By Marcello Cherchi, MD PhD
For patients
Here are answers to some of the most common questions about cervical vestibular evoked myogenic potentials testing.
| What is this test? | The test of cervical vestibular evoked myogenic potentials (cVEMPs) assesses part of the balance system of the inner ear. |
| What is this test looking for? | This test looks for changes in tone of the sternocleidomastoid muscle in response to sounds. |
| Is this test experimental or investigational? | This test is approved by the Food and Drug Administration. It is neither experimental nor investigational. |
| What happens during this test? | During this test the audiologist or technician usually has you lie down on an examination table. They place an earbud insert earphone in your ear and apply electrodes on your face, neck and chest. You raise your head off the table and hear a series of loud tones. This is performed once in each ear. |
| Is this test uncomfortable? | The test is not uncomfortable. |
| How long does this test take? | The test takes about 30 minutes. |
| Do I have to prepare for this test? | If you have ear wax, this should be removed before the test. There are otherwise no specific preparations for this test. |
| Are there any special instructions for what to do after the test? | There are no special instructions for what to do after this test. |
For clinicians
Overview
Cervical vestibular evoked myogenic potentials (cVEMPs) are reflex myogenic potentials usually elicited by vibration-induced stimulation of the saccule. The myogenic response is measured from the tonically contracted sternocleidomastoid ipsilateral to the acoustic stimulus. The test assesses the pathway from the saccule, through the inferior division of the vestibular nerve, to the vestibular nucleus, through the medial and lateral vestibulospinal tracts to the sternocleidomastoid. It is reasonable to check cVEMPs in some patients with the symptom of disequilibrium, and some patients with certain auditory symptoms (such as hyperacusis, pulsatile tinnitus, or autophony).
Introduction
Cervical vestibular evoked myogenic potentials (cVEMPs) are a reflex change in muscle tone of the sternocleidomastoid in response to a vestibular signal arising from acoustic stimulation (less commonly from bone vibration stimulus) of the saccule.
The cVEMP is one of several types of vestibular evoked myogenic potential responses.
Physiology and neuroanatomy
The cVEMP response is thought to originate in the saccule. The saccule is one of the two otolith organs in each labyrinth, as shown in the Figure below.
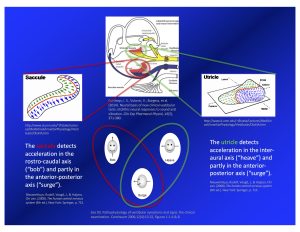
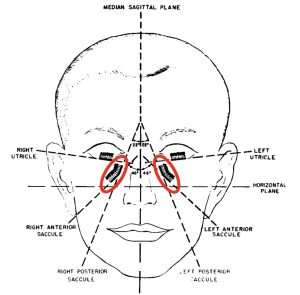
The dispositions of the saccules in the skull is depicted in the Figure below, from Miller (Miller 1962).
The saccule detects linear acceleration primarily along the rostro-caudal axis (“bob”), and less along the anterior-posterior axis (“surge”). Stimulation of the saccule elicits several responses, including the following oligosynaptic pathway:
- First-order neuron
- Receptor in the saccule
- Cell body resides in the vestibular (Scarpa’s) ganglion
- Projects axons through the inferior division of the vestibular nerve
- Synapses in the lateral vestibular nucleus
- Second-order neuron
- Cell body resides in the lateral vestibular nucleus
- Some second-order neurons project through the lateral vestibulospinal tract
- Other second-order neurons project through the ipsilateral (more than contralateral) medial vestibulospinal tract
- These projections synapse on the ipsilateral (more than contralateral) anterior horn cell
- Cell body resides in the lateral vestibular nucleus
- Third-order neuron
- Cell body resides in the internuncial neuron and/or alpha motor neuron
- Projects to the sternocleidomastoid and synapses at the neuromuscular junction
This pathway is schematically depicted in the Figure below, from Fife and colleagues (Fife et al. 2017).
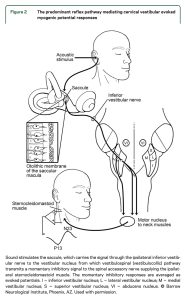
A lesion anywhere along this pathway may affect cVEMP responses.
