By Marcello Cherchi, MD PhD
For clinicians
Overview
Third window phenomena result when there is an abnormal (or abnormally large) connection between the labyrinth and some other space. Such abnormal connections can be congenital or acquired. A third window reduces the hydraulic resistance in the labyrinth, making it easier for fluid waves propagating through the labyrinth to stimulate cochlear and vestibular hair cells. This leads to clinical manifestations such as hyperacusis, sound/vibration-induced oscillopsia, nystagmus and disequilibrium. True third window phenomena include semicircular canal dehiscence, carotid dehiscence and temporal bone fracture involving the labyrinth; other conditions that reduce the labyrinth’s hydraulic resistance include large vestibular aqueduct and large cochlear aqueduct. These conditions can often be diagnosed on temporal bone CT. Treatment is surgical.
Introduction
Third window phenomena (Ota, Sakagami et al. 2021) are abnormal (or abnormally large) connections between the labyrinth and some other space. Some of these may be congenital, while others are usually acquired. A third window changes hydraulic resistance in the labyrinth, and may alter which hair cells get stimulated by vibration and sound. Symptoms often include abnormal auditory perceptions (such as hyperacusis), and sound/vibration-induced oscillopsia, nystagmus and disequilibrium. Management is surgical.
Anatomy and normal physiology
The bony labyrinth is a convoluted space embedded within the temporal bone. A very small amount of fluid can pass very slowly in or out of the labyrinth via various channels (cochlear aqueduct, endolymphatic duct, vestibular aqueduct), but otherwise the total amount of perilymphatic and endolymphatic fluid remains approximately constant. This fluid is effectively incompressible. There round window and the oval window are two “holes,” each covered with a thin membrane; these comprise an interface between the inner ear and the middle ear.
As sound enters the external auditory canal, the oscillating pressure waves get transduced into the kinetic energy of the eardrum moving inwards and outwards, and this motion is transmitted through the ossicular chain. At the end of the ossicular chain, the stapes footplate is attached to the membrane covering the oval window. As sounds make the eardrum vibrate, the stapes footplate will push the membrane of the oval window inwards and outwards in a piston-like motion. Because endolymphatic and perilymphatic fluid is incompressible, any inward movement of the membrane at the round window will move fluid of a certain volume, and that volume must be exactly offset by outward motion somewhere else, which is usually the round window. The alternating inward and outward motion of the membrane of the oval window, and the corresponding alternating outward and inward motion of the membrane of the round window, create fluid waves that stimulate hair cells in the cochlea that in turn transduce the movement into electrochemical signals that generate action potentials resulting in neural signaling through the cochlear nerve, which we eventually perceive as sound.
