By Marcello Cherchi, MD PhD
For patients
Some practitioners, particularly physical therapists, maintain that turning the head (while keeping the trunk still) and monitoring for whether this provokes any symptoms, is a way of “testing” the vertebral artery — one of the arteries that supplies blood to the brain. Researchers disagree about whether this test is useful.
For clinicians
Practical summary
“Vertebral artery testing” (VAT) refers to the practice (mostly by physical therapists) of rotating the patient’s head around the vertical axis (while keeping the trunk stationary) and monitoring for symptoms, in the belief that this can assess the patient’s risk of vascular compromise from further neck manipulations. Rotation of the head with respect to the shoulders exerts compressive and torquing forces on the vertebral arteries as they pass through the cervical vertebral foramina, particularly between C1 and C2. One risk of extrinsic compression of the vertebral artery is transient occlusion of flow, sometimes manifesting as bow hunter syndrome. A risk of extrinsic compression and torquing is vertebral artery dissection. Despite study of animal models, human cadaveric material, and in-vivo imaging studies, there is disagreement in the literature about how significant these risks are, though most such literature recommends caution in patients with known vascular risk factors. Thus the clinical value of “vertebral artery testing” (VAT) in assessing such risks is unclear; most of the literature, and meta-analyses of that literature, conclude that VAT is not useful.
Discussion
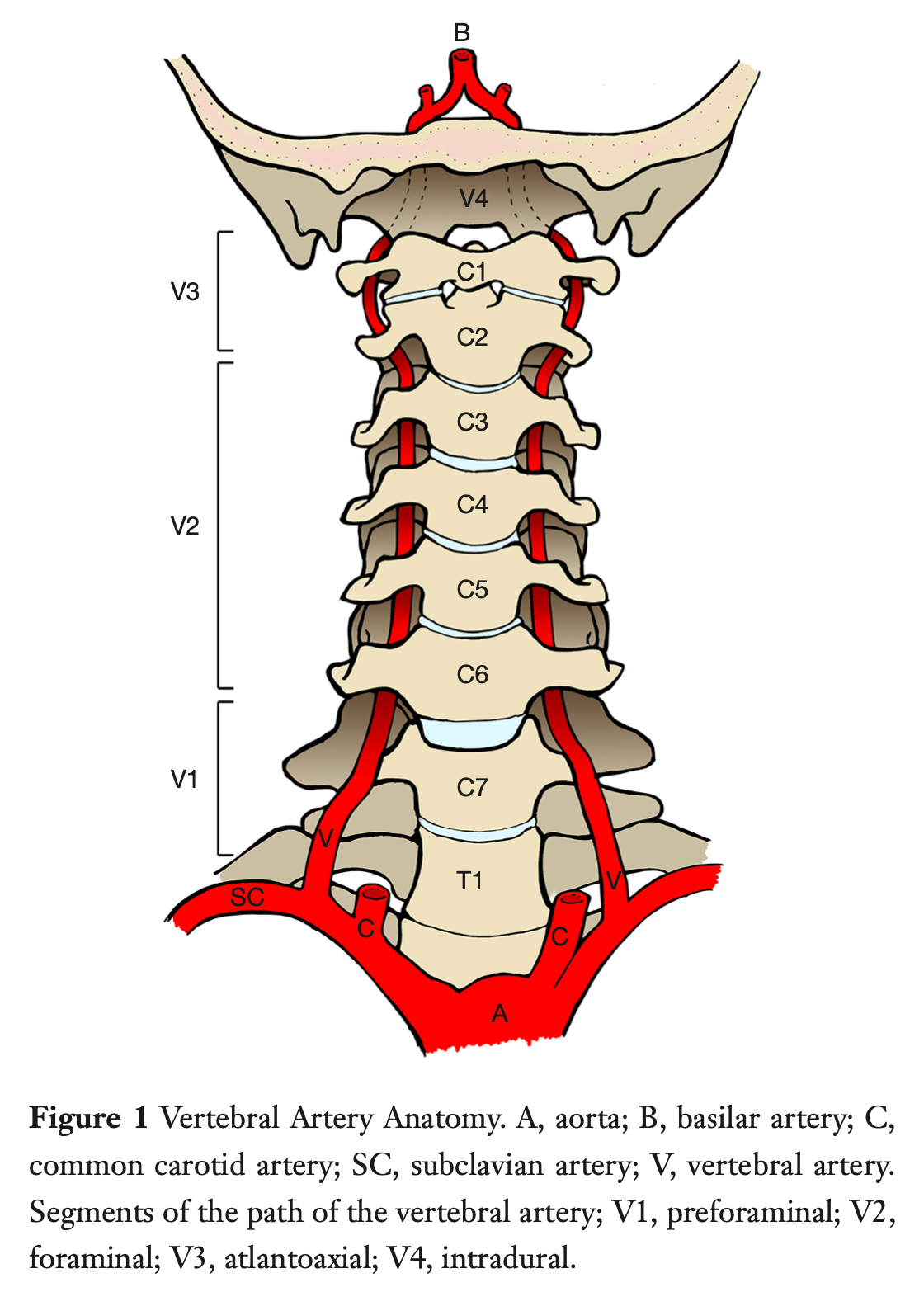
After the vertebral arteries branch off the subclavian arteries they ascend through cervical vertebral foramina at each level before joining to form the basilar artery.