Equipment needed
Depending on the clinical scenario, the stimulus generator can be acoustic (through earbud insert earphones) or vibratory (from a bone vibrator). When feasible it is desirable to use an acoustic stimulus because it is easier to stimulate one ear at a time. Using a bone vibrator is more likely to deliver a vibratory stimulus to both labyrinths.
The equipment for measuring myogenic responses from surface electrodes is similar to other evoked myogenic potential machines. The software is customized to the timing, amplitude and response-averaging parameters relevant for cVEMPs.
How to perform the test
If the cVEMP is to be performed using acoustic stimuli, then make sure there is no occlusion of the external auditory canal (such as from cerumen), and make sure that there is no conductive hearing loss.
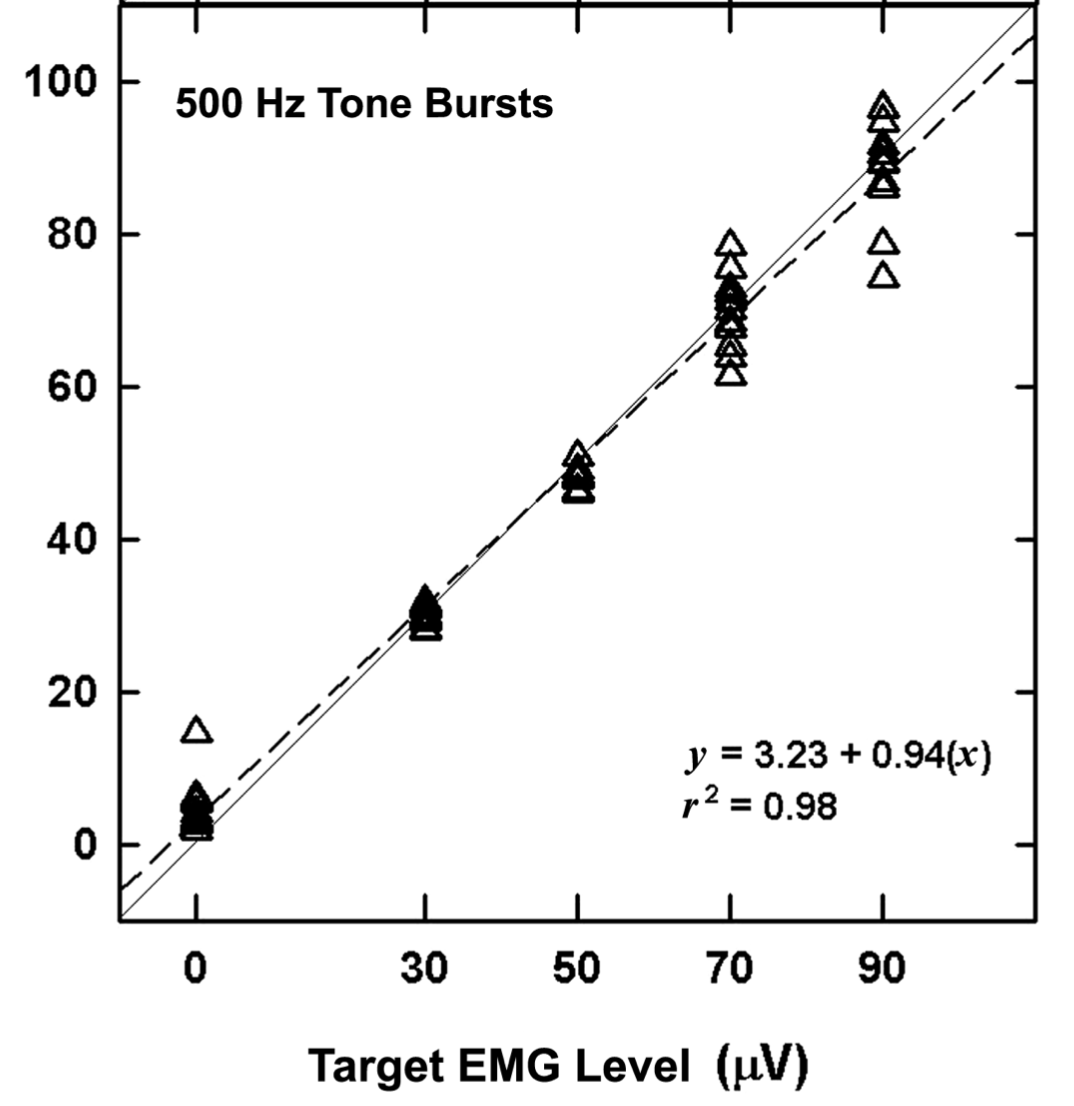
Vestibular evoked myogenic potentials measured from the neck or limbs require that the muscle be tonically activated. This is because the amplitude of the response partially depends on the baseline level of tonic muscle activation, as shown in the Figure below from Murnane and colleagues (Akin et al. 2004).
