By Marcello Cherchi, MD PhD
For cases of anterior canal BPPV that are bilateral, or for which the affected side is unknown, reasonable approaches include the maneuver developed by Dr. Darío Andrés Yacovino and colleagues (Yacovino et al. 2009).
Dr. Yacovino’s original paper (Yacovino et al. 2009) described the maneuver as follows:
“Our repositioning maneuver… consists of four steps, with position changes occurring at 30-second intervals. From the head-straight sitting position (position 1), a head-hanging maneuver is performed so that the head is brought to at least 30 degrees below the horizontal… [which is] (position 2). During the maneuver, loose otoconia within the anterior canal should move away from the anterior cupula, triggering a down beating nystagmus… After 30 seconds, once vertigo and nystagmus provoked by the maneuver cease and while still supine, the patient’s head is moved quickly forward ‘chin to chest’ (position 3), with the vertex near the vertical axis. After another 30 seconds have elapsed, head and body are brought into the sitting position (position 4), remaining there for another 30 seconds. In cases of failure or incomplete remission of symptoms, the same maneuver is repeated.”
The Figure below, from the original paper by Yacovino and colleagues (Yacovino et al. 2009), illustrates the positions of this maneuver.
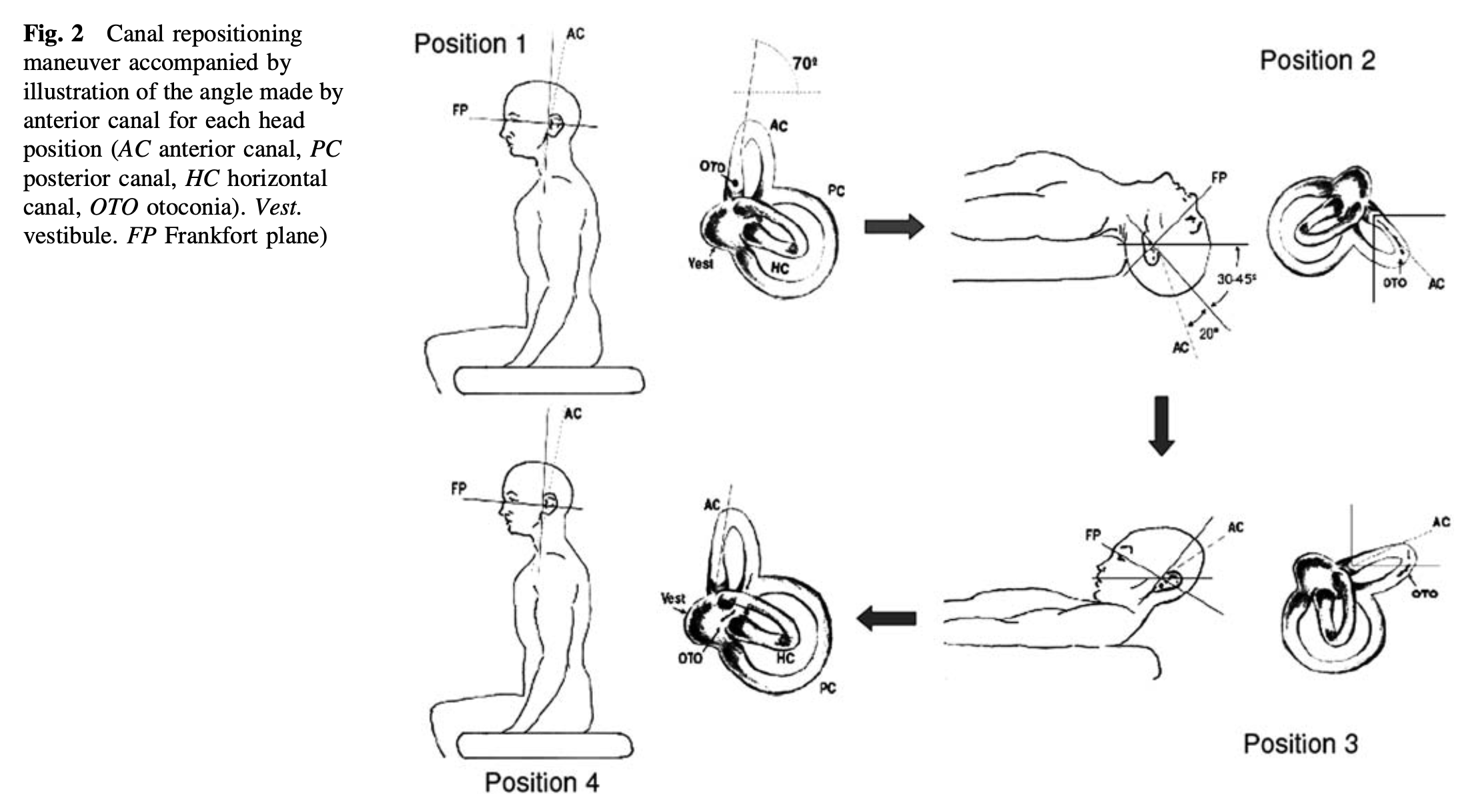
The point at which the patient is lying supine with the neck extended (head hanging off the table) and midline is referred to in some otoneurological literature (Psillas et al. 2007) as the “position of Rose,” named after Dr. Edmund Rose (Bickham 1931; Greene et al. 2003) who first described the utility of this position for certain oral surgeries in 1874 (Rose 1874).
