By Marcello Cherchi, MD PhD
For patients
Large vestibular aqueduct (LVA) is a genetically mediated inner ear developmental anomaly. It usually presents in childhood with hearing loss, typically starting on one side. Some patients also experience disequilibrium. The clinical course is quite variable, though the hearing loss tends to be progressive, and there are often abrupt, “stepwise” deteriorations in hearing. Workup may include hearing tests, vestibular tests, imaging studies and genetic testing. The hearing loss is sometimes treated with cochlear implantation. Patients with LVA are usually managed by an otolaryngologist.
For clinicians
Overview
Large vestibular aqueduct (LVA) is a genetically mediated developmental disorder in which the vestibular aqueduct is larger than normal. Some epidemiological studies report a slight female preponderance. Cases can be unilateral or bilateral. The pathophysiology remains poorly understood. Hearing loss is the most common presenting symptoms; most cases present with hearing loss on the same side as the large vestibular aqueduct; in many cases the contralateral (radiographically normal) ear eventually also loses hearing. The hearing loss often presents in childhood, and some case reports describe it as precipitated by minor head trauma. The hearing loss is progressive, often in a step-wise fashion. Vestibular symptoms are less common, though the reported incidence is broad (2 – 71%). Physical examination may show conductive hearing loss on Rinne’s test. Ocular motor examination may show nystagmus that is non-localizing. Audiologic testing usually shows mixed hearing loss, worse in the high frequencies. Tympanometry may show an abnormally low resonance frequency. A variety of vestibular test result abnormalities may be found, including: caloric weakness; VEMPs that are absent or unusually large or with unusually low thresholds; an elevated SP/AP ratio on electrocochleography. Interestingly, the correlation between abnormal vestibular test results and the presence of vestibular symptoms is often poor. Most cases of LVA are attributable to one of hundreds of mutations in the SLC26A4 gene, though mutations in other genes (CEVA, FOXi1, GJB2, KCNJ10, POU3F4) have been reported. High resolution temporal bone CT remains the study of choice; MRI may provide complementary information. The clinical course is extremely variable, though the overall trajectory tends to be one of deteriorating hearing. Some patients eventually choose to undergo cochlear implantation. Other treatment modalities (dietary sodium restriction; steroids) have not been well-studied. If LVA is suspected, then referral to otolaryngology is appropriate.
Introduction
The phrases “large vestibular aqueduct” (LVA) and “enlarged vestibular aqueduct” (EVA) are used interchangeably in the literature, sometimes appended with the word “syndrome” (LVAS, EVAS).
The term “enlarged” implies (incorrectly) that the vestibular aqueduct used to be appropriately small, and subsequently became inappropriately large. In fact, embryologically the vestibular aqueduct begins as large, and during development it becomes smaller; so really this abnormality results from the vestibular aqueduct’s “developmental failure to become smaller,” thus a more correct term might be, “unshrunken vestibular aqueduct,” but nobody says that.
For this reason we prefer the more neutral term, “large vestibular aqueduct” (LVA).
Epidemiology
An epidemiological survey conducted in Japan reported that of all patients diagnosed with LVA, 58.2% were female (Noguchi, Fukuda et al. 2017), suggesting female preponderance. Interestingly, although females with LVA tend to have larger vestibular aqueducts than males, their hearing loss on average is not worse (Ruthberg, Ascha et al. 2019).
LVA is typically present unilaterally, but bilateral cases are not rare (Subramaniam, Tan et al. 2012, Zhang, Chen et al. 2020, Nakano, Arimoto et al. 2022). An epidemiological study conducted in Japan surprisingly reported that EVA was bilateral in 91.1% of patients (Noguchi, Fukuda et al. 2017).
Pathophysiology
The pathophysiology of LVA remains poorly understood. Several studies suggest that it belongs to the class of “third-window phenomena” (Sheykholeslami, Schmerber et al. 2004, Mimura, Sato et al. 2005, Zhou and Gopen 2011, Seo, Kim et al. 2016, Riggs, Hiss et al. 2020). Biomechanical analyses have been suggested in modeling LVA (Han, Wang et al. 2020).
Presentation: auditory
The most common presentation of LVA is hearing loss, usually (initially) unilateral. An epidemiological survey conducted in Japan reported that 341/380 (89.7%) reported hearing loss as the initial symptom (Noguchi, Fukuda et al. 2017).
Of cases that are unilateral, the hearing loss may remain limited to the side with radiographic LVA (Macielak, Mattingly et al. 2019). However, it is also well-reported that patients with unilateral hearing loss ipsilateral to radiographic LVA eventually develop hearing loss in the contralateral (radiographically normal) ear (Greinwald, DeAlarcon et al. 2013, van Beeck Calkoen, Pennings et al. 2021).
Presentation: vestibular
Studies cite a broad range of the prevalence of vestibular symptoms in LVA patients. For example, an epidemiological survey conducted in Japan reported that 34/380 (8.9%) of patients with LVA listed “vertigo/dizziness/imbalance” as the initial symptom (Noguchi, Fukuda et al. 2017), compared to 89.7% that presented with hearing loss. A series of 27 children (age 3 – 12 years) reported that 6 (22%) complained of “vertigo” (Yang, Lavender et al. 2016). A series of 28 children with bilateral LVA reported that 11 (39%) suffered from vertigo attacks (Nakano, Arimoto et al. 2022). A retrospective chart review of 11 adult and 21 pediatric patients documented the incidence of vestibular symptoms to be 46% in adults and 48% in children (Grimmer and Hedlund 2007). A series of 22 patients with a median age of 8 years (range 6 months – 35 years) reported that 14 (64%) complained of “dizziness” (Song, Hong et al. 2018).
Systematic literature reviews report a similarly broad range of vestibular symptoms. For example, a literature review of 17 studies found that the reported rate of vestibular symptoms in patients with LVA ranged from 2 – 71% (Stahl and Otteson 2022). Aside from this apparent variability in incidence, “the degree to which vestibular symptoms impact patients with EVA varies significantly” (Stahl and Otteson 2022).
One report describes the duration of vestibular symptoms as ranging “minutes to hours,” and also points out that the onset of vestibular symptoms may be delayed until adulthood (Oh, Ishiyama et al. 2001).
Presentation: head trauma
The literature contains numerous reports of minor head trauma precipitating acute hearing loss in patients with LVA (Walsh, Ayshford et al. 1999, Oh, Ishiyama et al. 2001), or leading to a diagnosis of LVA.
Some investigators report a fairly consistent relationship between head trauma (including minor head trauma) and acute hearing loss in LVA patients (Kou and Macdonald 1998, Walsh, Ayshford et al. 1999, Steinbach, Brockmeier et al. 2006, Noordman, van Beeck Calkoen et al. 2015, Wendt and Hashikawa 2019), while others report no relationship (Madden, Halsted et al. 2003, Alemi and Chan 2015). An epidemiologic survey conducted in Japan reported that only 5.3% of patients with LVA reported hearing loss following head trauma (Noguchi, Fukuda et al. 2017). Since the (putatively) precipitating head trauma can be quite mild, this naturally raises the question of whether patients with LVA should restrict their activities, such as by avoiding contact sports (Ralli, Nola et al. 2017, Brodsky and Choi 2018).
Although the relationship between head trauma and acute hearing loss in patients with LVA remains debated, since hearing loss can impose significant functional limitations (and is not easily treated), most clinicians recommend that patients with LVA refrain from contact sports out of an abundance of caution.
Physical examination
Rinne’s test may show conductive hearing loss on the side affected by LVA.
Ocular motor examination may reveal nystagmus. One study of three patients reported positional nystagmus, unidirectional horizontal nystagmus, and nystagmus reproduced with head turning to the affected side (White and Krakovitz 2015).
Testing: audiologic
Some, though not all (Nakano, Arimoto et al. 2022), infants with LVA are detected on newborn screening.