For the sternocleidomastoid this can be accomplished in two ways.
Initially the most common practice was to have the patient turn the head (sometimes against force) to one side, which activates the contralateral sternocleidomastoid, as shown in the Figure below from Kumar and colleagues (Kumar et al. 2022). A disadvantage of this approach is that it is difficult to ensure that the patient exerts equal force on each side.

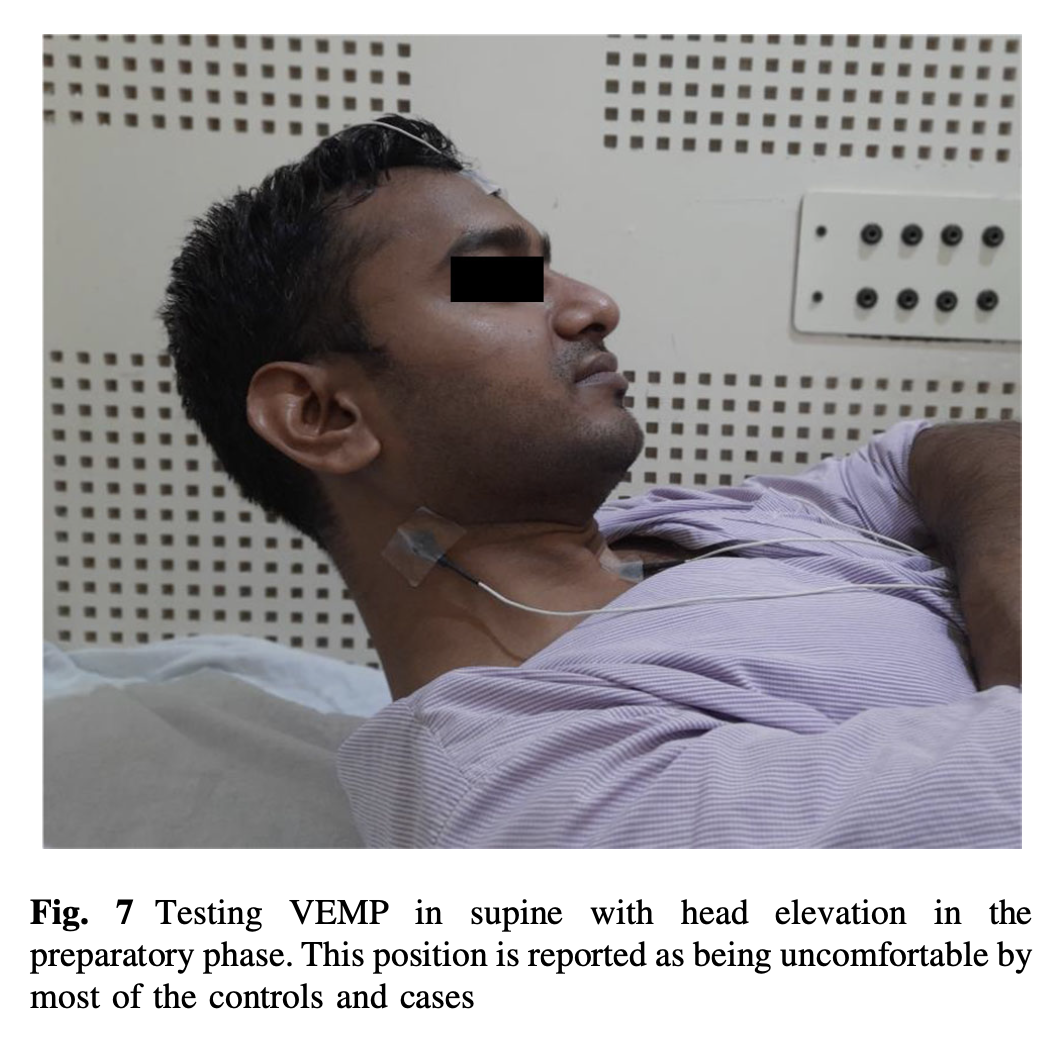
Another approach is to have the patient lie supine, and instruct them to elevate the head off the bed, as shown in the Figure below from Kumar and colleagues (Kumar et al. 2022). We favor this approach because it activates the sternocleidomastoids equally. However, one disadvantage is that some patients tire more easily with this method.
