By Marcello Cherchi, MD PhD
For patients
Mondini dysplasia (sometimes also called a Mondini malformation) is a congenital inner ear disorder that usually presents with significant hearing loss. The diagnosis is usually confirmed on a high resolution CT of the temporal bone. Some patients may elect to treat the hearing loss with cochlear implantation. If Mondini dysplasia is diagnosed or suspected, then a patient should consult with an otolaryngologist.
For clinicians
Overview
Mondini dysplasia is a congenital inner ear anomaly in which the cochlea has only 1.5 turns, the vestibule is enlarged, and the vestibular aqueduct is large. Mondini dysplasia accounts for over 50% of all congenital inner ear anomalies. It can be unilateral or bilateral, and can occur in syndromic contexts (Klippel-Feil syndrome, Pendred syndrome, DiGeorge syndrome and Down syndrome). It usually presents with severe to profound hearing loss, though some patients have relatively preserved high frequency hearing. Some patients also complain of disequilibrium. Mondini dysplasia is usually identified on a high resolution temporal bone CT, though MRI of the internal auditory canals may also be informative. Some patients benefit from cochlear implantation. A patient with diagnosed (or suspected) Mondini dysplasia should be referred to otolaryngology for evaluation.
Introduction
Carlo Mondini (1729 – 1803) was an Italian physician and anatomist who served as the chair of anatomy at the University of Bologna beginning in 1782. In 1791 he published a report of a dissection of a congenitally deaf 8-year-old boy (Mondini 1791, Mondini 1997). The findings he described included (Lo 1999):
- The cochlea consisted of 1.5 turns (instead of the normal 2.5 or 2.75 turns). Subsequent authors also comment on a cystic apex (Sennaroglu and Saatci 2004) and incomplete cochlear partition type 2 (referring to partial absence of the interscalar septum).
- The vestibule was enlarged, but the semicircular canals were normal.
- The vestibular aqueduct was enlarged and the endolymphatic sac was dilated.
The Figure below is one of several illustrations in Mondini’s original article (Mondini 1791) showing the cochlea with only 1.5 turns.

Some authors are careful to invoke the eponymous designation to refer to the specific set of abnormalities that Mondini originally described. Some commentators (Jackler, Luxford et al. 1987, Lo 1999) have noted that much otologic literature unfortunately uses the phrases “Mondini dysplasia,” “Mondini defect,” “Mondini anomaly” and “Mondini malformation” to refer to almost any inner ear anomaly, which has made diagnosis, classification and analysis more difficult.
Epidemiology
Mondini dysplasia accounts for >50% of all congenital inner ear malformations (Kaya, Hizli et al. 2017). It can occur unilaterally or bilaterally (Schuknecht 1980).
Embryology
The embryologically-based classification of congenital inner ear anomalies proposed by Jackler and colleagues (Jackler, Luxford et al. 1987) comments that an intrauterine insult around the 7th week of gestation can lead to the incomplete cochlear partition characteristic of the “classical Mondini’s” dysplasia.
Histopathology
Kaya and colleagues reported that patients with Mondini dysplasia exhibited a statistically significant reduction in density of type 1 and type 2 hair cells and reduced total number of hair cells, in the cristae of all the semicircular canals, compared to controls (Kaya, Hizli et al. 2017).
Clinical presentation: hearing loss
All patients have hearing loss, which can range from severe to profound. Some patients have relatively preserved high frequency hearing (Feghali, Leone et al. 1985), which is usually attributed to the fact that the base of the cochlea (that mediates high frequency hearing) is still present in Mondini dysplasia (Jackler, Luxford et al. 1987).
Clinical presentation: vestibular symptoms
Some literature states that patients occasionally have vestibular symptoms (Kaya, Hizli et al. 2017).
Comorbidities
Mondini dysplasia can occur in association with other congenital abnormalities, such as Klippel-Feil syndrome, Pendred syndrome, DiGeorge syndrome and Down syndrome (Kaya, Hizli et al. 2017).
Imaging
High resolution temporal bone CT is the imaging study of choice, though MRI of the internal auditory canals can provide complementary information.