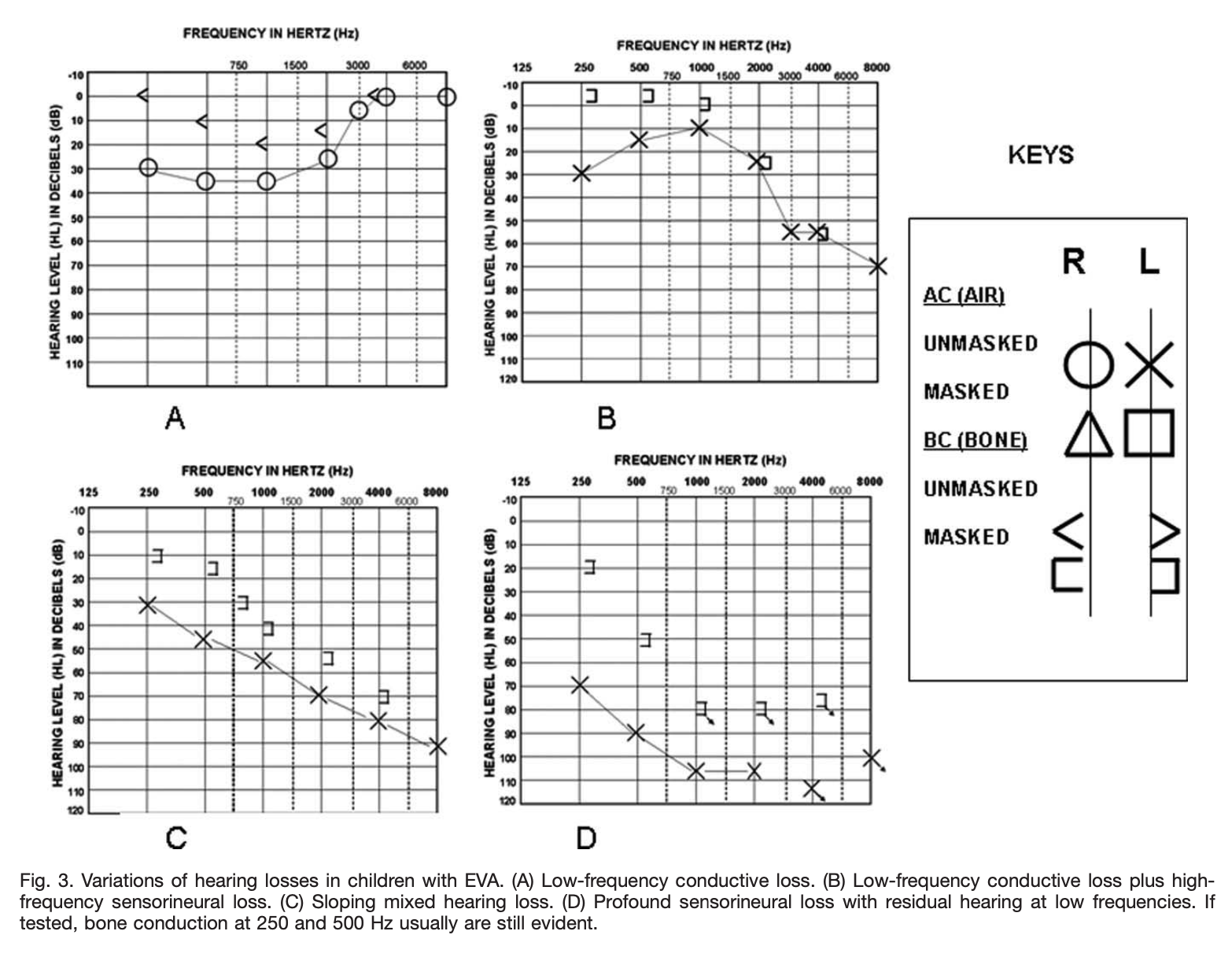
Most patients with LVA have hearing loss on audiometry that, on average, tends to slope from better (in the low frequencies) to worse (in the high frequencies), and usually has a conductive component, though often the hearing loss is mixed conductive and sensorineural (Sato, Nakashima et al. 2002). In practice, almost any pattern can be seen.
The Figure below from Zhou and Gopen (Zhou and Gopen 2011) displays several audiograms from pediatric patients with LVA.
Tympanometry sometimes shows an abnormally low resonance frequency (Sato, Nakashima et al. 2002).
One study explored the utility of acoustically evoked short latency negative response (part of the brainstem auditory evoked responses), and suggested that this might be helpful in diagnosis (Liu and Yang 2013). We are not aware of other literature about this.
Testing: vestibular
Relatively few studies have specifically explored vestibular function tests in patients with LVA.
One study of 31 LVA patients reported unilateral caloric weakness in 45% and bilateral caloric weakness in 6% of patients (Jung, Seo et al. 2016). Another study of 10 LVA patients reported unilateral caloric weakness in 30% (Jung, Suh et al. 2017).
Several case series studied LVA patients with rotatory chair testing (RCT), but did not report any sensitive or specific diagnostic findings (Zalewski, Chien et al. 2015, Yang, Lavender et al. 2016). Of 24 patients who underwent RCT, 4 (17%) showed decreased gain and 6 (25%) showed phase lead.
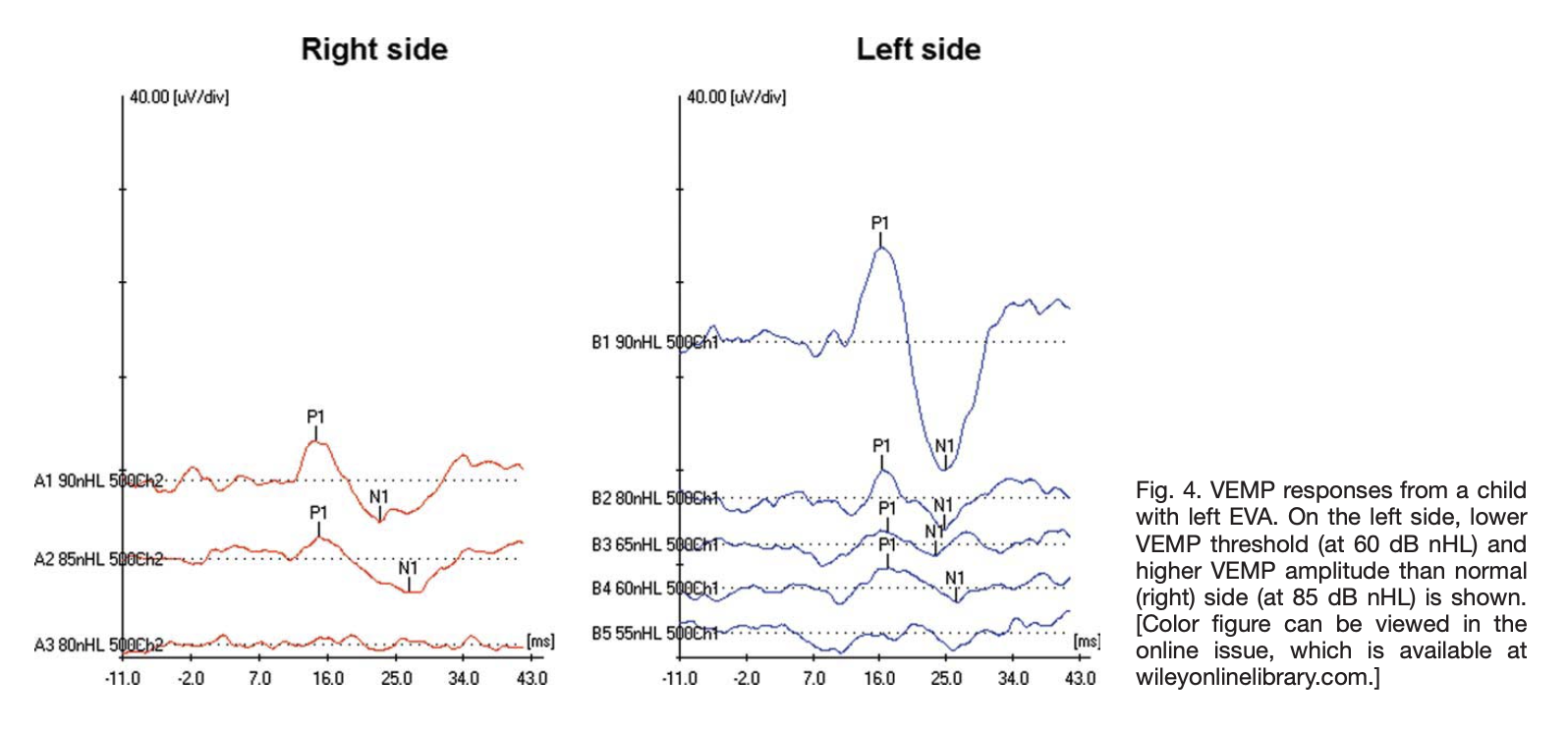
Several investigations have studies vestibular evoked myogenic potentials (VEMPs) in LVA patients. One study of vestibular evoked myogenic potentials in 29 bilateral LVA patients reported that in children ocular vestibular evoked myogenic potentials were present in 93% and cervical vestibular evoked myogenic potentials were present in 87%, whereas in adults ocular vestibular evoked myogenic potentials were present in in 83% and cervical vestibular evoked myogenic potentials were present in 75%; the authors concluded that LVA caused “a severer otolithic dysfunction in adults than in children” (Zhang, Chen et al. 2020). One study of children with LVA prior to cochlear implantation reported that compared to controls, the LVA patients exhibited, “shorter N1 latencies, shorter P1 latencies, and higher amplitudes” (Wang, Zhang et al. 2021). One study checked cervical vestibular evoked myogenic potentials on 9 patients and reported abnormalities in 2 (22%); specifically “1 ear from a patient with bilateral EVA had no measurable cVEMP response up to 107 dB nHL, and another ear from a patient with unilateral EVA had an abnormal amplitude symmetry ratio of 51% with a larger cVEMP amplitude in the ear affected with EVA” (Zalewski, Chien et al. 2015). A case study of a 42-year-old female with bilateral LVA reported that, “oVEMP reflexes demonstrated pathologically increased amplitudes and reduced thresholds for low-frequency tone bursts. Cervical VEMP amplitudes and thresholds were within normal limits for both ears across all frequencies of stimulation” (Taylor, Bradshaw et al. 2012). A retrospective cohort series studied 25 pediatric patients (37 ears) with cervical vestibular evoked myogenic potentials and found that hearing loss (with an air-bone gap) was present in 36 (97%) of ears; furthermore, despite the conductive component of hearing loss, “Abnormally low VEMP thresholds were found in 92% (34/37) of the ears with EVA. In addition, higher amplitudes were also noted in these cases. Statistically, the VEMP thresholds recorded from ears with EVA were significantly lower than that from non-EVA ears or normal ones” (Zhou and Gopen 2011).
