By Marcello Cherchi, MD PhD
For patients
Some kinds of headaches can be treated with “nerve blocks,” which are injections of a numbing medication at different locations in the head. Your doctor will tell you whether these injections may help for the kind of headache that you have. You do not need to do anything special to prepare for these injections. After the injections, you can continue doing most things you usually do, though you will want to avoid using hair-coloring dye for about a day, because that kind of day may irritate the injected skin.
For clinicians
Overview
Nerve blocks using local anesthetics are used in treatment of a variety of headaches, including neuralgic headaches and migraine. The blocks are generally well tolerated.
Introduction
Pain in the head, arising from a variety of causes, has a long history of being treated with injections of local anesthetics in specific areas (Ashkenazi and Levin 2007; Levin 2010). When targeted appropriately, these procedures are safe, well-tolerated and can be effective.
Injection of local anesthetic has several advantages over oral analgesics. First, injections deliver medication in the area from which the pain is arising, and is thus a more focused treatment. Second, since the injected medication is not given systemically (i.e., it is not ingested and does not circulate via the bloodstream throughout the body), the injected mode of delivery avoids many of the side effects that can occur with oral medications.
Nerve blocks are appropriate for certain kinds of headaches, but not for others. Generally, nerve blocks can be applied to a specific nerve that is irritated (a neuralgia), but interestingly, such nerve blockade can also be efficacious in patients with migraine (even though this is a disease of the brain rather than a disease of an individual nerve) (Afridi et al. 2006; Ashkenazi and Young 2005; Young et al. 2008). Blockade of several nerves in the head has also been studied in pregnant women with migraine (Govindappagari et al. 2014), in whom oral medications may not be feasible.
Neuralgias in the head are painful, but not life-threatening. Some patients whose pain is intermittent, mild, or otherwise manageable, may elect simply not to treat it. If a patient has several good (but transient) responses to a pharmacologic nerve block (i.e., injection of a local anesthetic), they may elect to consult an anesthesiologist to undergo radiofrequency nerve ablation (“RFA”).
There is some evidence that nerve blocks can be effective for migraine, (Afridi et al. 2006; Ashkenazi and Young 2005; Young et al. 2008), though many other treatment options are also available for migraine. Many oral medications can be used as migraine prophylactics and migraine abortives. Onabotulinum toxin (Botox®) injections are also used for prophylactic treatment of chronic migraine, though onabotulinum toxin cannot be used simultaneously with the local anesthetic nerve blocks (because those local anesthetics chemically “neutralize” the onabotulinum toxin).
Pharmacology
The drugs injected are local anesthetics. They are injected near nerves that are a few millimeters beneath the surface of the skin, and sometimes embedded within muscle. Below is a table summarizing the characteristics of some of these anesthetics.
|
Drug |
Brand name |
Type |
Potency |
Onset |
Duration |
Pregnancy |
|
Bupivacaine |
Marcaine® |
Amide |
100% |
8-12 minutes |
3.5 (4-8) hours |
Category C |
|
Mepivacaine |
Carbocaine® |
Amide |
25% of bupivacaine |
2-5 minutes |
1.9-3.2 hours |
Category C |
|
Ropivacaine |
Naropin® |
Amide |
60% of bupivacaine |
10-15 minutes |
4.2 (4-6) hours |
Category B |
|
Lidocaine |
Xylocaine® |
Amide |
25% of bupivacaine |
4-8 minutes |
1.5 (1-2) hours |
Category B |
|
Procaine |
Novocaine® |
Ester |
6% – 13% of bupivacaine |
10-20 minutes |
4.2 hours |
Category B |
In the past, steroids of various kinds (e.g., Kenalog®, Depo-medrol®) were sometimes mixed in with the injected anesthetic, based on the rationale that inflammation likely involved the impinged nerve. However, injection of steroids carries the risk of local alopecia (focal hair loss) (Shields et al. 2004).
In the past, epinephrine was sometimes mixed in with the injected anesthetic, based on the rationale that, by constricting blood vessels, the local anesthetic would not be cleared as rapidly and would therefore last longer. However, injection of epinephrine carries the risk of local skin necrosis from focal ischemia.
