By Marcello Cherchi, MD PhD
For patients
Formal audiometry is a test of hearing. This can identify whether hearing loss is present, and characterize the hearing loss. Results from audiometry can help diagnose some ear diseases and some disorders of equilibrium. During the test you will be seated in a soundproof booth wearing earbud insert earphones. You may hear various tones at different levels of loudness, and you may be asked to repeat words. The test takes about 30 minutes. The test is not uncomfortable. If you have wax in your ears, this should be removed before you have audiometry performed; otherwise there is no special preparation for this test. There are no specific instructions you need to follow after this test.
For clinicians
Overview
Formal audiometry assesses several aspects of hearing. Pure tone air-conducted and bone-conducted hearing are among the most useful audiologic tests for otoneurology and neuro-otology, as these can assess whether hearing loss is present, and whether it is sensorineural, conductive, or mixed. Conducting audiometry in a soundproof audiology booth with earbud inserts is desirable. The test can be performed either by an audiologist or a trained otologic technician.
Introduction
There are several fine reviews of the methodology and techniques of audiometry that are accessible to the neurologist, such as that by Davies (Davies 2016).
Information from audiometry is important for diagnosis and management of some otovestibular conditions.
Physiology and neuroanatomy
Familiarity with the anatomy and physiology of the auditory system is helpful in understanding how audiometry works and how to interpret its results. We provide an overview of the auditory system elsewhere.
Equipment needed
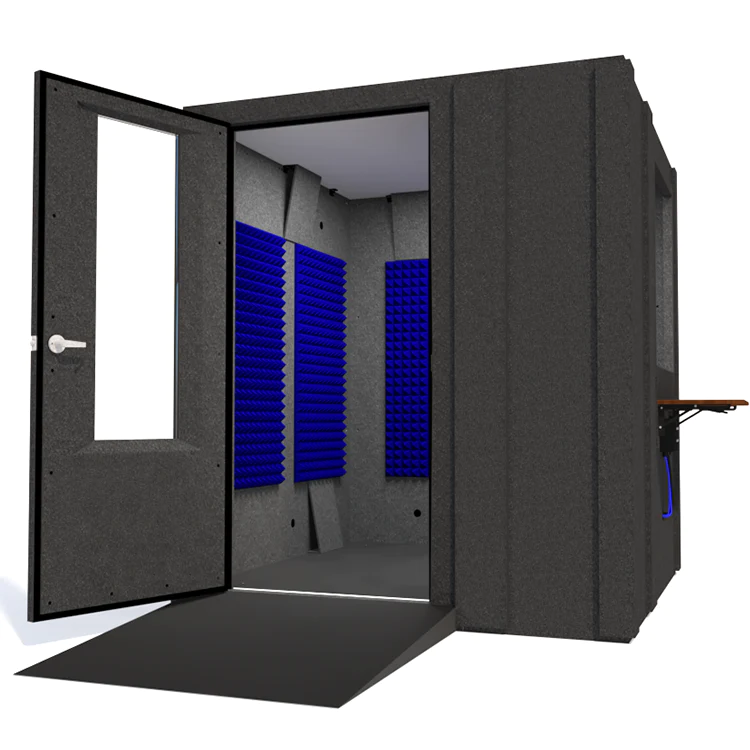
Ideally audiometry should be performed in a for-purpose soundproof audiometry booth (example in the Figure below) using earbud inserts (example in the Figure below) driven by a diagnostic audiometer (example in Figure below).
 |
 |
 |
“Portable” hearing booths (about the dimensions of an old phone booth) exist. Their advantage is that they occupy less space. Their disadvantages include that they are more uncomfortable for the patient, and some individuals feel claustrophobic.
The use of over-the-ear headphones can give suboptimal results.
Many of the basic audiometry tests can be performed by a trained otologic technician. Other procedures are better left to a trained audiologist.
