By Marcello Cherchi, MD PhD
For patients
In rare cases seizures can manifest with a sensation of disequilibrium (unassociated with other features) that starts abruptly, lasts seconds, and stops abruptly. An electroencephalogram (brain wave test) may show abnormalities compatible with seizures in a specific area. Your doctor may consider checking other tests to check for diseases that could look similar. If symptoms are frequent or otherwise intrusive, then treatment with anti-seizure medication is reasonable.
For clinicians
Overview
Epileptic vertigo refers to symptoms of disequilibrium attributable exclusively to seizure activity in vestibular cortical areas that roughly are mostly situated in the temporal and parietal areas. Some patients with seizures may have disequilibrium as an aura, but this is quickly overshadowed by more dramatic symptoms. It is unusual for seizures to remain restricted to vestibular cortex (and thus only cause disequilibrium), though this does appear to be a discrete clinical entity. For patients whose seizures truly only manifest with disequilibrium, the episodes usually start abruptly, last seconds, and end abruptly. The disequilibrium itself can have a variety of qualities, including rotational movement, translational movement, rocking, floating and unsteadiness. Otovestibular studies such as video head impulse testing and cervical vestibular evoked myogenic potentials are sometimes abnormal in patients with epileptic vertigo, but not in any patterns that are sensitive or specific for this diagnosis. Electroencephalography often shows abnormal activity in the temporoparietal area. Brain MRI should be checked to exclude structural etiologies of seizures. The differential diagnosis includes vestibular paroxysmia. Treatment is with anti-seizure medications; those reported include carbamazepine and phenytoin. If a patient’s symptoms evolve to include symptoms beyond disequilibrium then they should be under the care of a general neurologist or epileptologist.
Introduction
The phrase “epileptic vertigo” refers to symptoms of disequilibrium attributable exclusively to seizure activity in vestibular cortical areas. Synonymous designations in the literature include “vestibular epilepsy,” “vestibular seizures,” etc.
A modest proportion of seizure patients report disequilibrium as part of their seizure prodrome, but their episodes usually evolve to include much more dramatic symptoms (such as generalized tonic-clonic seizures), so the symptom of disequilibrium is likely under-reported. This sequence (prodrome including disequilibrium, followed by more dramatic seizure symptoms) is likely due to the fact that it is unusual for seizure activity to remain restricted to such a small focus (in this case, just so-called vestibular cortex); it is more common for it to spread and cause other sensory, motor and cognitive symptoms that overshadow the symptom of disequilibrium.
For example, Kim and colleagues (Kim, Sunwoo et al. 2016) retrospectively reviewed 831 epilepsy cases and found that 40 patients (4.8%) with a mean age of 32.8 ± 11.8 years “experienced vertigo or dizziness as aura, all of whom had partial seizures.”
Nevertheless, there is some evidence that epileptic vertigo (in which the disequilibrium is an isolated symptom) is a discrete clinical entity, albeit rare.
Anatomy
The areas of the cerebral cortex that mediate vestibular sensations have been imprecisely delineated. Reasonable data on this subject come from studies of intraoperative cortical stimulation, though such studies are limited by the fact that the study subjects were patients had illnesses that warranted craniotomies, rather than healthy individuals.