The acoustic stimulus (which can be either a tone burst or a click) is generated by a for-purpose stimulator. The most common protocol is to use a tone burst of 500 Hz at 95 dB. The myogenic potentials are collected from repeated cycles and response averaging is performed.
If thresholds are being tested, then cVEMPs may be performed multiple times with stimuli of different amplitudes.
The usual montage for cVEMP is (Dlugaiczyk 2020):
- Active electrode is placed on the middle of the belly of the sternocleidomastoid.
- Reference electrode is placed at the sternoclavicular junction.
- Ground electrode is placed on the forehead.
What this test assesses
Cervical vestibular evoked myogenic potentials (cVEMPs) assess the integrity of the neuroanatomical pathway described above from the saccule to the sternocleidomastoid, and is sensitive to lesions anywhere along that pathway.
How to interpret the test results
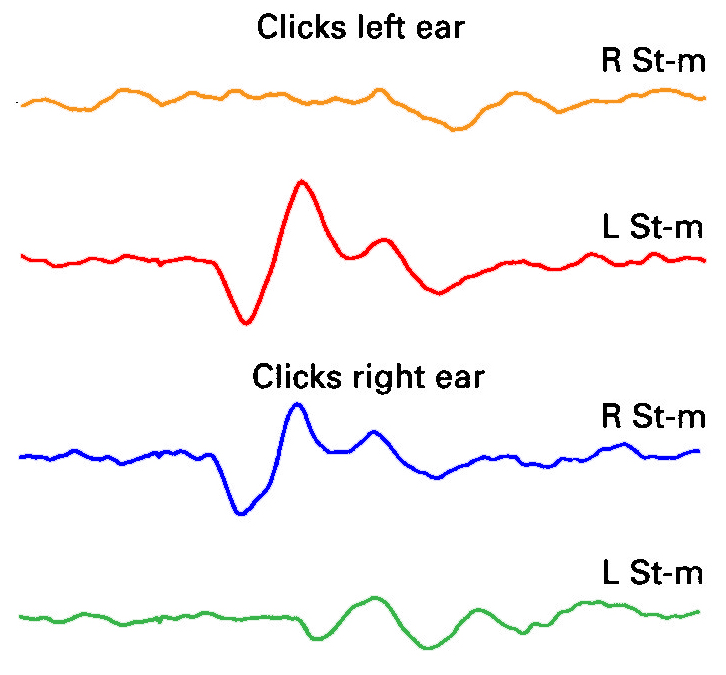
Cervical vestibular evoked myogenic potentials are usually clearer and more robust ipsilateral to the stimulated ear, whereas they are usually absent or much smaller contralaterally. This is shown in the Figure below, adapted from Colebatch and colleagues (Colebatch et al. 1994).
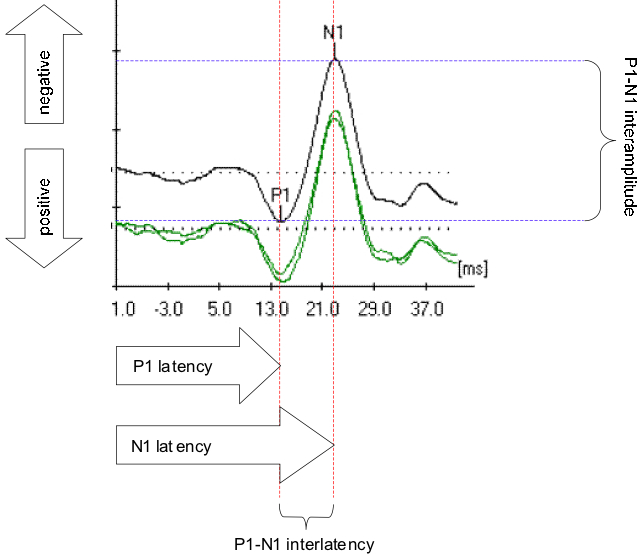
A normal cVEMP waveform is shown in the Figure below. There is an expected latency for each wave (p13, n23). Normative ranges for the inter-peak amplitude have been debated (Basta et al. 2005; Bi et al. 2016; Janky and Shepard 2009; Kumar et al. 2022), and are likely different for children (Kelsch et al. 2006).