The Figure below from Zhou and Gopen (Zhou and Gopen 2011) shows cervical vestibular evoked myogenic potentials (cVEMPs) from a patient with left-sided LVA. The cVEMP response on the left (right panel) shows larger than normal amplitude and lower than normal threshold.
One series of 5 pediatric patients studied electrocochleography (ECoG), and identified an elevated summation potential (and thus an elevated SP/AP ratio) in 2 (40%).
A few studies have explored video head impulse testing (vHIT) in LVA patients. A retrospective case-control study of 16 children (mean age 10.3 ± 4.4 years) with LVA before and after cochlear implantation reported that, “Statistically significant differences were not found in VOR gains of all three semicircular canals before and after surgery” (Wang, Zhang et al. 2021).
Another study noted a discrepancy between the results of caloric testing and video head impulse testing. This retrospective case series of 10 patients with LVA reported that, “40% showed unilateral caloric weakness and 30% had recurrent episodes of vertigo. All patients with recurrent vertigo had caloric weakness. However, only 25% of patients with abnormal caloric test results had abnormal vHIT results” (Jung, Suh et al. 2017). The authors noted that, “The discrepancy between the caloric test and vHIT results was also found in patients with MD.” The authors are referring to the fact that studies of vestibular tests in patients with Ménière’s disease sometimes report a dissociation between caloric testing (which may show unilateral caloric weakness) and video head impulse testing (which may be normal) (McGarvie, Curthoys et al. 2015, Rubin, Simon et al. 2018).
A literature review of 17 studies found that the reported rate of abnormalities among vestibular tests (physical examination maneuvers, caloric testing, electronystagmography, vestibular evoked myogenic potentials) ranged from 7 – 92% (Stahl and Otteson 2022).
A prospective cross-sectional cohort study evaluated 106 LVA patients with several vestibular tests (videonystagmography, cervical vestibular evoked myogenic potentials and rotatory chair testing) and reported that, “45% had vestibular signs and symptoms, and 44% of tested patients had abnormal VNG test results,” further observing that, “An increased number of vestibular signs and symptoms was correlated with the presence of bilateral EVA” (Zalewski, Chien et al. 2015).
Significantly, some studies report that the correlation between abnormal vestibular test results and the presence of vestibular symptoms is poor. For example, a prospective cohort study of 27 children (age 3 – 12 years) found abnormalities in vestibular tests (cervical vestibular evoked myogenic potentials, caloric testing, rotatory chair testing and posturography) in 24 (89%), yet only 6 (22%) actually endorsed a complaint of “vertigo,” leading the investigators to conclude that, “We found a high rate of vestibular pathology in children with EVA; however, the prevalence of abnormal vestibular testing findings in this patient population was not correlated with vestibular symptoms” (Yang, Lavender et al. 2016). Conversely, a prospective cross-sectional cohort study assessed 106 patients with several vestibular tests (videonystagmography, cervical vestibular evoked myogenic potentials, rotatory chair testing) and observed that “44% of tested patients abnormal VNG test results,” but further observed that, “not all patients with vestibular signs and symptoms have abnormal vestibular test results” (Zalewski, Chien et al. 2015).
Testing: genetic
Most, though not all (Claros, Fokouo et al. 2017), cases of LVA have an identifiable genetic abnormality.
Several hundred mutations in the SLC26A4 gene have been identified in patients with LVA. These mutations have been identified in various ethnic groups, including Iranian (Yazdanpanahi, Chaleshtori et al. 2012), Czech (Pourova, Janousek et al. 2010), Austrian (Roesch, Bernardinelli et al. 2018), and Chinese (Hu, Wu et al. 2007, Wang, Zhao et al. 2007, Yang, Gurrola et al. 2009, Guo, Wang et al. 2010, Lai, Hu et al. 2012, Yuan, Guo et al. 2012, Zhao, Yuan et al. 2012, Chai, Huang et al. 2013, Yao, Li et al. 2013, Pang, Chai et al. 2015, Pang, Chai et al. 2015, Yao, Qian et al. 2015, Li, Zhu et al. 2016, Liu, Wang et al. 2016, Wang, Zhang et al. 2016, Zhang, Bai et al. 2016, He, Peng et al. 2017, Zhu, Shi et al. 2017, Liang, Peng et al. 2018, Zhao, Cheng et al. 2018, Wen, Wang et al. 2019, Yu, Yang et al. 2019, Zhou, Huang et al. 2020, Tian, Xu et al. 2021, He, Zhao et al. 2022, Wu, Cui et al. 2022).
In other patients with LVA, mutations have been identified in CEVA (Chattaraj, Munjal et al. 2017, Chao, Chattaraj et al. 2019, Smits, de Bruijn et al. 2022), FOXI1(Song, Shin et al. 2014, Liu, Wen et al. 2020), GJB2 (Roesch, Rasp et al. 2021), KCNJ10 (Yang, Gurrola et al. 2009, Song, Shin et al. 2014, Liu, Wen et al. 2020) and POU3F4 (Roesch, Rasp et al. 2021).
Cases in which no genetic mutation is identified are few, and it seems likely that even these will eventually be shown to have identifiable mutations.
Imaging: CT
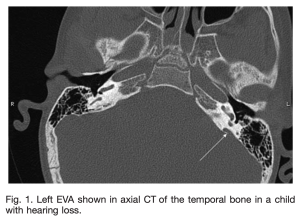
High resolution temporal bone CT is usually regarded as the imaging study of choice in identifying and characterizing LVA (Swartz, Yussen et al. 1985, Ma, Han et al. 2008, Maiolo, Savastio et al. 2013, Chen, Kachniarz et al. 2014, Gao, Jiang et al. 2019, Wang, Qin et al. 2022). There are debates regarding the specific CT technique and protocol (Hwang, Marovich et al. 2015, Weiss, Breitsprecher et al. 2022).
The Figure below from Zhou and Gopen (Zhou and Gopen 2011) shows an axial CT image from a child with a large vestibular aqueduct on the patient’s left.
Imaging: MRI
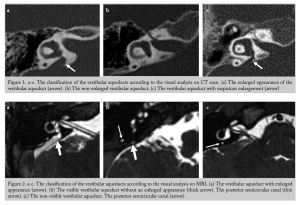
MRI has not (yet) surpassed CT in its ability to identify LVA, but in the interest of avoiding the ionizing radiation exposure of a temporal bone CT, some studies have explored whether MRI might serve as a screening test (Sarioglu, Cetin et al. 2020). Some investigators also advocate the use of MRI because of its superior characterization of soft tissue (Yang and Liu 2019).
There is modest literature regarding whether discrepancies between measurements of the vestibular aqueduct’s bony labyrinth and membranous labyrinth might have value in diagnosing LVA (Sun, Liang et al. 2019).
The Figure below from Sarioglu and colleagues (Sarioglu, Cetin et al. 2020)juxtaposes CT images (top panels) with MR images (bottom panels).
MRI may also be better than CT at diagnosing other otologic diseases and malformations with which LVA may be comorbid.
Correlations between workup and clinical features
The literature provides discrepant data regarding the correlation between genetics, imaging, audiologic testing and clinical features.
Some studies report some correlation between genotype and degree of hearing loss (Zhao, Lan et al. 2013) while others do not (Aimoni, Ciorba et al. 2017).
Some studies report a correlation between the genetic heterogeneity and the complexity of inner ear malformations (Azaiez, Yang et al. 2007).
Most studies report a correlation between various imaging parameters and the degree of hearing loss (Madden, Halsted et al. 2003, Seo, Kim et al. 2016, Ascha, Manzoor et al. 2017, Archibald, Ascha et al. 2019, Van Beck, Chinnadurai et al. 2020, Bouhadjer, Tissera et al. 2021, Anand, Stahl et al. 2022), though not all studies reach that conclusion (Abou-Elew, El-Khousht et al. 2014, Ruthberg, Ascha et al. 2019).