Pathology and pathophysiology
The arrangement described above works when there are two “windows” (the oval window and the round window). If a “third window” were to appear somewhere in the labyrinth, there would be two consequences (Iversen and Rabbitt 2020).
First, the presence of the third window would lower the total resistance (in the hydrodynamic sense) of the system. The result is that stimulation of inner ear hair cells would be “easier” — which is to say that it would require less input (kinetic energy) to generate the same stimulation of hair cells.
Second, depending on where the third window is placed, it could result in stimulation of different hair cells — specifically, vestibular hair cells (Iversen, Zhu et al. 2018).
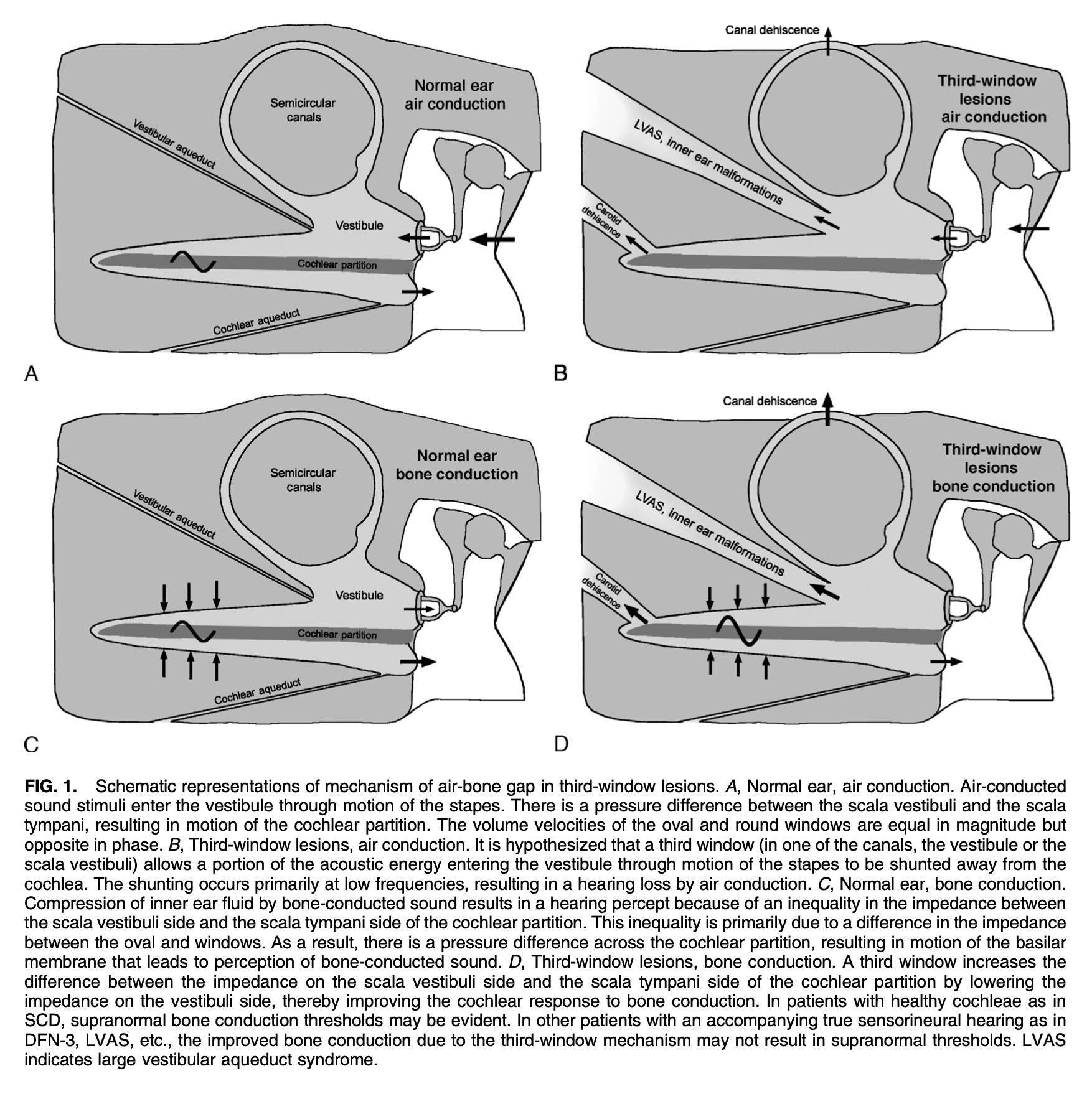
The Figure below, from Merchant and Rosowski (Merchant and Rosowski 2008), schematically depicts the effects of third window phenomena with air conducted and bone conducted stimuli.
In principle a third window can be created anywhere in the labyrinth. The main ones are:
- Dehiscence of any of the three semicircular canals
- Carotid dehiscence
- Temporal bone fracture involving the labyrinth
The following phenomena are not “third windows,” but are abnormally large passages into the labyrinth which (like third window phenomena) reduce the hydraulic resistance in the labyrinth:
Generally, a third window can manifest with clinical correlates of the two consequences described earlier.
First, less energy is required to stimulate inner ear hair cells; clinically this can manifest with overly sensitive hearing (and conductive hyperacusis on audiometry).
Second, depending on the location of the third window, the path of the fluid waves (generated by sound or vibration) may traverse a region with vestibular hair cells, resulting in some combination of Tullio’s phenomenon (sounds cause oscillopsia and disequilibrium) and nystagmus.
Some third window phenomena may be congenital (such as an enlarged vestibular aqueduct), while others may be acquired (such as semicircular canal dehiscence).
Diagnostic imaging
Depending on the type of third window phenomenon in question, imaging (such as with temporal bone CT) may be confirmatory.
Management
If symptoms from a third window phenomenon are sufficiently intrusive or limiting function, then surgical repair may be contemplated.
References
Iversen MM, Zhu H, Zhou W, Della Santina CC, Carey JP, Rabbitt RD (2018) Sound abnormally stimulates the vestibular system in canal dehiscence syndrome by generating pathological fluid-mechanical waves. Sci Rep 8: 10257. doi: 10.1038/s41598-018-28592-7
Merchant SN, Rosowski JJ (2008) Conductive hearing loss caused by third-window lesions of the inner ear. Otol Neurotol 29: 282-9. doi: 10.1097/mao.0b013e318161ab24
Ota I, Sakagami M, Kitahara T (2021) The Third Mobile Window Effects in Otology/Neurotology. J Int Adv Otol 17: 156-161. doi: 10.5152/JIAO.2021.8632
![]()