purpose is to keep the plane of the global equators parallel to the earth-horizontal plane. |
Right eye intorts. Left eye extorts. |
Right eye extorts. Left eye intorts. |
Pathological states
In some pathological states this ocular counter-rolling reaction is disrupted.
For example, in the acute stage of unilateral vestibular loss, if utricular afferents are affected, then the eyes tend to exhibit pathological cyclotropia (cyclodeviation, cyclotorsion) towards the side of the vestibular weakness. This is found in the majority of cases, though studies report variable rates, from 61% of cases (Choi et al. 2015), to 72% of cases (Choi et al. 2007), to 82% of cases (Kim et al. 2008). The cyclotorsion may be more consistent in the ipsilesional eye than the contralesional eye (Lapenna et al. 2018).
However, cyclotropia cannot be assessed simply on face-to-face examination, nor on infrared oculography, since the iris pattern does not have any orienting landmarks.
Measuring cyclotropia with retinal imaging
Cycloposition can be measured by imaging the retina.
“An objective way of measuring ocular cycloposition is to image the retina and calculate the disc–foveal angle — the angle formed by the intersection of one line drawn through the center of the optic disc and the center of the fovea, and a second line representing earth horizontal. The most common imaging modality for this purpose is visible light retinal photography, though optical coherence tomography (OCT) can be used for this as well” (Cherchi 2019).
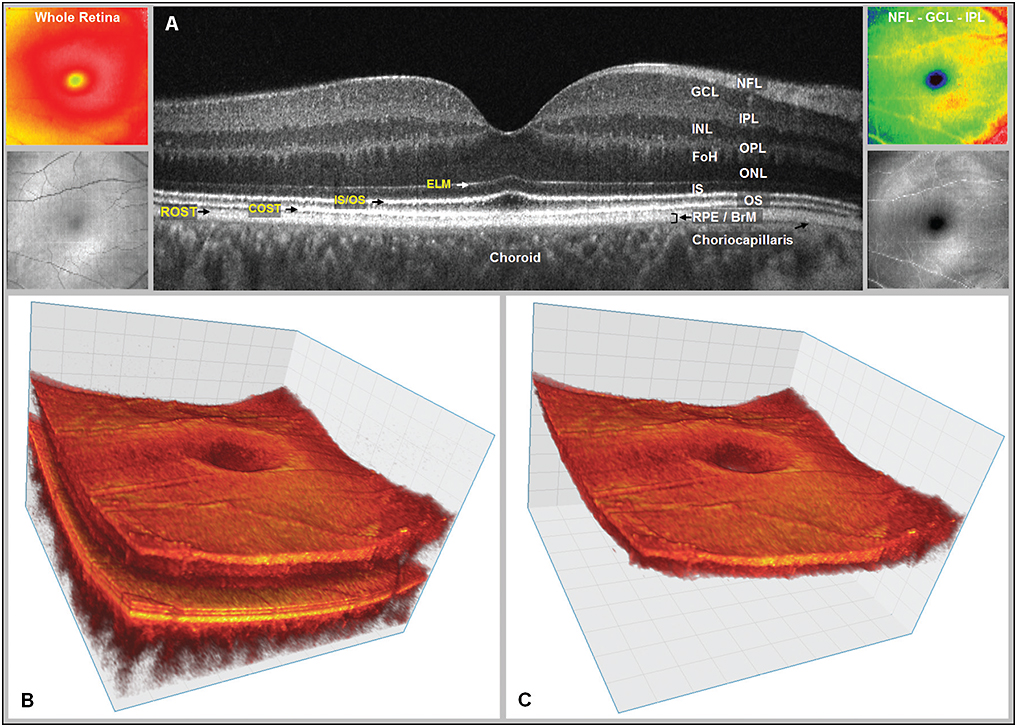
Our preference is to utilize optical coherence tomography when available, which has several advantages over regular retinal photography. Optical coherence tomography (OCT) is a very accurate way to determine the disc-foveal line, because it identifies the relevant structures based on the topography (shape) of the retina. Some OCT software platforms offer automatic calculation of the disc-foveal angle (Lengwiler et al. 2018).