The clinical course is characterized by significant fluctuations in hearing (Berrettini, Forli et al. 2005, Ruthberg, Kocharyan et al. 2022), and this fluctuation may underlie the discrepant results regarding correlation between the genetic, imaging, audiologic and clinical features of the disease. One group concluded, “Our study failed to uncover factors that might be predictive of hearing loss. We conclude that until a better understanding of the natural history and pathophysiologic condition of EVAs is achieved, there is no surgical or other intervention that can be demonstrated as being efficacious” (Zalzal, Tomaski et al. 1995).
Differential diagnosis
Because LVA presents with conductive (or mixed) hearing loss, it is sometimes mistaken for otosclerosis (Tavora-Vieira and Miller 2012, Wieczorek, Anderson et al. 2013).
Comorbidities: LVA plus other otologic disease
LVA sometimes co-occurs with other inner ear malformations, such as cochlear dysplasia, vestibulocochlear dysplasia, modiolar hypoplasia (Atkin, Grimmer et al. 2009), dilated dysplastic vestibule (Emmrich and Fatterpekar 2011), enlargement of the vestibule (Lyu, Chen et al. 2017), shortening of the common crus (Lyu, Hong et al. 2017) enlargement of the lateral semicircular canal (Suzuki, Ota et al. 2016) and superior semicircular canal dehiscence (Brandolini and Modugno 2011). Whether these additional inner ear malformations are merely associated with LVA, or whether there is a causal relationship, is unclear (Grover 2021).
Some patients with LVA also develop benign paroxysmal positional vertigo (BPPV). A retrospective review of 26 patients with a radiological diagnosis of LVA reported that 5 (19%) of patients had nystagmus compatible with BPPV (Song, Hong et al. 2012). A retrospective review of 22 LVA patients (age 6 months – 35 years) reported that 4 (18%) developed BPPV (Song, Hong et al. 2018). Some investigators relate the increased risk of recurrent BPPV to volumetric abnormalities of the vestibular aqueduct on imaging (Manzari 2008).
Comorbidities: LVA plus other non-otologic disease
A survey of parents of 133 children reported a 10-fold greater risk of developing torticollis than the general population (Brodsky, Kaur et al. 2020).
Prognosis
The hearing loss in LVA is quite variable and fluctuates (Zalzal, Tomaski et al. 1995, Berrettini, Forli et al. 2005, Ruthberg, Kocharyan et al. 2022), though the overall trajectory is usually one of decline (Govaerts, Casselman et al. 1999, Mori, Westerberg et al. 2008, Mey, Bille et al. 2019).
Predicting that overall trajectory of decline in hearing has proven difficult. One study reported that “the standard deviation of hearing at 500 Hz was the only prognostic factor for the progression of PTA [pure tone average]” (Lai and Shiao 2004). Another study reported that several features can help predict progression of hearing loss, including male gender, operculum size, hearing at the time of diagnosis, and presence of an incomplete partition type 2 (Farrokhian, Kocharyan et al. 2022).
The clinical course tends to be punctuated by abrupt declines in hearing. Often these declines occur without any clear precipitant, while others are sometimes suspected to be due to head trauma. The mechanism of the abrupt hearing loss (with or without head trauma) is unknown. Hemorrhage has been suggested (Kim, Kim et al. 2011).
Treatment: cochlear implantation
Cochlear implantation is the most commonly performed procedure for treating the hearing loss associated with LVA (Dewan, Wippold et al. 2009, Lee, Lee et al. 2010, Powell and Birman 2015, Pritchett, Zwolan et al. 2015, Manzoor, Wick et al. 2016, Bostic, Lewis et al. 2018, Patel, Ascha et al. 2018, Jahn, Bergan et al. 2020, Hodge, Thompson et al. 2021, Reynard, Ionescu et al. 2021, Alahmadi, Abdelsamad et al. 2022, Benchetrit, Jabbour et al. 2022, Hansen, Rye Rasmussen et al. 2022, Li, Kang et al. 2022, Saeed, Rajai et al. 2022).
Treatment: other modalities
Dietary sodium restriction has been advocated (Hill, Freint et al. 1984), and incurs no significant medical risk.
Treatment with corticosteroids has been explored. Transtympanic steroids have been tried in LVA patients who suffered acute hearing loss following head trauma (Ralli, Nola et al. 2017). Steroids have also been tried in LVA patients without head trauma (Grimmer, Hedlund et al. 2008).
References
Abou-Elew M, El-Khousht M, El-Minawi MS, Selim M, Kamel AI (2014) Enlarged vestibular aqueduct in congenital non-syndromic sensorineural hearing loss in egypt. Indian J Otolaryngol Head Neck Surg 66: 88-94. doi: 10.1007/s12070-011-0327-2
Aimoni C, Ciorba A, Cerritelli L, Ceruti S, Skarzynski PH, Hatzopoulos S (2017) Enlarged vestibular aqueduct: Audiological and genetical features in children and adolescents. Int J Pediatr Otorhinolaryngol 101: 254-258. doi: 10.1016/j.ijporl.2017.07.042
Alahmadi A, Abdelsamad Y, Salamah M, Alenzi S, Badr KM, Alghamdi S, Alsanosi A (2022) Cochlear implantation in adults and pediatrics with enlarged vestibular aqueduct: a systematic review on the surgical findings and patients’ performance. Eur Arch Otorhinolaryngol 279: 5497-5509. doi: 10.1007/s00405-022-07511-7
Alemi AS, Chan DK (2015) Progressive Hearing Loss and Head Trauma in Enlarged Vestibular Aqueduct: A Systematic Review and Meta-analysis. Otolaryngol Head Neck Surg 153: 512-7. doi: 10.1177/0194599815596343
Anand R, Stahl M, Hicks K, Murray G, Patel N, Gupta A, Otteson T (2022) Assessing the clinical utility of volumetric HRCT in pediatric enlarged vestibular aqueduct related hearing loss. Int J Pediatr Otorhinolaryngol 155: 111067. doi: 10.1016/j.ijporl.2022.111067
Archibald HD, Ascha M, Gupta A, Megerian C, Otteson T (2019) Hearing loss in unilateral and bilateral enlarged vestibular aqueduct syndrome. Int J Pediatr Otorhinolaryngol 118: 147-151. doi: 10.1016/j.ijporl.2018.12.023
Ascha MS, Manzoor N, Gupta A, Semaan M, Megerian C, Otteson TD (2017) Vestibular Aqueduct Midpoint Width and Hearing Loss in Patients With an Enlarged Vestibular Aqueduct. JAMA Otolaryngol Head Neck Surg 143: 601-608. doi: 10.1001/jamaoto.2016.4522
Atkin JS, Grimmer JF, Hedlund G, Park AH (2009) Cochlear abnormalities associated with enlarged vestibular aqueduct anomaly. Int J Pediatr Otorhinolaryngol 73: 1682-5. doi: 10.1016/j.ijporl.2009.08.028
Azaiez H, Yang T, Prasad S, Sorensen JL, Nishimura CJ, Kimberling WJ, Smith RJ (2007) Genotype-phenotype correlations for SLC26A4-related deafness. Hum Genet 122: 451-7. doi: 10.1007/s00439-007-0415-2
Benchetrit L, Jabbour N, Appachi S, Liu YC, Cohen MS, Anne S (2022) Cochlear Implantation in Pediatric Patients With Enlarged Vestibular Aqueduct: A Systematic Review. Laryngoscope 132: 1459-1472. doi: 10.1002/lary.29742
Berrettini S, Forli F, Bogazzi F, Neri E, Salvatori L, Casani AP, Franceschini SS (2005) Large vestibular aqueduct syndrome: audiological, radiological, clinical, and genetic features. Am J Otolaryngol 26: 363-71. doi: 10.1016/j.amjoto.2005.02.013
Bostic K, Lewis RM, Chai B, Manganella JL, Barrett DL, Kawai K, Kenna MA, Stiles DJ, Clark T (2018) Enlarged Vestibular Aqueduct and Cochlear Implants: The Effect of Early Counseling on the Length of Time Between Candidacy and Implantation. Otol Neurotol 39: e90-e95. doi: 10.1097/MAO.0000000000001663