How to perform the test
Basic audiometry consists of several parts, not every one of which is required in all patients. The main components are:
- Pure tone testing in each ear. In this section of the test, tones of various frequencies and amplitudes are presented to one or the other ear. If the patient hears the tone, they press the button. If they do not hear the tone, they do nothing. The audiologist plots the threshold (softest sound) at each frequency for each ear. Standard audiometry checks octave intervals of 250 Hz, 500 Hz, 1 kHz, 2 kHz, 4 kHz and 8 kHz. Often pure tone testing is assessed with two methods: first with air conducted stimuli, then with bone-conducted stimuli (using a bone vibrator); if hearing loss is present, this can distinguish whether it is sensorineural, conductive, or mixed.
- Speech reception thresholds in each ear. This is the lowest amplitude at which the patient can perceive at least 50% of the speech material presented.
- Word recognition score in each ear. This is the percentage of words that the patient can correctly repeat back from a spoken list.
What this test assesses
Pure tone testing assesses the “first step” in auditory processing — whether a patient can perceive a given frequency at a given amplitude — and this information is the most helpful part of audiometry for the otoneurologist.
The other components (speech reception thresholds and word recognition scores) test higher levels of processing. Usually these results are approximately commensurate with the results of pure tone testing. In some patients there is a discrepancy, such as when speech reception thresholds and word recognition scores are disproportionately poor compared to the pure tone hearing results; this can occur with aging, and with auditory processing disorders.