Technique
|
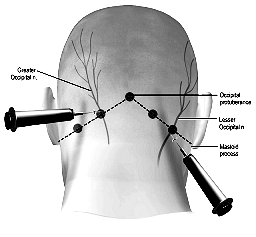
Blockades of the greater occipital nerve, and sometimes also the lesser occipital nerve, both of which arise from the second cervical nerve root, are often employed for occipital neuralgia (Tobin and Flitman 2009; Ward 2003; Young 2010), though has also demonstrated some efficacy in treatment of migraine (Afridi et al. 2006; Ashkenazi and Young 2005; Young et al. 2008). The locations of the nerve blockade injections for the supraorbital and supratrochlear nerves are shown in the adjacent Figure (Levin 2010). |
 |
|
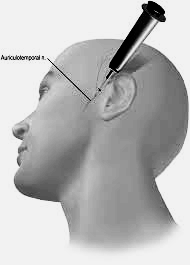
The auriculotemporal nerve arises from the posterior division of the mandibular branch of the trigeminal nerve, which mediates sensation in parts of the temporal region and part of the ear (Komarnitki et al. 2012). Blockade of this nerve can alleviate pain in these areas. The location of the nerve blockade injection is shown in the adjacent Figure (Levin 2010). |
 |
|
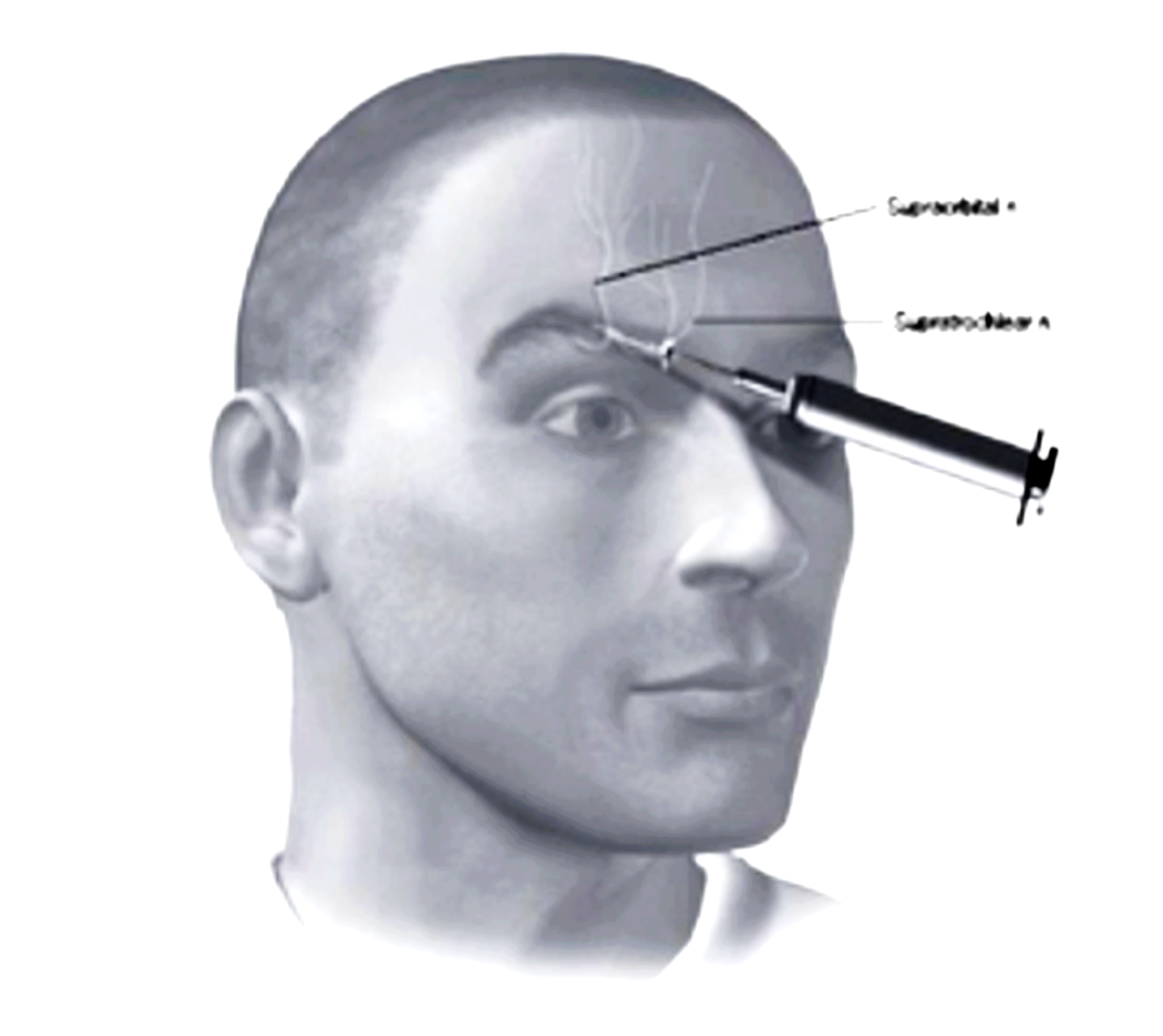
Pain above the eye, in approximately the region of the eyebrow, can be caused by trauma, though also occurs in migraine. Blockade of the supraorbital nerve (which arises from the frontal branch of the ophthalmic division of the trigeminal nerve) can be efficacious in cases of trauma (Sjaastad et al. 1999), and is sometimes efficacious in treatment of migraine (Caputi and Firetto 1997). Blockade of the supratrochlear nerve (which also arises from the frontal branch of the ophthalmic division of the trigeminal nerve) is sometimes also employed. The locations of the nerve blockade injections for the supraorbital and supratrochlear nerves are shown in the adjacent Figure (Levin 2010). |
 |
Adverse effects
Nerve blocks in the head are generally safe and well tolerated. In order to diminish patient discomfort, some practitioners first apply a topical anesthetic (such as EMLA cream) to the sites of the planned injections.