This is shown in the Figure below, from Shafafy and colleagues (Shafafy et al. 2017).
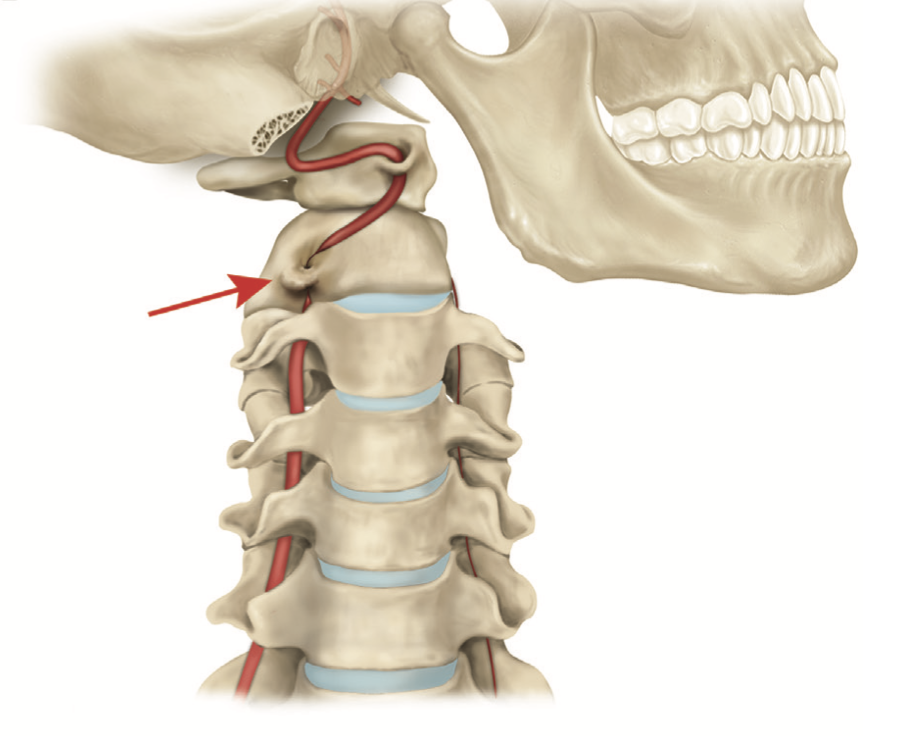
Head movement in yaw (rotation of the head around the vertical axis with respect to the shoulders) exerts torque and stretch forces on the vertebral arteries as they pass through the arterial foramina in the cervical vertebrae, particularly in the segment between the C1 and C2 foramina.
This is shown in the Figure below from Choi and colleagues (Choi et al. 2013).
The effects of these forces on the vertebral arteries raises two main concerns. The first is transient occlusion of the lumen due to extrinsic compression; this is sometimes referred to as bow hunter syndrome of which there are case reports and small series (Go et al. 2013; Hong et al. 2022; Kamouchi et al. 2003; Li et al. 2019; Lu et al. 2010; Sakaguchi et al. 2003; Sarkar et al. 2014; Sorensen 1978; Takafumi et al. 2024; Weintraub and Khoury 2004; Xue et al. 2023; Zaidi et al. 2014), and broader reviews (Cornelius et al. 2012; Duan et al. 2016). The second is injury to the vascular wall resulting in vertebral artery dissection (Albuquerque et al. 2011; Chen et al. 2006; Haldeman et al. 2001; Vibert et al. 1993), which can result in stroke (Charles et al. 1992; Chen et al. 2006; Choi et al. 2006; Eliezer et al. 2019).