How to interpret the test results
The results from pure tone audiometry are usually presented on a graph, such as that shown in the Figure below. The X‑axis represents frequencies, progressing from lower frequencies at the left, to higher frequencies on the right. The Y‑axis represents amplitude, progressing from softer sounds at the top, to louder sounds on the bottom. On the graph, air-conducted hearing thresholds (the softest sound at which a patient can perceive the stimulus) are plotted as red circles (“O”) for the right ear and blue “X”s for the left ear.
Audiologists usually recognize the following gradation of hearing thresholds:
- ‑10 to 20 dB: Normal hearing.
- 20 – 40 dB: Mild hearing loss.
- 40 – 70 dB: Moderate hearing loss.
- 70 – 90 dB: Severe hearing loss.
- 90 – 120 dB: Profound hearing loss.
In the Figure below, pure tone hearing is bilaterally normal at 125 – 250 kHz, then slopes gradually down to approximately symmetrical, severe hearing loss at 6 – 8 kHz.
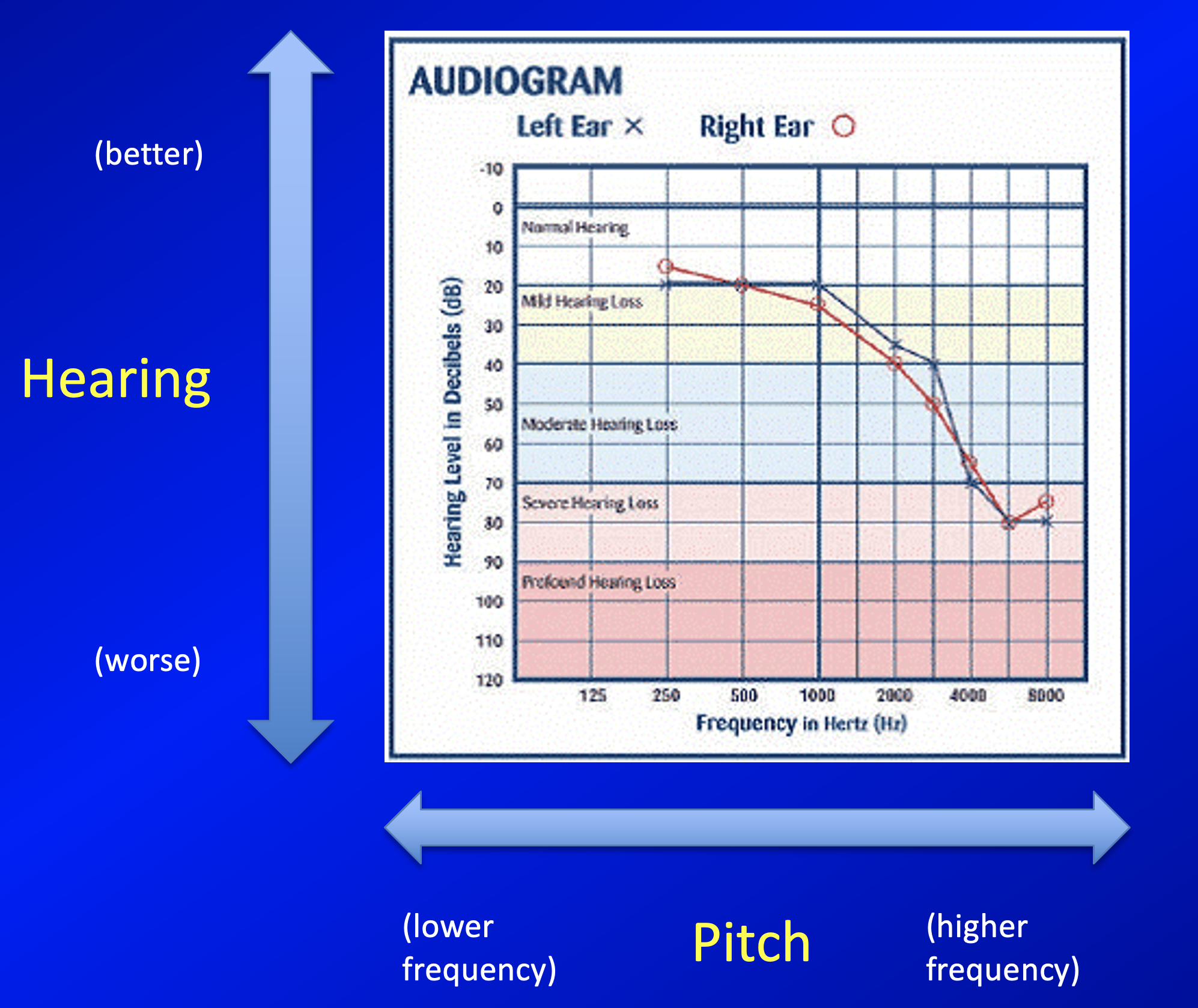
The graph in the Figure above only shows results for air-conducted stimuli.
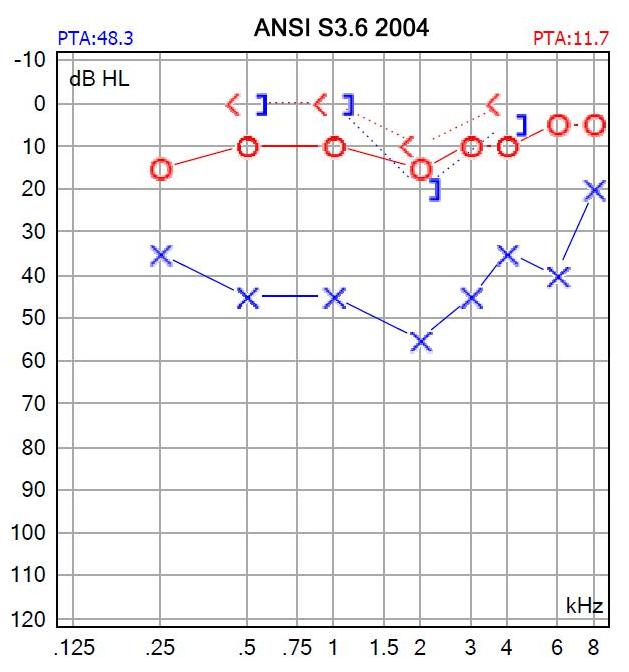
The results of bone-conducted hearing thresholds are usually plotted at a red “less than” sign (“<”) for the right ear, and a blue square bracket opening towards the left (“]”) for the left ear. The audiogram in the Figure below shows normal hearing on the right side; on the left side air-conducted hearing shows hearing loss at 250 Hz – 6 kHz. In contrast, bone-conducted hearing is within the normal range at 500 Hz – 4 kHz, resulting in air-bone gaps of 45 dB at 500 Hz – 1 kHz, 35 dB at 2 kHz and 30 dB at 4 kHz, which means that there is conductive hearing loss at those frequencies.