Bouhadjer K, Tissera K, Farris CW, Juliano AF, Cunnane ME, Curtin HD, Mankarious LA, Reinshagen KL (2021) Retrospective Review of Midpoint Vestibular Aqueduct Size in the 45 degrees Oblique (Poschl) Plane and Correlation with Hearing Loss in Patients with Enlarged Vestibular Aqueduct. AJNR Am J Neuroradiol 42: 2215-2221. doi: 10.3174/ajnr.A7339
Brandolini C, Modugno GC (2011) Superior semicircular canal dehiscence and enlarged vestibular aqueduct. Int J Pediatr Otorhinolaryngol 75: 861-3. doi: 10.1016/j.ijporl.2011.03.001
Brodsky JR, Choi SS (2018) Should children with an enlarged vestibular aqueduct be restricted from playing contact sports? Laryngoscope 128: 2219-2220. doi: 10.1002/lary.27119
Brodsky JR, Kaur K, Shoshany T, Manganella J, Barrett D, Kawai K, Murray M, Licameli G, Albano V, Stolzer A, Kenna M (2020) Torticollis in children with enlarged vestibular aqueducts. Int J Pediatr Otorhinolaryngol 131: 109862. doi: 10.1016/j.ijporl.2020.109862
Chai Y, Huang Z, Tao Z, Li X, Li L, Li Y, Wu H, Yang T (2013) Molecular etiology of hearing impairment associated with nonsyndromic enlarged vestibular aqueduct in East China. Am J Med Genet A 161A: 2226-33. doi: 10.1002/ajmg.a.36068
Chao JR, Chattaraj P, Munjal T, Honda K, King KA, Zalewski CK, Chien WW, Brewer CC, Griffith AJ (2019) SLC26A4-linked CEVA haplotype correlates with phenotype in patients with enlargement of the vestibular aqueduct. BMC Med Genet 20: 118. doi: 10.1186/s12881-019-0853-4
Chattaraj P, Munjal T, Honda K, Rendtorff ND, Ratay JS, Muskett JA, Risso DS, Roux I, Gertz EM, Schaffer AA, Friedman TB, Morell RJ, Tranebjaerg L, Griffith AJ (2017) A common SLC26A4-linked haplotype underlying non-syndromic hearing loss with enlargement of the vestibular aqueduct. J Med Genet 54: 665-673. doi: 10.1136/jmedgenet-2017-104721
Chen JX, Kachniarz B, Shin JJ (2014) Diagnostic yield of computed tomography scan for pediatric hearing loss: a systematic review. Otolaryngol Head Neck Surg 151: 718-39. doi: 10.1177/0194599814545727
Claros P, Fokouo JV, Claros A (2017) Cochlear implantation in patients with enlarged vestibular aqueduct. A case series with literature review. Cochlear Implants Int 18: 125-129. doi: 10.1080/14670100.2016.1268754
Dewan K, Wippold FJ, 2nd, Lieu JE (2009) Enlarged vestibular aqueduct in pediatric sensorineural hearing loss. Otolaryngol Head Neck Surg 140: 552-8. doi: 10.1016/j.otohns.2008.12.035
Emmrich JV, Fatterpekar GM (2011) Dilated dysplastic vestibule: a new computed tomographic finding in patients with large vestibular aqueduct syndrome. J Comput Assist Tomogr 35: 674-8. doi: 10.1097/RCT.0b013e318232988b
Farrokhian N, Kocharyan A, Ruthberg J, Piper R, Rivas A, Semaan M, Otteson T, Manzoor NF (2022) Predictive Modeling and Risk Stratification of Patients With Enlarged Vestibular Aqueduct. Laryngoscope 132: 1439-1445. doi: 10.1002/lary.29936
Gao B, Jiang Y, Huang S, Wang Q, Gao X, Cai J, Dai P (2019) Application of multiplanar reconstruction of spiral CT in the diagnosis and treatment of enlarged vestibular aqueducts. Acta Otolaryngol 139: 665-670. doi: 10.1080/00016489.2019.1612534
Govaerts PJ, Casselman J, Daemers K, De Ceulaer G, Somers T, Offeciers FE (1999) Audiological findings in large vestibular aqueduct syndrome. Int J Pediatr Otorhinolaryngol 51: 157-64. doi: 10.1016/s0165-5876(99)00268-2
Greinwald J, DeAlarcon A, Cohen A, Uwiera T, Zhang K, Benton C, Halstead M, Meinzen-Derr J (2013) Significance of unilateral enlarged vestibular aqueduct. Laryngoscope 123: 1537-46. doi: 10.1002/lary.23889
Grimmer JF, Hedlund G (2007) Vestibular symptoms in children with enlarged vestibular aqueduct anomaly. Int J Pediatr Otorhinolaryngol 71: 275-82. doi: 10.1016/j.ijporl.2006.10.010
Grimmer JF, Hedlund G, Park A (2008) Steroid treatment of hearing loss in enlarged vestibular aqueduct anomaly. Int J Pediatr Otorhinolaryngol 72: 1711-5. doi: 10.1016/j.ijporl.2008.08.009
Grover M (2021) Enlarged vestibular aqueduct and cochlear anomalies: just an association or a causal relationship? Cochlear Implants Int 22: 182. doi: 10.1080/14670100.2019.1667089
Guo YF, Wang YL, Xu BC, Liu XW, Zhu YM, Zhao FF, Ji YB, Zhou Y, Li JQ, Li Q, Wang DY, Wang QJ (2010) Identification of two novel mutations, c.232T>C and c.2006A>T, in SLC26A4 in a Chinese family associated with enlarged vestibular aqueduct. Int J Pediatr Otorhinolaryngol 74: 831-5. doi: 10.1016/j.ijporl.2010.04.005
Han JW, Wang L, Zhao H, Yang SM (2020) Biomechanical analysis of the clinical characteristics of enlarged vestibular aqueduct syndrome with Mondini malformation. Acta Otolaryngol 140: 813-817. doi: 10.1080/00016489.2020.1780312
Hansen MU, Rye Rasmussen E, Caye-Thomasen P, Mey K (2022) Cochlear Implantation in Children with Enlarged Vestibular Aqueduct: A Systematic Review of Surgical Implications and Outcomes. Ear Hear. doi: 10.1097/AUD.0000000000001309
He X, Peng Q, Li S, Zhu P, Wu C, Rao C, Chang J, Xie M, Zhong B, Lu X (2017) A novel missense mutation in the SLC26A4 gene causes nonsyndromic hearing loss and enlarged vestibular aqueduct. Int J Pediatr Otorhinolaryngol 95: 104-108. doi: 10.1016/j.ijporl.2017.02.013
He X, Zhao S, Shi L, Lu Y, Yang Y, Zhang X (2022) Compound heterozygous variants of the SLC26A4 gene in a Chinese family with enlarged vestibular aqueducts. BMC Med Genomics 15: 152. doi: 10.1186/s12920-022-01271-3
Hill JH, Freint AJ, Mafee MF (1984) Enlargement of the vestibular aqueduct. Am J Otolaryngol 5: 411-4. doi: 10.1016/s0196-0709(84)80057-5
Hodge SE, Thompson NJ, Park LR, Brown KD (2021) Enlarged Vestibular Aqueduct: Hearing Progression and Cochlear Implant Candidacy in Pediatric Patients. Otol Neurotol 42: 203-206. doi: 10.1097/MAO.0000000000003034
Hu H, Wu L, Feng Y, Pan Q, Long Z, Li J, Dai H, Xia K, Liang D, Niikawa N, Xia J (2007) Molecular analysis of hearing loss associated with enlarged vestibular aqueduct in the mainland Chinese: a unique SLC26A4 mutation spectrum. J Hum Genet 52: 492-497. doi: 10.1007/s10038-007-0139-0
Hwang M, Marovich R, Shin SS, Chi D, Branstetter BFt (2015) Optimizing CT for the evaluation of vestibular aqueduct enlargement: Inter-rater reproducibility and predictive value of reformatted CT measurements. J Otol 10: 13-17. doi: 10.1016/j.joto.2015.07.004
Jahn KN, Bergan MD, Arenberg JG (2020) Auditory Detection Thresholds and Cochlear Resistivity Differ Between Pediatric Cochlear Implant Listeners With Enlarged Vestibular Aqueduct and Those With Connexin-26 Mutations. Am J Audiol 29: 23-34. doi: 10.1044/2019_AJA-19-00054
Jung J, Seo YW, Choi JY, Kim SH (2016) Vestibular function is associated with residual low-frequency hearing loss in patients with bi-allelic mutations in the SLC26A4 gene. Hear Res 335: 33-39. doi: 10.1016/j.heares.2016.02.009
Jung J, Suh MJ, Kim SH (2017) Discrepancies between video head impulse and caloric tests in patients with enlarged vestibular aqueduct. Laryngoscope 127: 921-926. doi: 10.1002/lary.26122
Kim M, Kim J, Kim SH, Kim SC, Jeon JH, Lee WS, Kim UK, Kim HN, Choi JY (2011) Hemorrhage in the endolymphatic sac: a cause of hearing fluctuation in enlarged vestibular aqueduct. Int J Pediatr Otorhinolaryngol 75: 1538-44. doi: 10.1016/j.ijporl.2011.09.002
Kou B, Macdonald R (1998) Toronto’s Hospital for Sick Children study of traumatic sudden sensorineural hearing loss. J Otolaryngol 27: 64-8.