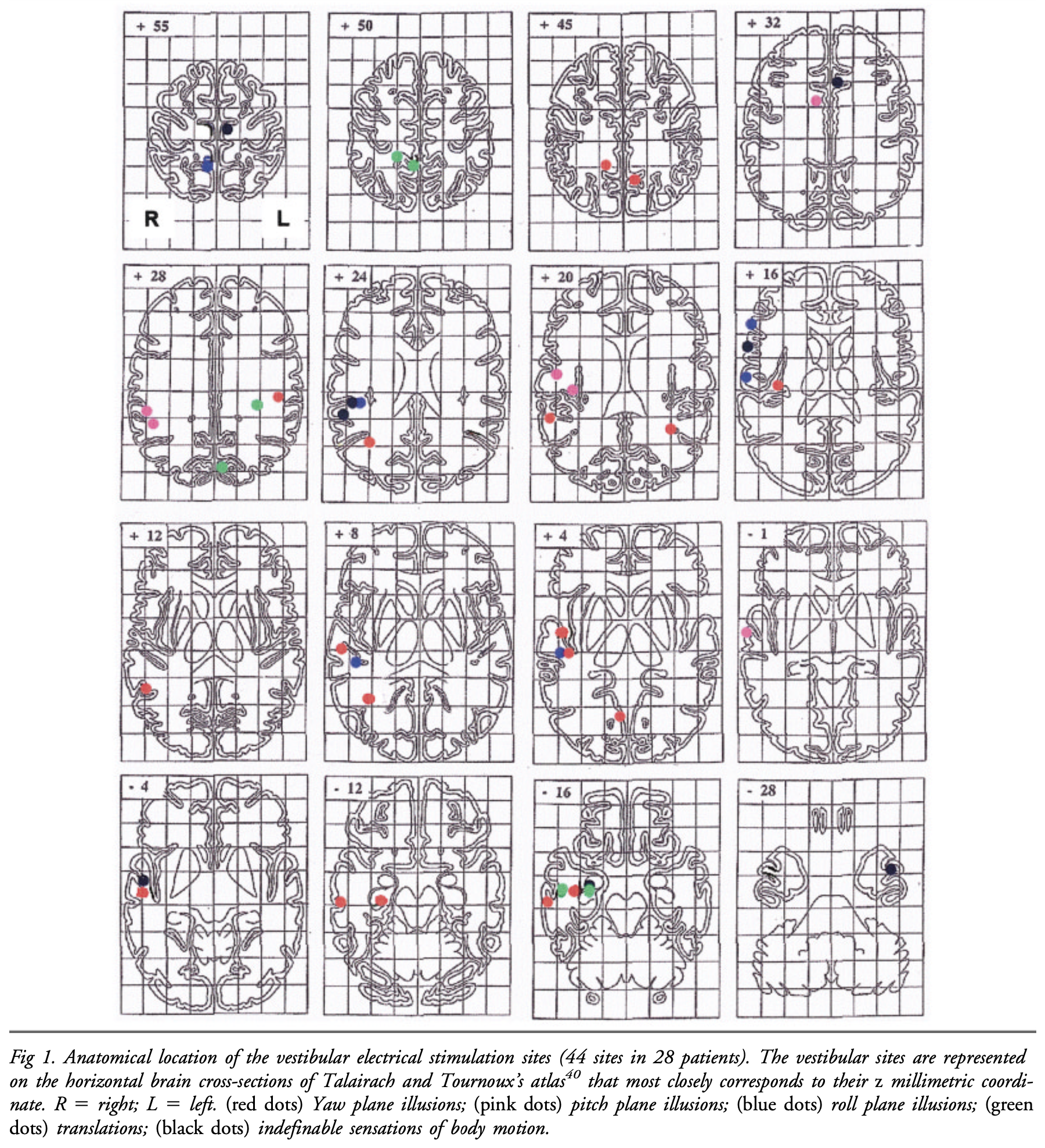
Such a study by Kahane and colleagues (Kahane, Hoffmann et al. 2003), who studied epilepsy patients (prior to surgical treatment of the epilepsy) by implanting surface electrodes and stimulating various areas of the cortex. They stimulated 44 sites in 28 patients. Of the 44 stimulated sites, 19 (43%) were in the temporal lobe, 14 (32%) were in the parietal lobe, 5 (11%) were in the frontal lobe, 2 (5%) were in the occipital lobe and 1 (2%) was in the insular lobe. Some patients had multiple susceptible areas. They designated the area with the highest density of susceptible sites as the “temporo-peri-Sylvian vestibular cortex (TPSVC).”