Despite analyses of possible risk factors (Thomas et al. 2011), it is difficult to predict which individuals are vulnerable to these effects. This may be due in part to the considerable variability in the normal anatomy of vertebral arteries (Tudose et al. 2023).
Canine (Kawchuk et al. 2004) and porcine (Licht et al. 1999) animal models have been proposed for studying vertebral arterial mechanics, and while interesting, they comprise an approximation of the situation in humans.
Human cadaveric studies of vertebral arterial mechanics generally conclude that, “The engineering strains during cervical spinal manipulations… impart stretches on the VA [vertebral artery] that are well within the normal physiologic range of neck motion” (Wuest et al. 2010), and that “SMT [spinal manipulative therapy] resulted in strains to the VA that were almost an order of magnitude lower than the strains required to mechanically disrupt it” (Symons et al. 2002). Not all cadaveric studies reach such conclusions (Li et al. 1999).
Doppler ultrasonography is a commonly used approach for studying in vivo vertebral artery flow during cervical manipulations (Haynes 2000; Haynes et al. 2000; Shum et al. 2017), though other modalities include MR angiography (Haynes et al. 2002). The majority of vascular imaging studies observe no significant changes in various head-on-neck positions (Erhardt et al. 2015; Haynes et al. 2002; Leenaerts et al. 2020; Mitchell 2007; Moll et al. 2023; Thiel et al. 1994; Yelverton et al. 2020; Zaina et al. 2003); a minority of studies express a dissenting opinion (Arnold et al. 2004; Mitchell et al. 2004; Mitchell 2003; Thomas et al. 2015).
An extensive systematic review conducted by academic physical therapists (Richter and Reinking 2005) concluded that:
“The VA [vertebral artery] test has been called a clearing test, implying that a negative test ‘clears’ the patient of VBI [vertebrobasilar insufficiency] and allows cervical mobilization or manipulation if indicated. The diagnostic accuracy data we found do not support this interpretation… We believe the strength of the evidence for VA testing is weak” (Richter and Reinking 2005).
Several studies conclude that overall the evidence in support of vertebral artery testing is weak (Mitchell 2008; Richter and Reinking 2005) and that more studies are needed before any firm conclusions can be drawn (Rivett et al. 1999). Some authors take the more extreme position that vertebral artery testing should be abandoned altogether (Hutting et al. 2020), while others conclude that it would be premature to do so (Thomas and Treleaven 2020).
Most studies expressing caution take the position that cervical spine manipulations should be avoided in patients with a history suggestive of vertebral artery dissection (injury, neck pain) or known vascular risk factors (Thiel and Rix 2005), whereas in individuals without such risk factors (Yelverton et al. 2020), cervical spine manipulations are safe.
Our reading of this literature is that:
- The overall risk from the more rapid and larger-amplitude head-on-neck movements involved in chiropractic manipulation logically produces more robust forces, from which the risk of sequelae (such as vertebral arterial dissection) appears to be higher.
- In contrast, the slower and smaller head-on-neck movements entailed by, for example, vestibular rehabilitation therapy management of benign paroxysmal positional vertigo (BPPV), exert more modest forces, with commensurately lower risk. The risk can be further reduced through modification of standard maneuvers; for example, when treating lateral canal BPPV, rather than rotating the head 90 degrees to either side (with respect to the trunk) during the supine roll test, the treating clinician can rotate the entire body, thereby keeping the head-on-neck position stable (with no relative rotation), while still achieving the head positioned with respect to gravity such that canaliths can be repositioned.