The Figure below, from Moisseiev and colleagues (Moisseiev et al. 2016), shows an OCT three-dimensional rendition of the macula.
The Figure below, from Lengwiler and colleagues (Lengwiler et al. 2018), shows OCT-based calculation of the disc-foveal angle.

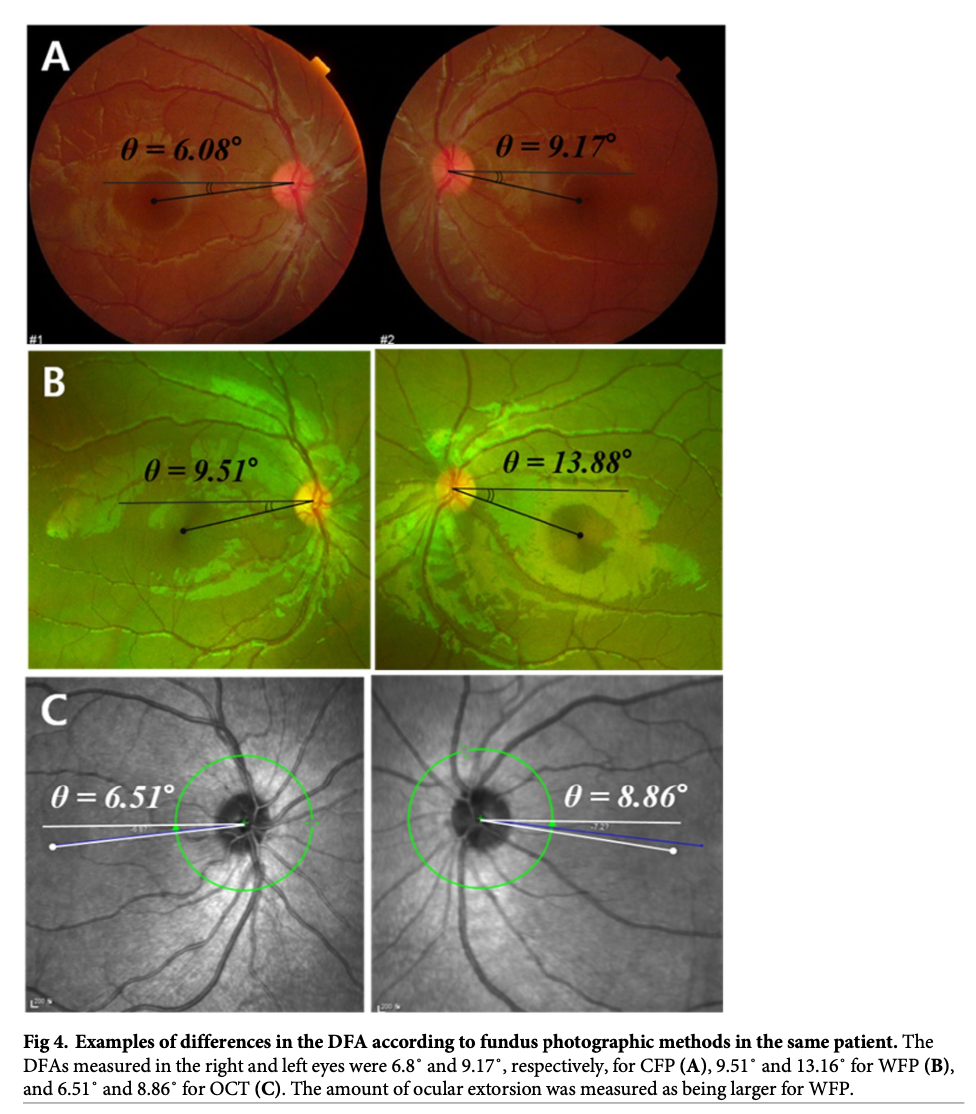
There is some variability among the different retinal imaging modalities. Kang and colleagues (Kang et al. 2020) compared conventional fundus photography, wide-field fundus photography, and optical coherence tomography for estimating the disc-foveal angle. They reported that conventional fundus photography and optical coherence tomography were very similar, while results from wide-field fundus photography were less replicable.
The Figure below, from Kang and colleagues (Kang et al. 2020), shows a comparison of the three imaging modalities in one and the same patient.