The Figure below illustrates that sensorineural hearing loss results from dysfunction in the cochlea or cochlear nerve, while conductive hearing loss results from mechanical dysfunction in the external ear (such as cerumen) or middle ear (such as a middle ear effusion, otosclerosis, ossicular chain dislocation, etc.).
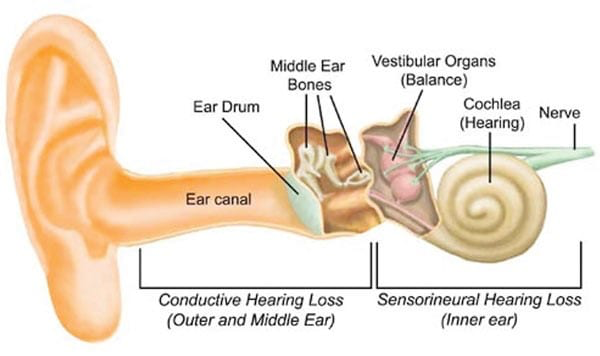
When a patient is found to have conductive or mixed hearing loss, it is reasonable to check tympanometry to assess middle ear function.
Limitations
Note that audiometry is a subjective test, in the sense that the patient’s responses rely on their cooperative and truthful participation. Regular audiometry cannot, for example, identify non-physiologic hearing loss (such as from psychiatric conditions or malingering).
Contraindications
There are no significant contraindications to audiometry.
Pitfalls
There are several potential sources of error in standard audiometry, including:
- Mechanical failures – the headphones can, and do, burn out.
- Calibration. Old (analog) audiometers need to be checked and re-calibrated periodically. In theory, new (digital) audiometers do not need calibration.
- Improper technique, or inexperienced technician/audiologist.
- Poor patient cooperation, whether unintentional (e.g., language barrier, cognitive impairment) or intentional (e.g., malingering).
When is the test indicated
Indications for audiometry include:
- Any new subjective hearing loss, particularly if asymmetrical.
- Any acute change in hearing.
- New tinnitus, or abrupt change from prior baseline of tinnitus.
- Many cases of dizziness (depending on the clinical scenario).
- Medico-legal cases, including head trauma (even if there is no specific complaint of hearing loss).
Diseases that may be diagnosed by this test
There are numerous disorders that involve changes in auditory function, such as Ménière’s disease, ototoxicity, autoimmune inner ear disease, presbycusis, auditory neuropathy, noise-induced hearing loss, labyrinthine ossification, vestibular schwannoma, Ramsay Hunt syndrome, labyrinthitis, sudden sensorineural hearing loss, superior semicircular canal dehiscence, hyperacusis, middle ear effusion, temporal bone fracture, large vestibular aqueduct, Mondini dysplasia, Pendred syndrome, Usher syndrome, superficial siderosis, intracranial pressure fluctuations, cortical deafness, COVID‑19, HIV, otosyphilis, radiation exposure, central auditory processing disorders, and many others.
Some research is beginning to explore the degree to which auditory assessment alone may predict vestibular dysfunction (Nicolas-Puel et al. 2025).
Additional notes
The soundproof audiology booth can be used for certain other audiologic tests as well, such as otoacoustic emissions.
References
Davies RA (2016) Audiometry and other hearing tests. Handb Clin Neurol 137: 157-76. doi: 10.1016/B978-0-444-63437-5.00011-X
Nicolas-Puel C, Bourien J, Nouvian R, Puel JL, Ceccato JC (2025) Audiometry as a predictive proxy for balance dysfunction. Sci Rep 15: 13722. doi: 10.1038/s41598-025-97995-0
![]()