References
Albuquerque FC, Hu YC, Dashti SR, Abla AA, Clark JC, Alkire B, Theodore N, McDougall CG (2011) Craniocervical arterial dissections as sequelae of chiropractic manipulation: patterns of injury and management. J Neurosurg 115: 1197-205. doi: 10.3171/2011.8.JNS111212
Arnold C, Bourassa R, Langer T, Stoneham G (2004) Doppler studies evaluating the effect of a physical therapy screening protocol on vertebral artery blood flow. Man Ther 9: 13-21. doi: 10.1016/s1356-689x(03)00087-0
Charles N, Froment C, Rode G, Vighetto A, Turjman F, Trillet M, Aimard G (1992) Vertigo and upside down vision due to an infarct in the territory of the medial branch of the posterior inferior cerebellar artery caused by dissection of a vertebral artery. J Neurol Neurosurg Psychiatry 55: 188-9. doi: 10.1136/jnnp.55.3.188
Chen WL, Chern CH, Wu YL, Lee CH (2006) Vertebral artery dissection and cerebellar infarction following chiropractic manipulation. Emerg Med J 23: e1. doi: 10.1136/emj.2004.015636
Choi KD, Choi JH, Kim JS, Kim HJ, Kim MJ, Lee TH, Lee H, Moon IS, Oh HJ, Kim JI (2013) Rotational vertebral artery occlusion: mechanisms and long-term outcome. Stroke 44: 1817-24. doi: 10.1161/STROKEAHA.113.001219
Choi KD, Chun JU, Han MG, Park SH, Kim JS (2006) Embolic internal auditory artery infarction from vertebral artery dissection. J Neurol Sci 246: 169-72. doi: 10.1016/j.jns.2006.02.014
Cornelius JF, George B, N’Dri Oka D, Spiriev T, Steiger HJ, Hanggi D (2012) Bow-hunter’s syndrome caused by dynamic vertebral artery stenosis at the cranio-cervical junction–a management algorithm based on a systematic review and a clinical series. Neurosurg Rev 35: 127-35; discussion 135. doi: 10.1007/s10143-011-0343-4
Duan G, Xu J, Shi J, Cao Y (2016) Advances in the Pathogenesis, Diagnosis and Treatment of Bow Hunter’s Syndrome: A Comprehensive Review of the Literature. Interv Neurol 5: 29-38. doi: 10.1159/000444306
Eliezer M, Verillaud B, Guichard JP, Kania R, Toupet M, Herman P, Houdart E, Hautefort C (2019) Labyrinthine infarction caused by vertebral artery dissection: consideration based on MRI. J Neurol. doi: 10.1007/s00415-019-09456-0
Erhardt JW, Windsor BA, Kerry R, Hoekstra C, Powell DW, Porter-Hoke A, Taylor A (2015) The immediate effect of atlanto-axial high velocity thrust techniques on blood flow in the vertebral artery: A randomized controlled trial. Man Ther 20: 614-22. doi: 10.1016/j.math.2015.02.008
Go G, Hwang SH, Park IS, Park H (2013) Rotational Vertebral Artery Compression : Bow Hunter’s Syndrome. J Korean Neurosurg Soc 54: 243-5. doi: 10.3340/jkns.2013.54.3.243
Haldeman S, Carey P, Townsend M, Papadopoulos C (2001) Arterial dissections following cervical manipulation: the chiropractic experience. CMAJ 165: 905-6.
Haynes MJ (2000) Vertebral arteries and neck rotation: Doppler velocimeter and duplex results compared. Ultrasound Med Biol 26: 57-62. doi: 10.1016/s0301-5629(99)00132-5
Haynes MJ, Cala LA, Melsom A, Mastaglia FL, Milne N, McGeachie JK (2002) Vertebral arteries and cervical rotation: modeling and magnetic resonance angiography studies. J Manipulative Physiol Ther 25: 370-83. doi: 10.1067/mmt.2002.126130
Haynes MJ, Hart R, McGeachie J (2000) Vertebral arteries and neck rotation: Doppler velocimeter interexaminer reliability. Ultrasound Med Biol 26: 1363-7. doi: 10.1016/s0301-5629(00)00303-3
Hong IS, Jung EH, Kim KH, Kwon HJ, Choi SW, Kim SH, Koh HS, Youm JY, Lee HJ (2022) Rotational Vertebral Artery Syndrome (Bow Hunter’s Syndrome): A Rare Differential Diagnosis in Patients With Syncope. Korean J Neurotrauma 18: 410-417. doi: 10.13004/kjnt.2022.18.e63
Hutting N, Kranenburg HAR, Kerry R (2020) Yes, we should abandon pre-treatment positional testing of the cervical spine. Musculoskelet Sci Pract 49: 102181. doi: 10.1016/j.msksp.2020.102181
Kamouchi M, Kishikawa K, Matsuo R, Yasumori K, Inoue T, Okada Y, Ibayashi S (2003) Ultrasonographic detection of extracranial vertebral artery compression in bow hunter’s brain ischemia caused by neck rotation. Cerebrovasc Dis 16: 303-5. doi: 10.1159/000071134