The Figure below shows the distribution of vetibularly-sensitive sites in the study by Kahane and colleagues (Kahane, Hoffmann et al. 2003).
The Figure below shows a single schematic with a composite of the distribution of vestibularly-sensitive sites in the study by Kahane and colleagues (Kahane, Hoffmann et al. 2003).

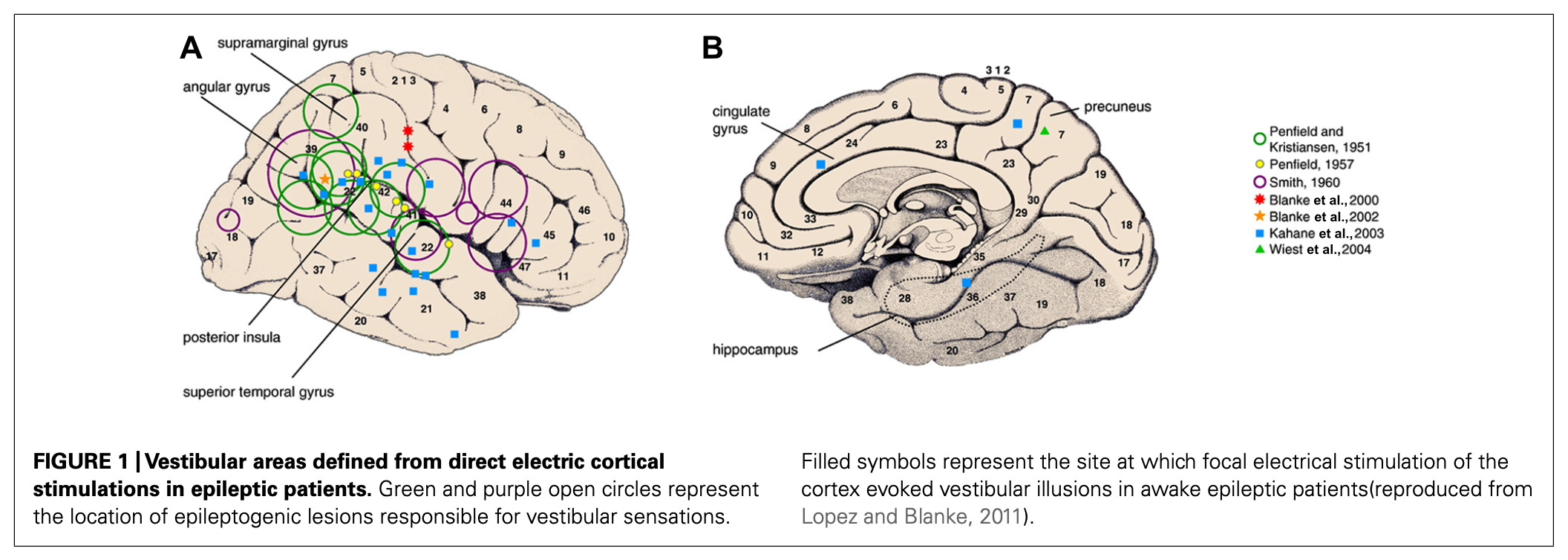
Hewitt and colleagues (Hewett and Bartolomei 2013) point out that, “Partial seizures could also elicit vestibular symptoms by interfering with areas associated with representation of the body in space.” They review multiple studies on localization and summarize them in the Figure below, which shows areas not included in the study by Kahane and colleagues (Kahane, Hoffmann et al. 2003).
Pathophysiological mechanism of disease
Vestibular cortex mediates conscious perception of equilibrium. Seizure in this area should provoke symptoms of disequilibrium.
Clinical presentation
Most case series on epileptic vertigo describe the most common chronology of the symptom of disequilibrium to be one of abrupt onset, brief duration (seconds), and abrupt offset. For example:
- Tarnutzer and colleagues (Tarnutzer, Lee et al. 2015) conducted a systematic literature review of 84 studies (including 11,354 patients) of what they term “epileptic vertigo and dizziness (EVD). They drew a distinction between patients with “isolated EVD” (meaning disequilibrium and no other symptoms) and “non-isolated EVD” (meaning additional symptoms were present). They reported that the duration of episodic vestibular symptoms were “very brief (<30 seconds) in 69.6% of isolated EVD and 6.9% of non-isolated EVD.”