The Yacovino maneuver, used for treating anterior canal BPPV when it is bilateral, or when the affected side is unknown, can be described as follows:
- The patient starts in a seated neutral position.
- The patient lies down, with the trunk supine, and the head/neck midline but extended 30 to 45 degrees below the level of the table. This position is maintained for 30 seconds.
- The head/neck, while still in the midline, is flexed anteriorly (tucking the chin to the chest), raising the head/neck above the level of the table by 30 degrees. This position is maintained for 30 seconds.
- The patient sits up in a neutral position.
Yacovino maneuver, videos
The Yacovino maneuver has been studied in a retrospective review (Yacovino et al. 2009).
One could reasonably ask why a single maneuver such as this would treat anterior semicircular canal BPPV irrespective of the affected side.
In order to understand this, it is necessary first to dispel a pedagogical myth about the anatomy of the semicircular canals. Most textbooks, probably for purposes of perceived didactic clarity, depict the vertical semicircular canals (the posterior and anterior canals) as disposed in an ‘X’-like configuration (when viewing them in an axial plane from above the head), with each canal obliquely oriented 45 degrees off the sagittal and coronal planes. However, it has been very well documented (Blanks et al. 1975) that the reality is more complex. It turns out that the plane of the anterior semicircular canals is angled more closely to the sagittal plane than to the coronal plane, as shown in the Figure below.