Lai CC, Shiao AS (2004) Chronological changes of hearing in pediatric patients with large vestibular aqueduct syndrome. Laryngoscope 114: 832-8. doi: 10.1097/00005537-200405000-00008
Lai R, Hu P, Zhu F, Zhu G, Vivero R, Peng A, Wu W, Xiao Z, Liu X, Xie D (2012) Genetic diagnosis and cochlear implantation for patients with nonsyndromic hearing loss and enlarged vestibular aqueduct. J Laryngol Otol 126: 349-55. doi: 10.1017/S002221511100346X
Lee KH, Lee J, Isaacson B, Kutz JW, Roland PS (2010) Cochlear implantation in children with enlarged vestibular aqueduct. Laryngoscope 120: 1675-81. doi: 10.1002/lary.20987
Li J, Kang S, Du H, Wang S, Wang D, Liu M, Yang S (2022) Analysis of Cochlear Parameters in Paediatric Inner Ears with Enlarged Vestibular Aqueduct and Patent Cochlea. J Pers Med 12. doi: 10.3390/jpm12101666
Li Y, Zhu B, Su J, Yin Y, Yu F (2016) Identification of SLC26A4 mutations p.L582LfsX4, p.I188T and p.E704K in a Chinese family with large vestibular aqueduct syndrome (LVAS). Int J Pediatr Otorhinolaryngol 91: 1-5. doi: 10.1016/j.ijporl.2016.08.026
Liang Y, Peng Q, Wang K, Zhu P, Wu C, Rao C, Chang J, Li S, Lu X (2018) A novel mutation in the SLC26A4 gene in a Chinese family with non-syndromic hearing loss and enlarged vestibular aqueduct. Int J Pediatr Otorhinolaryngol 107: 97-100. doi: 10.1016/j.ijporl.2018.01.037
Liu L, Yang B (2013) Acoustically evoked short latency negative responses in hearing loss patients with enlarged vestibular aqueduct. Acta Neurol Belg 113: 157-60. doi: 10.1007/s13760-012-0138-6
Liu Y, Wang L, Feng Y, He C, Liu D, Cai X, Jiang L, Chen H, Liu C, Wu H, Mei L (2016) A New Genetic Diagnostic for Enlarged Vestibular Aqueduct Based on Next-Generation Sequencing. PLoS One 11: e0168508. doi: 10.1371/journal.pone.0168508
Liu Y, Wen J, Sang S, Mei L, He C, Jiang L, Huang S, Feng Y (2020) Next-generation sequencing-based mutation analysis of genes associated with enlarged vestibular aqueduct in Chinese families. Eur Arch Otorhinolaryngol 277: 3331-3339. doi: 10.1007/s00405-020-06050-3
Lyu H, Chen K, Xie Y, Yang L, Zhang T, Dai P (2017a) Morphometric Study of the Vestibular Aqueduct in Patients With Enlarged Vestibular Aqueduct. J Comput Assist Tomogr 41: 467-471. doi: 10.1097/RCT.0000000000000524
Lyu H, Hong J, Yin D, Chen K, Li J, Yang L, Zhang T, Dai P (2017b) Position of the Internal Aperture of Vestibular Aqueduct in Patients With Enlarged Vestibular Aqueduct. Otol Neurotol 38: 1198-1204. doi: 10.1097/MAO.0000000000001495
Ma H, Han P, Liang B, Tian ZL, Lei ZQ, Kong WJ, Feng GS (2008) Multislice spiral computed tomography imaging in congenital inner ear malformations. J Comput Assist Tomogr 32: 146-50. doi: 10.1097/rct.0b013e318063c64a
Macielak RJ, Mattingly JK, Findlen UM, Moberly AC, Malhotra PS, Adunka OF (2019) Audiometric findings in children with unilateral enlarged vestibular aqueduct. Int J Pediatr Otorhinolaryngol 120: 25-29. doi: 10.1016/j.ijporl.2019.01.034
Madden C, Halsted M, Benton C, Greinwald J, Choo D (2003) Enlarged vestibular aqueduct syndrome in the pediatric population. Otol Neurotol 24: 625-32. doi: 10.1097/00129492-200307000-00016
Maiolo V, Savastio G, Modugno GC, Barozzi L (2013) Relationship between multidetector CT imaging of the vestibular aqueduct and inner ear pathologies. Neuroradiol J 26: 683-92. doi: 10.1177/197140091302600612
Manzari L (2008) Enlarged vestibular aqueduct (EVA) related with recurrent benign paroxysmal positional vertigo (BPPV). Med Hypotheses 70: 61-5. doi: 10.1016/j.mehy.2007.04.032
Manzoor NF, Wick CC, Wahba M, Gupta A, Piper R, Murray GS, Otteson T, Megerian CA, Semaan MT (2016) Bilateral Sequential Cochlear Implantation in Patients With Enlarged Vestibular Aqueduct (EVA) Syndrome. Otol Neurotol 37: e96-103. doi: 10.1097/MAO.0000000000000925
McGarvie LA, Curthoys IS, MacDougall HG, Halmagyi GM (2015) What does the dissociation between the results of video head impulse versus caloric testing reveal about the vestibular dysfunction in Meniere’s disease? Acta Otolaryngol 135: 859-65. doi: 10.3109/00016489.2015.1015606
Mey K, Bille M, Rye Rasmussen SH, Tranebjaerg L, Caye-Thomasen P (2019) The Natural History of Hearing Loss in Pendred Syndrome and Non-Syndromic Enlarged Vestibular Aqueduct. Otol Neurotol 40: e178-e185. doi: 10.1097/MAO.0000000000002140
Mimura T, Sato E, Sugiura M, Yoshino T, Naganawa S, Nakashima T (2005) Hearing loss in patients with enlarged vestibular aqueduct: air-bone gap and audiological Bing test. Int J Audiol 44: 466-9. doi: 10.1080/14992020500057665
Mori T, Westerberg BD, Atashband S, Kozak FK (2008) Natural history of hearing loss in children with enlarged vestibular aqueduct syndrome. J Otolaryngol Head Neck Surg 37: 112-8.
Nakano A, Arimoto Y, Mutai H, Nara K, Inoue S, Matsunaga T (2022) Clinical and genetic analysis of children with hearing loss and bilateral enlarged vestibular aqueducts. Int J Pediatr Otorhinolaryngol 152: 110975. doi: 10.1016/j.ijporl.2021.110975
Noguchi Y, Fukuda S, Fukushima K, Gyo K, Hara A, Nakashima T, Ogawa K, Okamoto M, Sato H, Usami SI, Yamasoba T, Yokoyama T, Kitamura K (2017) A nationwide study on enlargement of the vestibular aqueduct in Japan. Auris Nasus Larynx 44: 33-39. doi: 10.1016/j.anl.2016.04.012
Noordman BJ, van Beeck Calkoen E, Witte B, Goverts T, Hensen E, Merkus P (2015) Prognostic factors for sudden drops in hearing level after minor head injury in patients with an enlarged vestibular aqueduct: a meta-analysis. Otol Neurotol 36: 4-11. doi: 10.1097/MAO.0000000000000659
Oh AK, Ishiyama A, Baloh RW (2001) Vertigo and the enlarged vestibular aqueduct syndrome. J Neurol 248: 971-4. doi: 10.1007/s004150170050
Pang X, Chai Y, Chen P, He L, Wang X, Wu H, Yang T (2015a) Mono-allelic mutations of SLC26A4 is over-presented in deaf patients with non-syndromic enlarged vestibular aqueduct. Int J Pediatr Otorhinolaryngol 79: 1351-3. doi: 10.1016/j.ijporl.2015.06.009
Pang X, Chai Y, He L, Chen P, Wang X, Li L, Jia H, Wu H, Yang T (2015b) A 7666-bp genomic deletion is frequent in Chinese Han deaf patients with non-syndromic enlarged vestibular aqueduct but without bi-allelic SLC26A4 mutations. Int J Pediatr Otorhinolaryngol 79: 2248-52. doi: 10.1016/j.ijporl.2015.10.015
Patel ND, Ascha MS, Manzoor NF, Gupta A, Semaan M, Megerian C, Otteson TD (2018) Morphology and cochlear implantation in enlarged vestibular aqueduct. Am J Otolaryngol 39: 657-663. doi: 10.1016/j.amjoto.2018.06.006
Pourova R, Janousek P, Jurovcik M, Dvorakova M, Malikova M, Raskova D, Bendova O, Leonardi E, Murgia A, Kabelka Z, Astl J, Seeman P (2010) Spectrum and frequency of SLC26A4 mutations among Czech patients with early hearing loss with and without Enlarged Vestibular Aqueduct (EVA). Ann Hum Genet 74: 299-307. doi: 10.1111/j.1469-1809.2010.00581.x