- Similarly, Hewett and colleagues (Hewett and Bartolomei 2013) report that, “The duration of [vestibular] seizures can be variable but is usually brief lasting a few seconds, though there are some patients reporting seizures lasting many minutes. The symptoms are typically paroxysmal beginning suddenly and unless the seizure secondarily generalizes they usually discontinue abruptly.”
- Kogeorgos and colleagues (Kogeorgos, Scott et al. 1981) studied 30 consecutive patients age 15 – 65 years (mean 35 years), of whom 18 (60%) were women, and reported that, “In all 30 patients dizziness occurred in brief episodes, each lasting no more than a few seconds… The symptom usually began abruptly as dizziness or as a feeling of instability that evolved to dizziness or rotational vertigo during several seconds. In the recovery phase nausea was often experienced.”
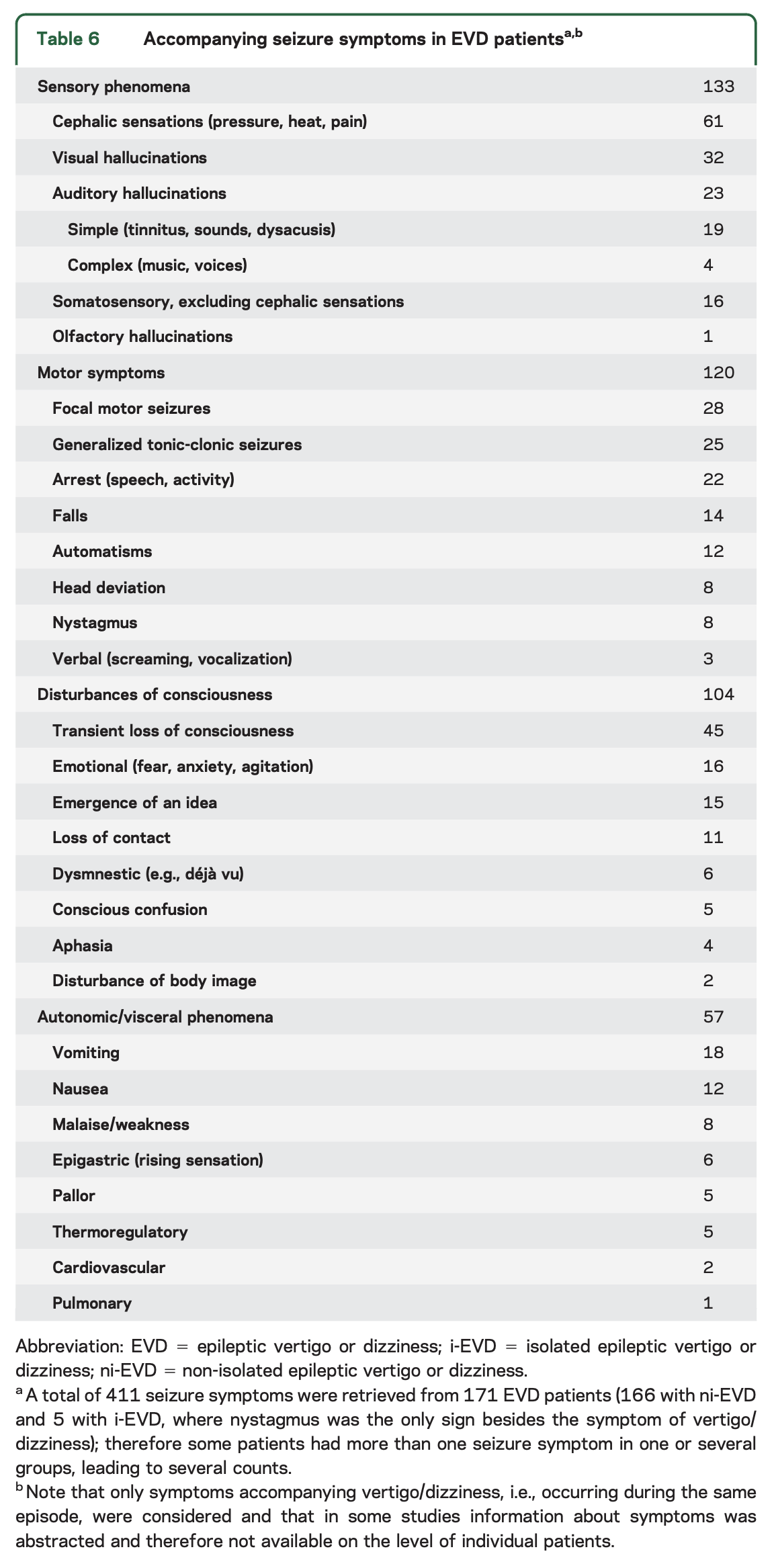
In the systematic literature review by Tarnutzer and colleagues (Tarnutzer, Lee et al. 2015), they collated data from 171 “epileptic vertigo and dizziness (EVD)” patients, of whom 166 had “non-isolated EVD” and 5 had “isolated EVD,” though since “isolated EVD” was supposed to refer to patients whose seizure symptoms were limited to disequilibrium, it