Kawchuk GN, Wynd S, Anderson T (2004) Defining the effect of cervical manipulation on vertebral artery integrity: establishment of an animal model. J Manipulative Physiol Ther 27: 539-46. doi: 10.1016/j.jmpt.2004.10.005
Leenaerts T, Molenaar W, Cattrysse E (2020) Changes in Vertebral Arterial Blood Flow During Premanipulative Tests in Participants With Upper Cervical Spine Motion Restriction. J Manipulative Physiol Ther 43: 134-143. doi: 10.1016/j.jmpt.2019.10.002
Li Q, Xie P, Yang WS, Yan B, Davis S, Caplan LR (2019) Vertebral Artery Compression Syndrome. Front Neurol 10: 1075. doi: 10.3389/fneur.2019.01075
Li YK, Zhang YK, Lu CM, Zhong SZ (1999) Changes and implications of blood flow velocity of the vertebral artery during rotation and extension of the head. J Manipulative Physiol Ther 22: 91-5. doi: 10.1016/s0161-4754(99)70113-2
Licht PB, Christensen HW, Svendensen P, Hoilund-Carlsen PF (1999) Vertebral artery flow and cervical manipulation: an experimental study. J Manipulative Physiol Ther 22: 431-5. doi: 10.1016/s0161-4754(99)70030-8
Lu DC, Zador Z, Mummaneni PV, Lawton MT (2010) Rotational vertebral artery occlusion-series of 9 cases. Neurosurgery 67: 1066-72; discussion 1072. doi: 10.1227/NEU.0b013e3181ee36db
Mitchell J (2007) Doppler insonation of vertebral artery blood flow changes associated with cervical spine rotation: Implications for manual therapists. Physiother Theory Pract 23: 303-13. doi: 10.1080/09593980701593771
Mitchell J (2008) Is mechanical deformation of the suboccipital vertebral artery during cervical spine rotation responsible for vertebrobasilar insufficiency? Physiother Res Int 13: 53-66. doi: 10.1002/pri.370
Mitchell J, Keene D, Dyson C, Harvey L, Pruvey C, Phillips R (2004) Is cervical spine rotation, as used in the standard vertebrobasilar insufficiency test, associated with a measureable change in intracranial vertebral artery blood flow? Man Ther 9: 220-7. doi: 10.1016/j.math.2004.03.005
Mitchell JA (2003) Changes in vertebral artery blood flow following normal rotation of the cervical spine. J Manipulative Physiol Ther 26: 347-51. doi: 10.1016/S0161-4754(03)00074-5
Moll F, Sleiman M, Sturm D, Kerry R, von Piekartz H (2023) Pre-manipulative cervical spine testing and sustained rotation do not influence intracranial hemodynamics: an observational study with transcranial Doppler ultrasound. J Man Manip Ther 31: 13-23. doi: 10.1080/10669817.2022.2068824
Richter RR, Reinking MF (2005) Evidence in practice. How does evidence on the diagnostic accuracy of the vertebral artery test influence teaching of the test in a professional physical therapist education program? Phys Ther 85: 589-99.
Rivett DA, Sharples KJ, Milburn PD (1999) Effect of premanipulative tests on vertebral artery and internal carotid artery blood flow: a pilot study. J Manipulative Physiol Ther 22: 368-75. doi: 10.1016/s0161-4754(99)70081-3
Sakaguchi M, Kitagawa K, Hougaku H, Hashimoto H, Nagai Y, Yamagami H, Ohtsuki T, Oku N, Hashikawa K, Matsushita K, Matsumoto M, Hori M (2003) Mechanical compression of the extracranial vertebral artery during neck rotation. Neurology 61: 845-7. doi: 10.1212/01.wnl.0000078081.12097.ae
Sarkar J, Wolfe SQ, Ching BH, Kellicut DC (2014) Bow hunter’s syndrome causing vertebrobasilar insufficiency in a young man with neck muscle hypertrophy. Ann Vasc Surg 28: 1032 e1-1032 e10. doi: 10.1016/j.avsg.2013.06.038
Shafafy R, Suresh S, Afolayan JO, Vaccaro AR, Panchmatia JR (2017) Blunt vertebral vascular injury in trauma patients: ATLS((R)) recommendations and review of current evidence. J Spine Surg 3: 217-225. doi: 10.21037/jss.2017.05.10
Shum GL, Cinnamond S, Hough AD, Craven R, Whittingham W (2017) Test-Retest Reliability of Measuring the Vertebral Arterial Blood Flow Velocity in People With Cervicogenic Dizziness. J Manipulative Physiol Ther 40: 255-262. doi: 10.1016/j.jmpt.2017.02.005
Sorensen BF (1978) Bow hunter’s stroke. Neurosurgery 2: 259-61.