Clinically we find the asymmetry between the two ears to be more informative than the absolute amplitudes.
The effect of age on cVEMP responses
Age has been shown to affect cVEMP responses.
- Janky and Shepard studied cVEMP responses and reported that advancing age positively correlates with thresholds and negatively correlates with amplitudes, and does not correlate with latencies (Janky and Shepard 2009).
- Su and colleagues studied cVEMP responses and reported that advancing age positively correlates with latency, negatively correlates with amplitude, and negatively correlates with response rates overall (Su et al. 2004).
- Ochi and Ohashi studied cVEMPs and reported that advancing age positively correlates with thresholds and negatively correlates with amplitudes (Ochi and Ohashi 2003).
- Maes and colleagues studied cVEMPs and reported that advancing age positively correlates with thresholds, negatively correlates with amplitudes, and negatively correlates with latencies (Maes et al. 2010).
- Agrawal and colleagues studied cVEMPs and reported that advancing age negatively correlates with amplitudes (Agrawal et al. 2012).
- Welgampola and Colebatch studied cVEMPs and reported that advancing age positively correlates with thresholds and negatively correlates with amplitudes (Welgampola and Colebatch 2001).
In summary, there is evidence that advancing age causes an increase in latencies, an increase in thresholds, a decrease in amplitude and a decrease in overall cVEMP responses. Thus, in an older individual, symmetrically absent cVEMPs are generally not diagnostically meaningful.
Limitations
Vestibular evoked myogenic potentials that use acoustic stimuli rely on the integrity of the middle ear to transmit the vibrations from sound to the labyrinth. Thus, conductive hearing loss can interfere with cVEMP results. For this reason it is desirable to have a recent audiogram when performing and interpreting acoustically-elicited cVEMPs. In patients with conductive hearing loss, the audiologist or technician may switch to using a bone vibrator for the stimulus.
Some patients with limited cervical range of motion, or with neck weakness, may be unable to perform cVEMPs.
Contraindications
Acoustically-elicited VEMPs generally use earbud insert earphones, which is relatively contraindicated in patients with external ear problems such as otitis externa or recent injury.
Pitfalls
Keep in mind that non-vestibular lesions can result in abnormal VEMPs. For example, a patient with hemiparesis may have a weakened sternocleidomastoid (and thus a weak or absent cervical VEMP) even though the peripheral vestibular system is intact.
When evaluating an asymmetry in cervical vestibular evoked myogenic potentials, keep in mind that the side with the smaller response may be too weak, or the side with the larger response may be too strong.
- In most cases, the side with pathology will be the that with the smaller amplitude cVEMP.
- However, there are some cases in which the side with the pathology will be that with the larger amplitude cVEMP. This usually occurs in third window phenomena such as semicircular canal dehiscence (SCD). In the case of SCD, there may also be low cVEMP thresholds, and audiometry may show conductive hyperacusis.
The earbud insert earphones can burn out. Improperly cleaned skin beneath electrodes can lead to high electrical impedance and interfere with measurement of myogenic responses. There is sometimes artifact from electrical interference.
When is the test indicated
Cervical vestibular evoked myogenic potentials comprise a reasonable tool for testing saccular pathways in patients with the symptom of disequilibrium. It may also be helpful in evaluating patients with certain auditory symptoms (such as hyperacusis, pulsatile tinnitus or autophony).
Diseases that may be diagnosed by this test
Diseases of the labyrinth and vestibular nerve are sometimes diagnosable if they involve saccular pathways.
Some lesions causing vestibular weakness may be detectable on cVEMPs if there is involvement of the saccule or its afferents through the vestibular nerve.
Third window phenomena, such as semicircular canal dehiscence, can manifest with abnormally large-amplitude cervical vestibular evoked myogenic potentials ipsilateral to the stimulated ear. Confidence in the diagnosis increases if there are ipsilaterally low cVEMP thresholds, and if audiometry shows ipsilateral conductive hyperacusis.