is unclear why those 5 patients would have been included in an analysis of symptoms other than disequilibrium. In any case, of these 171 patients, Tarnutzer and colleagues review 411 reported seizure symptoms, and summarized them in the Table below.
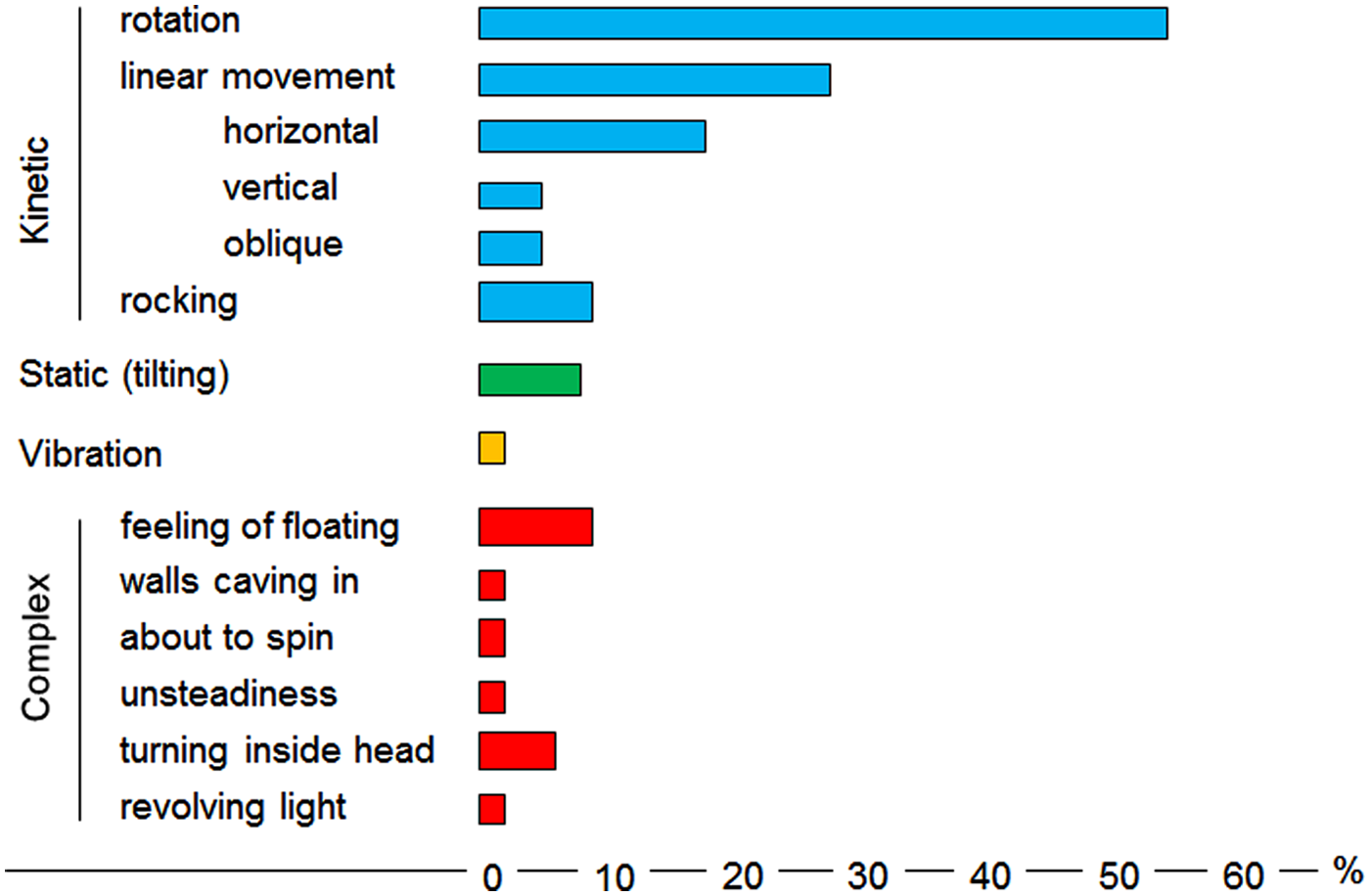
The reported quality of the disequilibrium is variable. The Figure below, which Hewett and colleagues (Hewett and Bartolomei 2013) adapted from Smith (Smith 1960), illustrates the relative frequency of different sensations of disequilibrium described by 120 patients with epileptic vertigo.
Ocular motor examination
Seizures often cause eye movement abnormalities, such as the classic deviation of the eyes contralateral to a unilateral frontal lobe seizure (driven by aberrant activity in the frontal eye field).
It is less common for seizures to cause nystagmus, but this can occur.
Some cortical stimulation studies have found that it is possible to induce actual nystagmus (not simply tonic deviation of the eyes). For example, Blanke and colleagues (Blanke, Perrig et al. 2000) demonstrated that stimulation of an area in the right middle temporal gyrus (MTG) elicited left beat nystagmus, and stimulation of an area in the superior temporal gyrus (STG) elicited rightward, downward and “clockwise” nystagmus. The investigators concluded that, “the finding of a direction-specific nystagmus during electrical stimulation of the STG supports the view that the STG takes part in the processing of vestibular and ocular motor information.”
Testing: vestibular
Very few studies report results of any otovestibular tests in patients diagnosed with epileptic vertigo.
Surmeli and colleagues (Surmeli, Yalcin et al. 2020) studied 9 epileptic vertigo patients with electroencephalography (EEG), video head impulse testing (vHIT) and cervical vestibular evoked myogenic potentials (cVEMP). They reported that, “On vHIT examination, abnormal responses were recorded in five (55.5%), bilateral in three cases and unilateral in two. Similarly, cVEMP revealed no response in five (55.5%), bilateral in two and unilateral in three. In three patients, the side of no response to cVEMP corresponded to the side of epileptiform pathology on EEG. Two patients with bilateral abnormalities on EEG, located in temporal and temporoparietal regions, showed bilateral abnormalities on either cVEMP, or vHIT, or both.”
While these observations are interesting, their value in confirming or refuting a diagnosis of epileptic vertigo is unclear.