Symons BP, Leonard T, Herzog W (2002) Internal forces sustained by the vertebral artery during spinal manipulative therapy. J Manipulative Physiol Ther 25: 504-10. doi: 10.1067/mmt.2002.127076
Takafumi S, Hojo R, Tsuchiyama T, Fukamizu S (2024) A case report of Bow Hunter’s syndrome with intravascular ultrasound showing changing significant severe stenosis of the left vertebral artery associated with turning left. Eur Heart J Case Rep 8: ytad639. doi: 10.1093/ehjcr/ytad639
Thiel H, Rix G (2005) Is it time to stop functional pre-manipulation testing of the cervical spine? Man Ther 10: 154-8. doi: 10.1016/j.math.2004.06.004
Thiel H, Wallace K, Donat J, Yong-Hing K (1994) Effect of various head and neck positions on vertebral artery blood flow. Clin Biomech (Bristol, Avon) 9: 105-10. doi: 10.1016/0268-0033(94)90032-9
Thomas L, Treleaven J (2020) Should we abandon positional testing for vertebrobasilar insufficiency? Musculoskelet Sci Pract 46: 102095. doi: 10.1016/j.msksp.2019.102095
Thomas LC, McLeod LR, Osmotherly PG, Rivett DA (2015) The effect of end-range cervical rotation on vertebral and internal carotid arterial blood flow and cerebral inflow: A sub analysis of an MRI study. Man Ther 20: 475-80. doi: 10.1016/j.math.2014.11.012
Thomas LC, Rivett DA, Attia JR, Parsons M, Levi C (2011) Risk factors and clinical features of craniocervical arterial dissection. Man Ther 16: 351-6. doi: 10.1016/j.math.2010.12.008
Tudose RC, Rusu MC, Hostiuc S (2023) The Vertebral Artery: A Systematic Review and a Meta-Analysis of the Current Literature. Diagnostics (Basel) 13. doi: 10.3390/diagnostics13122036
Vibert D, Rohr-Le Floch J, Gauthier G (1993) Vertigo as manifestation of vertebral artery dissection after chiropractic neck manipulations. ORL J Otorhinolaryngol Relat Spec 55: 140-2. doi: 10.1159/000276405
Weintraub MI, Khoury A (2004) Mechanical compression of the extracranial vertebral artery during neck rotation. Neurology 62: 2143; author reply 2144. doi: 10.1212/wnl.62.11.2143-a
Wuest S, Symons B, Leonard T, Herzog W (2010) Preliminary report: biomechanics of vertebral artery segments C1-C6 during cervical spinal manipulation. J Manipulative Physiol Ther 33: 273-8. doi: 10.1016/j.jmpt.2010.03.007
Xue S, Shi H, Du X, Ma X (2023) Bow Hunter’s syndrome combined with ipsilateral vertebral artery dissection/pseudoaneurysm: case study and literature review. Br J Neurosurg 37: 911-915. doi: 10.1080/02688697.2020.1718604
Yelverton C, Wood JJ, Petersen DL, Peterson C (2020) Changes in Vertebral Artery Blood Flow in Different Head Positions and Post-Cervical Manipulative Therapy. J Manipulative Physiol Ther 43: 144-151. doi: 10.1016/j.jmpt.2019.09.001
Zaidi HA, Albuquerque FC, Chowdhry SA, Zabramski JM, Ducruet AF, Spetzler RF (2014) Diagnosis and management of bow hunter’s syndrome: 15-year experience at barrow neurological institute. World Neurosurg 82: 733-8. doi: 10.1016/j.wneu.2014.02.027
Zaina C, Grant R, Johnson C, Dansie B, Taylor J, Spyropolous P (2003) The effect of cervical rotation on blood flow in the contralateral vertebral artery. Man Ther 8: 103-9. doi: 10.1016/s1356-689x(02)00155-8
![]()