References
Agrawal Y, Zuniga MG, Davalos-Bichara M, Schubert MC, Walston JD, Hughes J, Carey JP (2012) Decline in semicircular canal and otolith function with age. Otol Neurotol 33: 832-9. doi: 10.1097/MAO.0b013e3182545061
Akin FW, Murnane OD, Panus PC, Caruthers SK, Wilkinson AE, Proffitt TM (2004) The influence of voluntary tonic EMG level on the vestibular-evoked myogenic potential. J Rehabil Res Dev 41: 473-480. doi: PMID: 15543465
Basta D, Todt I, Ernst A (2005) Normative data for P1/N1-latencies of vestibular evoked myogenic potentials induced by air- or bone-conducted tone bursts. Clin Neurophysiol 116: 2216-2219. doi: PMID: 16043396
Bi X, Zhou HF, Su J, Zhang J, Wang MX (2016) [The normative values of vestibular evoked myogenic potential in different age-groups]. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 30: 1016-1020. doi: 10.13201/j.issn.1001-1781.2016.13.003
Colebatch JG, Halmagyi GM, Skuse NF (1994) Myogenic potentials generated by a click-evoked vestibulocollic reflex. J Neurol Neurosurg Psychiatry 57: 190-197.
Dlugaiczyk J (2020) Evidence-based diagnostic use of VEMPs (Evidenzbasierte VEMP-Diagnostik): From neurophysiological principles to clinical application (Von den neurophysiologischen Grundlagen zur klinischen Anwendung). HNO. doi: 10.1007/s00106-019-00767-2
Fife TD, Colebatch JG, Kerber KA, Brantberg K, Strupp M, Lee H, Walker MF, Ashman E, Fletcher J, Callaghan B, Gloss DS, 2nd (2017) Practice guideline: Cervical and ocular vestibular evoked myogenic potential testing: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. Neurology 89: 2288-2296. doi: 10.1212/WNL.0000000000004690
Janky KL, Shepard N (2009) Vestibular evoked myogenic potential (VEMP) testing: normative threshold response curves and effects of age. J Am Acad Audiol 20: 514-22. doi: 10.3766/jaaa.20.8.6
Jongkees LB, Maas JP, Philipszoon AJ (1962) Clinical nystagmography. A detailed study of electro-nystagmography in 341 patients with vertigo. Pract Otorhinolaryngol (Basel) 24: 65-93.
Kelsch TA, Schaefer LA, Esquivel CR (2006) Vestibular evoked myogenic potentials in young children: test parameters and normative data. Laryngoscope 116: 895-900. doi: PMID: 16735887
Kumar L, Kairo A, Thakar A (2022) Normative and Pathological Ranges of Cervical Vestibular Evoked Myogenic Potentials in Normal Subjects and Patients with Complete Compensated Unilateral Vestibular Loss: A Cross Sectional Study. Indian Journal of Otolaryngology and Head & Neck Surgery 74: 4020-4027. doi: 10.1007/s12070-021-02723-5
Maes L, Dhooge I, D’Haenens W, Bockstael A, Keppler H, Philips B, Swinnen F, Vinck BM (2010) The effect of age on the sinusoidal harmonic acceleration test, pseudorandom rotation test, velocity step test, caloric test, and vestibular-evoked myogenic potential test. Ear Hear 31: 84-94. doi: 10.1097/AUD.0b013e3181b9640e
Miller EF, 2nd (1962) Counterrolling of the human eyes produced by head tilt with respect to gravity. Acta Otolaryngol 54: 479-501.
Ochi K, Ohashi T (2003) Age-related changes in the vestibular-evoked myogenic potentials. Otolaryngol Head Neck Surg 129: 655-659. doi: 10.1016/s0194-5998(03)01578-x
Su HC, Huang TW, Young YH, Cheng PW (2004) Aging effect on vestibular evoked myogenic potential. Otol Neurotol 25: 977-980. doi: 10.1097/00129492-200411000-00019
Welgampola MS, Colebatch JG (2001) Vestibulocollic reflexes: normal values and the effect of age. Clin Neurophysiol 112: 1971-9.
![]()