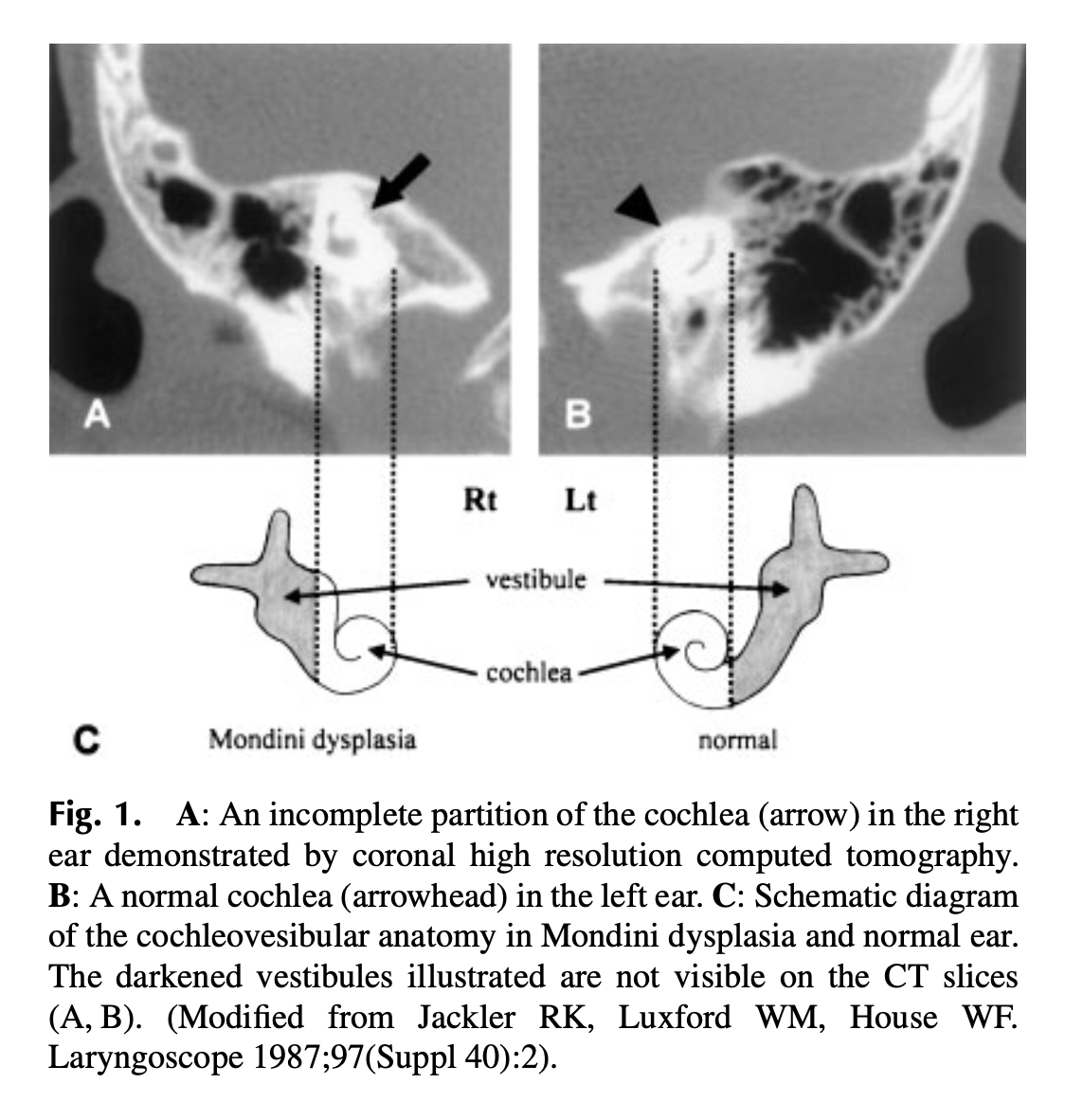
The Figure below, from Kitazawa and colleagues (Kitazawa, Matsumoto et al. 2004), shows bilateral Mondini dysplasia, with corresponding schematics.
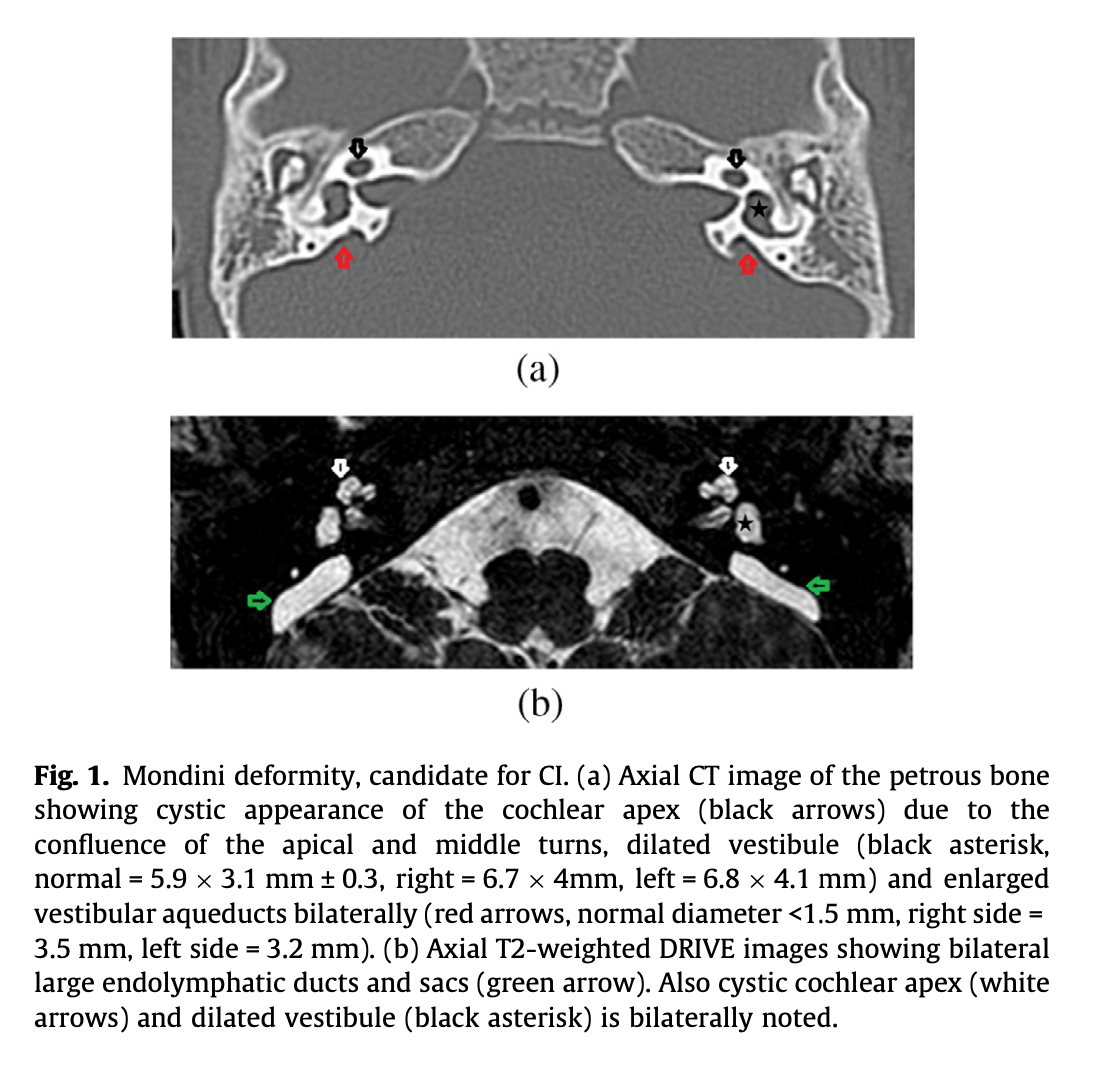
The Figure below, from Al-Rawy and colleagues (Rawy, Al-Shatouri et al. 2018), shows axial images from temporal bone CT (top panel) and MRI of the internal auditory canals (bottom panel) of a patient with bilateral Mondini dysplasia.
Treatment
Some patients elect cochlear implantation to manage the hearing loss.
References
Feghali JG, Leone CA, Linthicum FH, Jr. (1985) Residual high-frequency hearing in a patient with Mondini’s deformity: clinical implications. Am J Otol 6: 336-7.
Jackler RK, Luxford WM, House WF (1987) Congenital malformations of the inner ear: a classification based on embryogenesis. Laryngoscope 97: 2-14. doi: 10.1002/lary.5540971301
Kaya S, Hizli O, Kaya FK, Monsanto RD, Paparella MM, Cureoglu S (2017) Peripheral vestibular pathology in Mondini dysplasia. Laryngoscope 127: 206-209. doi: 10.1002/lary.25995