Testing: electroencephalography (EEG)
Tarnutzer and colleagues (Tarnutzer, Lee et al. 2015) conducted a systematic literature review of 84 studies (including 11,354 patients) of what they term “epileptic vertigo and dizziness (EVD). They drew a distinction between patients with “isolated EVD” (meaning disequilibrium and no other symptoms) and “non-isolated EVD” (meaning additional symptoms were present). They reported that localized electroencephalography (EEG) abnormalities were mostly temporal (79.8%) rather than parietal (11.8%).
Imaging
Brain MRI without and with contrast should be undertaken to exclude structural etiologies of seizures.
Differential diagnosis
Most episodes of epileptic vertigo start abruptly, last a few seconds, and end abruptly. That clinical history is difficult to differentiate from vestibular paroxysmia. There are two additional factors that make this distinction difficult:
- First, some patients with epileptic vertigo are reported to have otovestibular test result abnormalities, such as on video head impulse testing and cervical vestibular evoked myogenic potentials (Surmeli, Yalcin et al. 2020). Some (though not all) patients with vestibular paroxysmia may have similar findings.
- Second, the treatments (various anti-seizure medications) of these two diseases are similar.
In other words, the history, the results of otovestibular testing, and the response to treatments do not help distinguish epileptic vertigo from vestibular paroxysmia.
At least in theory, electroencephalography (see above) should help distinguish between these two diseases. While the results of EEG may secure the diagnosis, since those results will not change management (i.e., the treatment will be the same), a case can be made for forgoing that study.
Treatment
Treatment with anti-seizure medication is appropriate.
Prognosis
Kogeorgos and colleagues (Kogeorgos, Scott et al. 1981) studied 30 patients with epileptic vertigo and reported that through treatment with phenytoin or carbamazepine:
- In 23/30 (77%) patients without generalized seizures:
- 10 achieved complete remission (mean follow-up 18 months)
- 13 achieved “considerable reduction in the frequency and severity” (mean follow-up two years).
- In 7/30 (33%) of patients whose seizures secondarily generalized:
- 6 “were completely free of both dizziness and other manifestations of epilepsy during one and half to five years of follow-up.”
- 1 patient “with persisting seizures and dizzy episodes did not comply with treatment.”
References
Blanke O, Perrig S, Thut G, Landis T, Seeck M (2000) Simple and complex vestibular responses induced by electrical cortical stimulation of the parietal cortex in humans. J Neurol Neurosurg Psychiatry 69: 553-6. doi: 10.1136/jnnp.69.4.553
Hewett R, Bartolomei F (2013) Epilepsy and the cortical vestibular system: tales of dizziness and recent concepts. Front Integr Neurosci 7: 73. doi: 10.3389/fnint.2013.00073
Kahane P, Hoffmann D, Minotti L, Berthoz A (2003) Reappraisal of the human vestibular cortex by cortical electrical stimulation study. Ann Neurol 54: 615-24. doi: 10.1002/ana.10726
Kim DW, Sunwoo JS, Lee SK (2016) Incidence and localizing value of vertigo and dizziness in patients with epilepsy: Video-EEG monitoring study. Epilepsy Res 126: 102-5. doi: 10.1016/j.eplepsyres.2016.07.002
Kogeorgos J, Scott DF, Swash M (1981) Epileptic dizziness. Br Med J (Clin Res Ed) 282: 687-9. doi: 10.1136/bmj.282.6265.687
Smith BH (1960) Vestibular disturbances in epilepsy. Neurology 10: 465-9. doi: 10.1212/wnl.10.5.465
Surmeli R, Yalcin AD, Surmeli M, Gunay G (2020) Vertiginous epilepsy: documentation of clinical and electrophysiological findings of nine patients. Epileptic Disord 22: 775-781. doi: 10.1684/epd.2020.1232
Tarnutzer AA, Lee SH, Robinson KA, Kaplan PW, Newman-Toker DE (2015) Clinical and electrographic findings in epileptic vertigo and dizziness: a systematic review. Neurology 84: 1595-604. doi: 10.1212/WNL.0000000000001474
![]()