Measuring dynamic cyclotorsion with infrared video oculography
The discussion to this point has focused on static ocular cycloposition (cyclotropia). In cases of unilateral vestibular weakness involving utricular afferents, it turns out that cyclotorsional nystagmus (in response to head roll in the coronal plane) can be asymmetrical.
It is possible to detect cyclotorsional nystagmus using magnetic scleral search coils, or infrared video oculography (Otero-Millan et al. 2017; Sadeghpour et al. 2021) using an iris torsional detection algorithm developed by Otero-Millan and colleagues (Otero-Millan et al. 2015).
As optical coherence tomography (OCT) improves in terms of temporal resolution, it may also become possible to use OCT for detecting nystagmus (Brodsky et al. 2014), including torsional nystagmus.
References
Brodsky MC, Klaehn L, Goddard SM, Link TP (2014) Heidelberg Spectralis infrared video imaging: a clinical tool for diagnosing ocular torsional instability. J AAPOS 18: 306-7. doi: 10.1016/j.jaapos.2014.01.009
Cherchi M (2019) Utricular function in vestibular neuritis: a pilot study of concordance/discordance between ocular vestibular evoked myogenic potentials and ocular cycloposition. Exp Brain Res. doi: 10.1007/s00221-019-05529-8
Choi JW, Kang SI, Rhee JH, Choi BY, Kim JS, Koo JW (2015) Clinical implication of ocular torsion in peripheral vestibulopathy. Eur Arch Otorhinolaryngol 272: 1613-7. doi: 10.1007/s00405-014-2952-3
Choi KD, Oh SY, Kim HJ, Koo JW, Cho BM, Kim JS (2007) Recovery of vestibular imbalances after vestibular neuritis. Laryngoscope 117: 1307-12. doi: 10.1097/MLG.0b013e31805c08ac
Kang H, Lee SJ, Shin HJ, Lee AG (2020) Measuring ocular torsion and its variations using different nonmydriatic fundus photographic methods. PLoS One 15: e0244230. doi: 10.1371/journal.pone.0244230
Kim HA, Hong JH, Lee H, Yi HA, Lee SR, Lee SY, Jang BC, Ahn BH, Baloh RW (2008) Otolith dysfunction in vestibular neuritis: recovery pattern and a predictor of symptom recovery. Neurology 70: 449-53. doi: 10.1212/01.wnl.0000297554.21221.a0
Lapenna R, Pellegrino A, Ricci G, Cagini C, Faralli M (2018) Binocular cyclotorsion in superior vestibular neuritis. Acta Otorhinolaryngol Ital 38: 138-144. doi: 10.14639/0392-100X-1645
Lengwiler F, Rappoport D, Jaggi GP, Landau K, Traber GL (2018) Reliability of Cyclotorsion measurements using Scanning Laser Ophthalmoscopy imaging in healthy subjects: the CySLO study. Br J Ophthalmol 102: 535-538. doi: 10.1136/bjophthalmol-2017-310396
Moisseiev E, Park S, Yiu G, Werner JS, Zawadzki RJ (2016) The third dimension: advantages of 3D-OCT in retina. Retinal Physician.
Otero-Millan J, Roberts DC, Lasker A, Zee DS, Kheradmand A (2015) Knowing what the brain is seeing in three dimensions: A novel, noninvasive, sensitive, accurate, and low-noise technique for measuring ocular torsion. J Vis 15: 11. doi: 10.1167/15.14.11
Otero-Millan J, Trevino C, Winnick A, Zee DS, Carey JP, Kheradmand A (2017) The video ocular counter-roll (vOCR): a clinical test to detect loss of otolith-ocular function. Acta Otolaryngol 137: 593-597. doi: 10.1080/00016489.2016.1269364
Sadeghpour S, Fornasari F, Otero-Millan J, Carey J, Zee D, Kheradmand A, Motor O, Sadeghpour, Fornasari O-M, Zee K (2021) Evaluation of the Video Ocular Counter-Roll (vOCR) as a New Clinical Test of Otolith Function in Peripheral Vestibulopathy. JAMA Otolaryngology – Head and Neck Surgery. doi: 10.1001/jamaoto.2021.0176
![]()