Powell HR, Birman CS (2015) Large vestibular aqueduct syndrome: Impedance changes over time with different cochlear implant electrode arrays. Cochlear Implants Int 16: 326-30. doi: 10.1179/1754762815Y.0000000013
Pritchett C, Zwolan T, Huq F, Phillips A, Parmar H, Ibrahim M, Thorne M, Telian S (2015) Variations in the cochlear implant experience in children with enlarged vestibular aqueduct. Laryngoscope 125: 2169-74. doi: 10.1002/lary.25187
Ralli M, Nola G, Sparvoli L, Ralli G (2017) Unilateral Enlarged Vestibular Aqueduct Syndrome and Bilateral Endolymphatic Hydrops. Case Rep Otolaryngol 2017: 6195317. doi: 10.1155/2017/6195317
Reynard P, Ionescu E, Joly CA, Ltaief-Boudrigua A, Coudert A, Thai-Van H (2021) Vestibular impairment in cochlear implanted children presenting enlarged vestibular aqueduct and enlarged endolymphatic sac. Int J Pediatr Otorhinolaryngol 141: 110557. doi: 10.1016/j.ijporl.2020.110557
Riggs WJ, Hiss MM, Varadarajan VV, Mattingly JK, Adunka OF (2020) Enlarged vestibular aqueduct: Intraoperative electrocochleography findings during cochlear implantation. Int J Pediatr Otorhinolaryngol 134: 110065. doi: 10.1016/j.ijporl.2020.110065
Roesch S, Bernardinelli E, Nofziger C, Toth M, Patsch W, Rasp G, Paulmichl M, Dossena S (2018) Functional Testing of SLC26A4 Variants-Clinical and Molecular Analysis of a Cohort with Enlarged Vestibular Aqueduct from Austria. Int J Mol Sci 19. doi: 10.3390/ijms19010209
Roesch S, Rasp G, Sarikas A, Dossena S (2021) Genetic Determinants of Non-Syndromic Enlarged Vestibular Aqueduct: A Review. Audiol Res 11: 423-442. doi: 10.3390/audiolres11030040
Rubin F, Simon F, Verillaud B, Herman P, Kania R, Hautefort C (2018) Comparison of Video Head Impulse Test and Caloric Reflex Test in advanced unilateral definite Meniere’s disease. Eur Ann Otorhinolaryngol Head Neck Dis 135: 167-169. doi: 10.1016/j.anorl.2017.08.008
Ruthberg J, Ascha MS, Kocharyan A, Gupta A, Murray GS, Megerian CA, Otteson TD (2019) Sex-specific enlarged vestibular aqueduct morphology and audiometry. Am J Otolaryngol 40: 473-477. doi: 10.1016/j.amjoto.2019.03.008
Ruthberg JS, Kocharyan A, Farrokhian N, Stahl MC, Hicks K, Scarborough J, Murray GS, Wu S, Manzoor N, Otteson T (2022) Hearing loss patterns in enlarged vestibular aqueduct syndrome: Do fluctuations have clinical significance? Int J Pediatr Otorhinolaryngol 156: 111072. doi: 10.1016/j.ijporl.2022.111072
Saeed HS, Rajai A, Nash R, Saeed SR, Stivaros SM, Black G, Bruce IA (2022) Enlarged Vestibular Aqueduct: Disease Characterization and Exploration of Potential Prognostic Factors for Cochlear Implantation. Otol Neurotol 43: e563-e570. doi: 10.1097/MAO.0000000000003518
Sarioglu FC, Cetin AC, Guleryuz H, Guneri EA (2020) The Diagnostic Efficacy of MRI in the Evaluation of the Enlarged Vestibular Aqueduct in Children with Hearing Loss. Turk Arch Otorhinolaryngol 58: 220-226. doi: 10.5152/tao.2020.5864
Sato E, Nakashima T, Lilly DJ, Fausti SA, Ueda H, Misawa H, Uchida Y, Furuhashi A, Asahi K, Naganawa S (2002) Tympanometric findings in patients with enlarged vestibular aqueducts. Laryngoscope 112: 1642-6. doi: 10.1097/00005537-200209000-00021
Seo YJ, Kim J, Choi JY (2016) Correlation of vestibular aqueduct size with air-bone gap in enlarged vestibular aqueduct syndrome. Laryngoscope 126: 1633-8. doi: 10.1002/lary.25664
Sheykholeslami K, Schmerber S, Habiby Kermany M, Kaga K (2004) Vestibular-evoked myogenic potentials in three patients with large vestibular aqueduct. Hear Res 190: 161-8. doi: 10.1016/S0378-5955(04)00018-8
Smits JJ, de Bruijn SE, Lanting CP, Oostrik J, O’Gorman L, Mantere T, Consortium D, Cremers FPM, Roosing S, Yntema HG, de Vrieze E, Derks R, Hoischen A, Pegge SAH, Neveling K, Pennings RJE, Kremer H (2022) Exploring the missing heritability in subjects with hearing loss, enlarged vestibular aqueducts, and a single or no pathogenic SLC26A4 variant. Hum Genet 141: 465-484. doi: 10.1007/s00439-021-02336-6
Song JJ, Hong SK, Kim JS, Koo JW (2012) Enlarged vestibular aqueduct may precipitate benign paroxysmal positional vertigo in children. Acta Otolaryngol 132 Suppl 1: S109-17. doi: 10.3109/00016489.2012.662714
Song JJ, Hong SK, Lee SY, Park SJ, Kang SI, An YH, Jang JH, Kim JS, Koo JW (2018) Vestibular Manifestations in Subjects With Enlarged Vestibular Aqueduct. Otol Neurotol 39: e461-e467. doi: 10.1097/MAO.0000000000001817
Song MH, Shin JW, Park HJ, Lee KA, Kim Y, Kim UK, Jeon JH, Choi JY (2014) Intrafamilial phenotypic variability in families with biallelic SLC26A4 mutations. Laryngoscope 124: E194-202. doi: 10.1002/lary.24504
Stahl MC, Otteson T (2022) Systematic Review on Vestibular Symptoms in Patients With Enlarged Vestibular Aqueducts. Laryngoscope 132: 873-880. doi: 10.1002/lary.29819
Steinbach S, Brockmeier SJ, Kiefer J (2006) The large vestibular aqueduct–case report and review of the literature. Acta Otolaryngol 126: 788-95. doi: 10.1080/00016480500527276
Subramaniam S, Tan TY, Yuen HW (2012) Bilateral enlarged vestibular aqueduct with associated bilateral Mondini’s dysplasia. Am J Otolaryngol 33: 455-6. doi: 10.1016/j.amjoto.2012.01.005
Sun W, Liang Q, Kuang S, Zhou S, Wang W (2019) 3D-real IR MRI detects serendipity of inner ear in enlarged vestibular aqueduct syndrome. Acta Otolaryngol 139: 233-237. doi: 10.1080/00016489.2018.1563719
Suzuki M, Ota Y, Tanaka T, Ota Y (2016) Lateral Semicircular Canal-enlarged Vestibular Aqueduct Fistula Associated With Paroxysmal Positional Nystagmus. Otol Neurotol 37: e192-3. doi: 10.1097/MAO.0000000000000778
Swartz JD, Yussen PS, Mandell DW, Mikaelian DO, Berger AS, Wolfson RJ (1985) The vestibular aqueduct syndrome: computed tomographic appearance. Clin Radiol 36: 241-3. doi: 10.1016/s0009-9260(85)80046-5
Tavora-Vieira D, Miller S (2012) Misdiagnosis of otosclerosis in a patient with enlarged vestibular aqueduct syndrome: a case report. J Med Case Rep 6: 178. doi: 10.1186/1752-1947-6-178
Taylor RL, Bradshaw AP, Magnussen JS, Gibson WP, Halmagyi GM, Welgampola MS (2012) Augmented ocular vestibular evoked myogenic potentials to air-conducted sound in large vestibular aqueduct syndrome. Ear Hear 33: 768-71. doi: 10.1097/AUD.0b013e31825ce613
Tian Y, Xu H, Liu D, Zhang J, Yang Z, Zhang S, Liu H, Li R, Tian Y, Zeng B, Li T, Lin Q, Wang H, Li X, Lu W, Shi Y, Zhang Y, Zhang H, Jiang C, Xu Y, Chen B, Liu J, Tang W (2021) Increased diagnosis of enlarged vestibular aqueduct by multiplex PCR enrichment and next-generation sequencing of the SLC26A4 gene. Mol Genet Genomic Med 9: e1734. doi: 10.1002/mgg3.1734
Van Beck J, Chinnadurai S, Morrison AK, Zuniga MG, Smith B, Lohse CM, McCaslin D (2020) Correlation of air-bone gap and size of Enlarged Vestibular Aqueduct in children. Int J Pediatr Otorhinolaryngol 132: 109909. doi: 10.1016/j.ijporl.2020.109909
van Beeck Calkoen EA, Pennings RJE, Smits J, Pegge S, Rotteveel LJC, Merkus P, Verbist BM, Sanchez E, Hensen EF (2021) Contralateral hearing loss in children with a unilateral enlarged vestibular aqueduct. Int J Pediatr Otorhinolaryngol 150: 110891. doi: 10.1016/j.ijporl.2021.110891