The greatest risk is that the procedure will be unsuccessful – in other words, the injection will fail to relieve the pain in the head.
As with any procedure involving needles, there is always a risk of bleeding and infection. Bleeding is usually controlled simply by applying pressure. The risk of infection is reduced by using sterile procedure and by cleaning the injection site with an alcohol swab; this reduces the risk of infection, though it does not eliminate it completely.
Some patients report mild local pain at the injection site for up to several days after the injection (Young 2010).
Nerve blocks are generally avoided in patients with a history of skull fractures in the vicinity of the injection target area due to the theoretical risk of the injected substance entering the intracranial space (Ward 2003).
Cautions and contraindications
In patients who are not pregnant we generally recommend bupivacaine due to its relative potency and long duration. In patients who are pregnant we generally recommend ropivacaine. Note that all injected local anesthetics are considered safe during nursing.
Relevance in otoneurology
Insofar as nerve blocks may treat migraine, they may have some role in the management of migraine associated vertigo (MAV), though this has not been specifically studied.
Other comments
Nerve blocks for headache may be performed by a neurologist trained in this technique, or at a headache subspecialty clinic, or at a pain clinic.
References
Afridi SK, Shields KG, Bhola R, Goadsby PJ (2006) Greater occipital nerve injection in primary headache syndromes–prolonged effects from a single injection. Pain 122: 126-9. doi: 10.1016/j.pain.2006.01.016
Ashkenazi A, Levin M (2007) Peripheral procedures for headaches. In: Silberstein SD (ed) Wolff’s Headache and Other Head Pain, 8 edn. Oxford University Press
Ashkenazi A, Young WB (2005) The effects of greater occipital nerve block and trigger point injection on brush allodynia and pain in migraine. Headache 45: 350-4. doi: 10.1111/j.1526-4610.2005.05073.x
Caputi CA, Firetto V (1997) Therapeutic blockade of greater occipital and supraorbital nerves in migraine patients. Headache 37: 174-9.
Govindappagari S, Grossman TB, Dayal AK, Grosberg BM, Vollbracht S, Robbins MS (2014) Peripheral nerve blocks in the treatment of migraine in pregnancy. Obstet Gynecol 124: 1169-74. doi: 10.1097/AOG.0000000000000555
Komarnitki I, Andrzejczak-Sobocinska A, Tomczyk J, Deszczynska K, Ciszek B (2012) Clinical anatomy of the auriculotemporal nerve in the area of the infratemporal fossa. Folia Morphol (Warsz) 71: 187-93.
Levin M (2010) Nerve blocks in the treatment of headache. Neurotherapeutics 7: 197-203. doi: 10.1016/j.nurt.2010.03.001
Shields KG, Levy MJ, Goadsby PJ (2004) Alopecia and cutaneous atrophy after greater occipital nerve infiltration with corticosteroid. Neurology 63: 2193-4.
Sjaastad O, Stolt-Nielsen A, Pareja JA, Fredriksen TA, Vincent M (1999) Supraorbital neuralgia. On the clinical manifestations and a possible therapeutic approach. Headache 39: 204-12. doi: 10.1046/j.1526-4610.1999.3903204.x
Tobin J, Flitman S (2009) Occipital nerve blocks: when and what to inject? Headache 49: 1521-33. doi: 10.1111/j.1526-4610.2009.01493.x
Ward JB (2003) Greater occipital nerve block. Semin Neurol 23: 59-62. doi: 10.1055/s-2003-40752
Young W, Cook B, Malik S, Shaw J, Oshinsky M (2008) The first 5 minutes after greater occipital nerve block. Headache 48: 1126-8. doi: 10.1111/j.1526-4610.2008.01146.x
Young WB (2010) Blocking the greater occipital nerve: utility in headache management. Curr Pain Headache Rep 14: 404-8. doi: 10.1007/s11916-010-0130-x
![]()