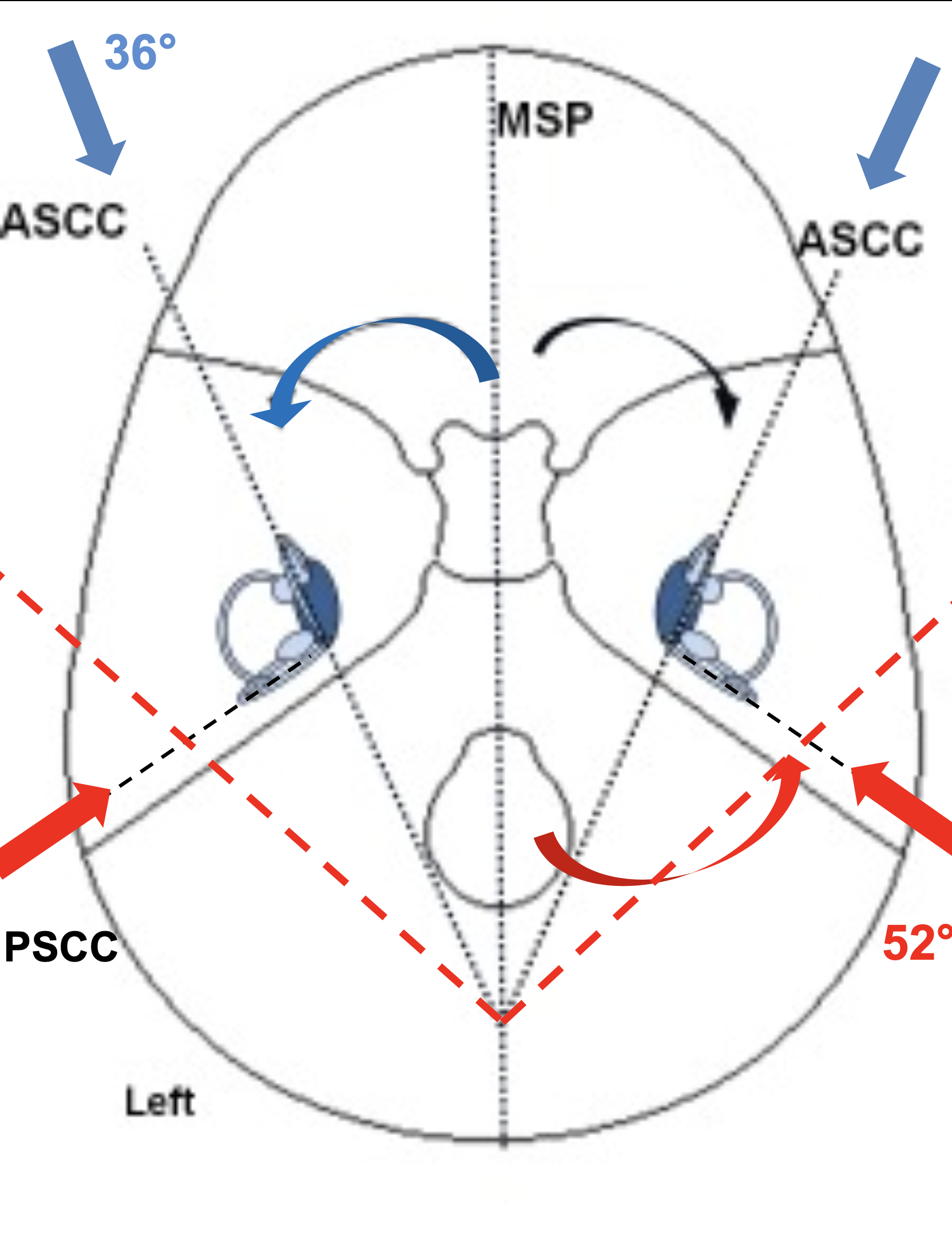
Thus, during treatment with the Yacovino maneuver, when the head remains midline (i.e., turned towards neither the patient’s left nor right), more of the vector of gravitational acceleration will be operating along the sagittal plane (compared to any plane collinear with the inter-aural axis), which will function to coax otoliths around and along the course of the anterior semicircular canal.
References
Bickham WS (1931) Misconception, in America, as to the Rose position. Journal of the American Medical Association 96: 2185-2187. doi: 10.1001/jama.1931.02720520013004
Blanks RH, Curthoys IS, Markham CH (1975) Planar relationships of the semicircular canals in man. Acta Otolaryngol 80: 185-96. doi: 10.3109/00016487509121318
Greene AK, Kreuter M, Mulliken JB (2003) Professor Edmund Rose: his position in surgery. Plast Reconstr Surg 111: 383-6. doi: 10.1097/01.PRS.0000037903.81310.D6
Psillas G, Kekes G, Constantinidis J, Triaridis S, Vital V (2007) Subclavian steal syndrome: neurotological manifestations. Acta Otorhinolaryngol Ital 27: 33-7.
Rose E Vorschlag zur Erleichterung der Operationen am Oberkiefer [Proposal to facilitate operations on the upper jaw] Third Congress of German Surgeons, third session 1874. Langbeck’s Archiv
Yacovino DA, Hain TC, Gualtieri F (2009) New therapeutic maneuver for anterior canal benign paroxysmal positional vertigo. J Neurol 256: 1851-5. doi: 10.1007/s00415-009-5208-1
![]()