Walsh RM, Ayshford CA, Chavda SV, Proops DW (1999) Large vestibular aqueduct syndrome. ORL J Otorhinolaryngol Relat Spec 61: 41-4. doi: 10.1159/000027637
Wang L, Qin Y, Zhu L, Li X, Chen Y, Zhang L (2022) Auditory and imaging markers of atypical enlarged vestibular aqueduct. Eur Arch Otorhinolaryngol 279: 695-702. doi: 10.1007/s00405-021-06700-0
Wang M, Zhang F, Xu L, Xiao Y, Li J, Fan Z, Sun Q, Bai X, Wang H (2016) Novel compound heterozygous mutations in SLC26A4 gene in a Chinese Han family with enlarged vestibular aqueduct. Int J Pediatr Otorhinolaryngol 90: 170-174. doi: 10.1016/j.ijporl.2016.09.018
Wang QJ, Zhao YL, Rao SQ, Guo YF, Yuan H, Zong L, Guan J, Xu BC, Wang DY, Han MK, Lan L, Zhai SQ, Shen Y (2007) A distinct spectrum of SLC26A4 mutations in patients with enlarged vestibular aqueduct in China. Clin Genet 72: 245-54. doi: 10.1111/j.1399-0004.2007.00862.x
Wang R, Zhang D, Luo J, Chao X, Xu J, Liu X, Fan Z, Wang H, Xu L (2021) Influence of Cochlear Implantation on Vestibular Function in Children With an Enlarged Vestibular Aqueduct. Front Neurol 12: 663123. doi: 10.3389/fneur.2021.663123
Weiss NM, Breitsprecher TM, Pscheidl A, Bachinger D, Volkenstein S, Dazert S, Mlynski R, Langner S, Roland P, Dhanasingh A (2022) Volumetry improves the assessment of the vestibular aqueduct size in inner ear malformation. Eur Arch Otorhinolaryngol. doi: 10.1007/s00405-022-07681-4
Wen C, Wang S, Zhao X, Wang X, Wang X, Cheng X, Huang L (2019) Mutation analysis of the SLC26A4 gene in three Chinese families. Biosci Trends 13: 441-447. doi: 10.5582/bst.2019.01282
Wendt WJ, Hashikawa A (2019) Enlarged Vestibular Aqueduct Syndrome: Sudden Hearing Loss in a Child with a Cerebral Shunt. Pediatr Emerg Care 35: e135-e137. doi: 10.1097/PEC.0000000000001043
White J, Krakovitz P (2015) Nystagmus in Enlarged Vestibular Aqueduct: A Case Series. Audiol Res 5: 120. doi: 10.4081/audiores.2015.120
Wieczorek SS, Anderson ME, Jr., Harris DA, Mikulec AA (2013) Enlarged vestibular aqueduct syndrome mimicking otosclerosis in adults. Am J Otolaryngol 34: 619-25. doi: 10.1016/j.amjoto.2013.07.015
Wu T, Cui L, Mou Y, Guo W, Liu D, Qiu J, Xu C, Zhou J, Han F, Sun Y (2022) A newly identified mutation (c.2029 C > T) in SLC26A4 gene is associated with enlarged vestibular aqueducts in a Chinese family. BMC Med Genomics 15: 49. doi: 10.1186/s12920-022-01200-4
Yang CJ, Lavender V, Meinzen-Derr JK, Cohen AP, Youssif M, Castiglione M, Manickam V, Bachmann KR, Greinwald JH (2016) Vestibular pathology in children with enlarged vestibular aqueduct. Laryngoscope 126: 2344-50. doi: 10.1002/lary.25890
Yang L, Liu J (2019) Comparative Analysis of CT and MRI Diagnosis of Large Vestibular Aqueduct Syndrome (LVAS) in Children. J Coll Physicians Surg Pak 29: 753-756. doi: 10.29271/jcpsp.2019.08.753
Yang T, Gurrola JG, 2nd, Wu H, Chiu SM, Wangemann P, Snyder PM, Smith RJ (2009) Mutations of KCNJ10 together with mutations of SLC26A4 cause digenic nonsyndromic hearing loss associated with enlarged vestibular aqueduct syndrome. Am J Hum Genet 84: 651-7. doi: 10.1016/j.ajhg.2009.04.014
Yao G, Li S, Chen D, Wang H, Zhang J, Feng Z, Guo L, Yang Z, Yang S, Sun C, Zhang X, Ma D (2013) Compound heterozygous mutations of SLC26A4 in 4 Chinese families with enlarged vestibular aqueduct. Int J Pediatr Otorhinolaryngol 77: 544-9. doi: 10.1016/j.ijporl.2013.01.002
Yao J, Qian X, Bao J, Wei Q, Lu Y, Zheng H, Cao X, Xing G (2015) Probing the Effect of Two Heterozygous Mutations in Codon 723 of SLC26A4 on Deafness Phenotype Based on Molecular Dynamics Simulations. Sci Rep 5: 10831. doi: 10.1038/srep10831
Yazdanpanahi N, Chaleshtori MH, Tabatabaiefar MA, Noormohammadi Z, Farrokhi E, Najmabadi H, Shahbazi S, Hosseinipour A (2012) Two novel SLC26A4 mutations in Iranian families with autosomal recessive hearing loss. Int J Pediatr Otorhinolaryngol 76: 845-50. doi: 10.1016/j.ijporl.2012.02.056
Yu Y, Yang Y, Lu J, Jin Y, Yang Y, Hong E, Shi J, Chen F, Han S, Chu P, Guo Y, Ni X (2019) Two Compound Heterozygous Were Identified in SLC26A4 Gene in Two Chinese Families With Enlarged Vestibular Aqueduct. Clin Exp Otorhinolaryngol 12: 50-57. doi: 10.21053/ceo.2018.00213
Yuan Y, Guo W, Tang J, Zhang G, Wang G, Han M, Zhang X, Yang S, He DZ, Dai P (2012) Molecular epidemiology and functional assessment of novel allelic variants of SLC26A4 in non-syndromic hearing loss patients with enlarged vestibular aqueduct in China. PLoS One 7: e49984. doi: 10.1371/journal.pone.0049984
Zalewski CK, Chien WW, King KA, Muskett JA, Baron RE, Butman JA, Griffith AJ, Brewer CC (2015) Vestibular Dysfunction in Patients with Enlarged Vestibular Aqueduct. Otolaryngol Head Neck Surg 153: 257-62. doi: 10.1177/0194599815585098
Zalzal GH, Tomaski SM, Vezina LG, Bjornsti P, Grundfast KM (1995) Enlarged vestibular aqueduct and sensorineural hearing loss in childhood. Arch Otolaryngol Head Neck Surg 121: 23-8. doi: 10.1001/archotol.1995.01890010011003
Zhang F, Bai X, Xiao Y, Zhang X, Zhang G, Li J, Xu L, Wang H (2016) Identification of a novel mutation in SLC26A4 gene in a Chinese family with enlarged vestibular aqueduct syndrome. Int J Pediatr Otorhinolaryngol 85: 75-9. doi: 10.1016/j.ijporl.2016.03.020
Zhang Y, Chen Z, Zhang Y, Hu J, Wang J, Xu M, Zhang Q (2020) Vestibular-evoked myogenic potentials in patients with large vestibular aqueduct syndrome. Acta Otolaryngol 140: 40-45. doi: 10.1080/00016489.2019.1687937
Zhao FF, Lan L, Wang DY, Han B, Qi Y, Zhao Y, Zong L, Li Q, Wang QJ (2013) Correlation analysis of genotypes, auditory function, and vestibular size in Chinese children with enlarged vestibular aqueduct syndrome. Acta Otolaryngol 133: 1242-9. doi: 10.3109/00016489.2013.822555
Zhao J, Yuan Y, Chen J, Huang S, Wang G, Han D, Dai P (2012) SLC26A4 gene copy number variations in Chinese patients with non-syndromic enlarged vestibular aqueduct. J Transl Med 10: 82. doi: 10.1186/1479-5876-10-82
Zhao X, Cheng X, Huang L, Wang X, Wen C, Wang X (2018) Novel compound heterozygous mutations in SLC26A4 gene in a Chinese family with enlarged vestibular aqueduct. Biosci Trends 12: 502-506. doi: 10.5582/bst.2018.01260
Zhou G, Gopen Q (2011) Characteristics of vestibular evoked myogenic potentials in children with enlarged vestibular aqueduct. Laryngoscope 121: 220-5. doi: 10.1002/lary.21184
Zhou K, Huang L, Feng M, Li X, Zhao Y, Liu F, Wei J, Qin D, Lu Q, Shi M, Qu S, Tang F (2020) A novel SLC26A4 splicing mutation identified in two deaf Chinese twin sisters with enlarged vestibular aqueducts. Mol Genet Genomic Med 8: e1447. doi: 10.1002/mgg3.1447
Zhu GJ, Shi LS, Zhou H, Yang Y, Chen J, Gao X (2017) A novel compound heterozygous mutation of SLC26A4 in two Chinese families with nonsyndromic hearing loss and enlarged vestibular aqueducts. Mol Med Rep 16: 9011-9016. doi: 10.3892/mmr.2017.7690
![]()