Kitazawa K, Matsumoto M, Senda M, Honda A, Morimoto N, Kawashiro N, Imashuku S (2004) Mondini dysplasia and recurrent bacterial meningitis in a girl with relapsing Langerhans cell histiocytosis. Pediatr Blood Cancer 43: 85-7. doi: 10.1002/pbc.20057
Lo WW (1999) What is a ‘Mondini’ and what difference does a name make? AJNR Am J Neuroradiol 20: 1442-4.
Mondini C (1791) Anatomica surdi natisectio. De Bononiensi scientarum et artium institute atque academia commentarii. Bononiae 7: 419-431.
Mondini C (1997) Minor works of Carlo Mondini: the anatomical section of a boy born deaf. Am J Otol 18: 288-93.
Rawy A, Al-Shatouri M, Tabbakh M, Gad A (2018) Systematic approach by computed tomography and magnetic resonance imaging in cochlear implantation candidates in Suez Canal University Hospital. The Egyptian Journal of Radiology and Nuclear Medicine 48. doi: 10.1016/j.ejrnm.2017.08.005
Schuknecht HF (1980) Mondini dysplasia; a clinical and pathological study. Ann Otol Rhinol Laryngol Suppl 89: 1-23.
Sennaroglu L, Saatci I (2004) Unpartitioned versus incompletely partitioned cochleae: radiologic differentiation. Otol Neurotol 25: 520-9; discussion 529. doi: 10.1097/00129492-200407000-00020
![]()