By Marcello Cherchi, MD PhD
For patients
Some degree of hearing loss comes along with normal healthy aging, and is sometimes called presbycusis or age-related hearing loss. There are probably multiple factors that contribute to age-related hearing loss. This type of hearing loss usually starts slowly, progresses gradually, and is similar in both ears. A hearing test will usually show that the high frequencies are affected first, and more than the lower frequencies. If history of hearing loss is unusual (for example, it starts abruptly or progresses very rapidly), or if a hearing test is unusual (for example, it shows that one ear is affected much more than the other, or that the low frequencies are more affected than the high frequencies), then your doctor may suspect other causes and consider additional testing. Patients with presbycusis often consult an audiologist, who may recommend amplification.
For clinicians
Practical summary
The term presbycusis is synonymous with the phrase age-related hearing loss. These refer to insidious onset, gradually progressive, bilateral, symmetrical sensorineural hearing loss that is more pronounced in the higher frequencies, resulting from physiologic and pathologic changes in most or all of the structures in the auditory pathway. Presbycusis is extremely common. Risk factors include environmental and probably genetic, though the genetic factors have not yet been clearly defined. Bedside hearing tests may serve the purpose of screening, but formal audiometry is superior for identifying the pattern of hearing loss compatible with presbycusis. Unexpected findings may prompt the search for alternative explanations. There is no curative or arrestive direct therapy for presbycusis. Many patients consult with an audiologist and may eventually consider amplification strategies.
Introduction
Presbycusis, or age-related hearing loss (ARHL), “refers to hearing loss as a result of physiologic and pathologic changes associated with increasing age” (Patel and McKinnon 2018) and can be “defined as a progressive, bilateral, symmetrical age-related sensorineural hearing loss, which is most pronounced at the higher frequencies” (Bowl and Dawson 2019). Hearing loss in general is an extraordinarily common condition. In the United States in 1990 – 1992, hearing loss was the third most common chronic problem in persons age 65 – 74 years (after arthritis and hypertension) and the second most common chronic problem in persons age ≥75 (after arthritis) (Collins 1997).
Epidemiology
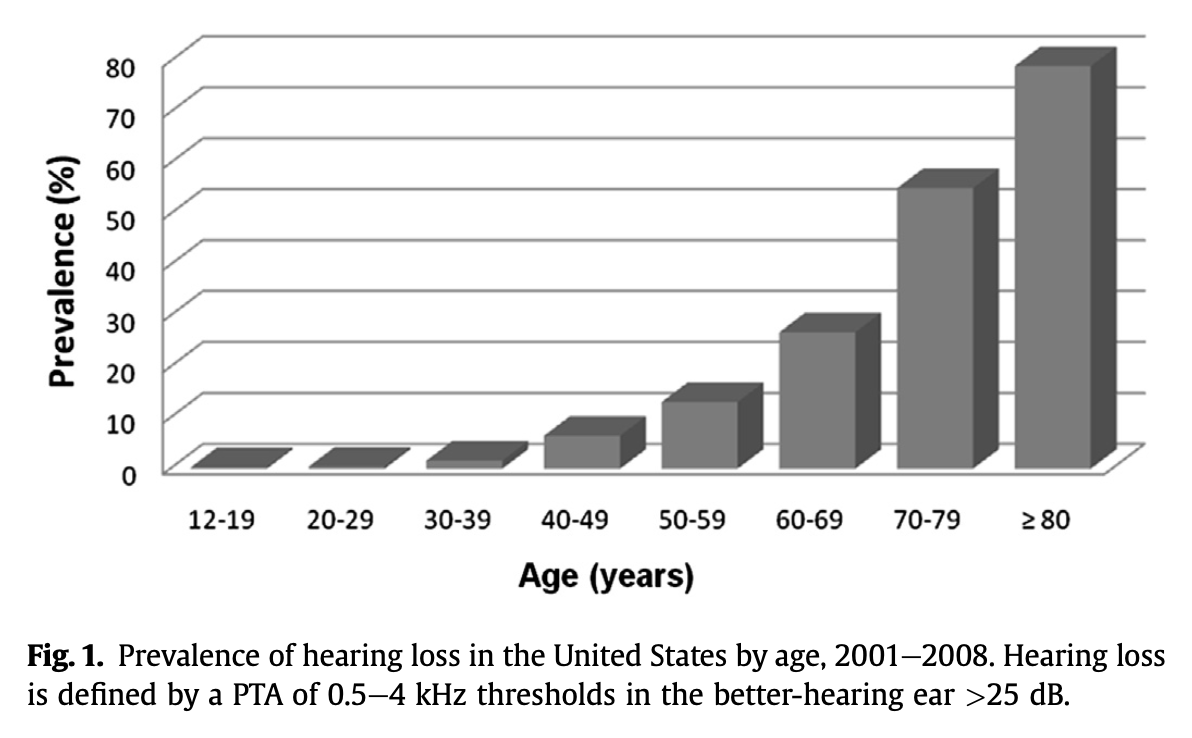
Repeated studies have demonstrated an increase in hearing loss with age.
The Figure below, from Yamasoba and colleagues (Yamasoba et al. 2013), shows the prevalence of hearing loss by decade in the United States.
Genetics
Accumulating studies suggest that “genetic predisposition forms a large and important risk factor for ARHL” (Bowl and Dawson 2019), but Bowl and Dawson also review the difficulties of identifying candidate genes even using genome-wide association studies. Nevertheless, there have been some advances in identifying likely candidate genes (Wells et al. 2020).
Pathophysiological mechanism of disease
In a general sense presbycusis reflects age-related attrition of sensoria, but it is likely that multiple mechanisms contribute to this decline (Yamasoba et al. 2013). Bowl and Dawson summarize:
“Historical studies of postmortem human temporal bones suggest that ARHL involves a number of auditory structures: degeneration of the mechanotransducing cochlear inner and outer hair cells (sensory presbycusis); reduced function within the stria vascularis (SV) (strial presbycusis, also known as metabolic presbycusis); and degeneration of the auditory nerve (neural presbycusis)… However, in reality, it is likely most people with presbycusis will show a ‘mixed’ pathology. In addition to peripheral lesions it is also likely that there will be changes occurring in central auditory pathways that contribute to the development and progression of ARHL… As such, ARHL is considered a multifactorial disorder with underlying risk factors that can be divided into several categories: biological age, gender, ethnicity, environment (e.g., noise exposure, ototoxic medications), lifestyle (e.g., smoking, drinking, diet), health comorbidities (e.g., hypertension, diabetes), and genetic pre- disposition” (Collins 1997).
Elliott and colleagues (Elliott et al. 2022) review the various patterns of degenerative changes occurring at different points along the auditory pathway.
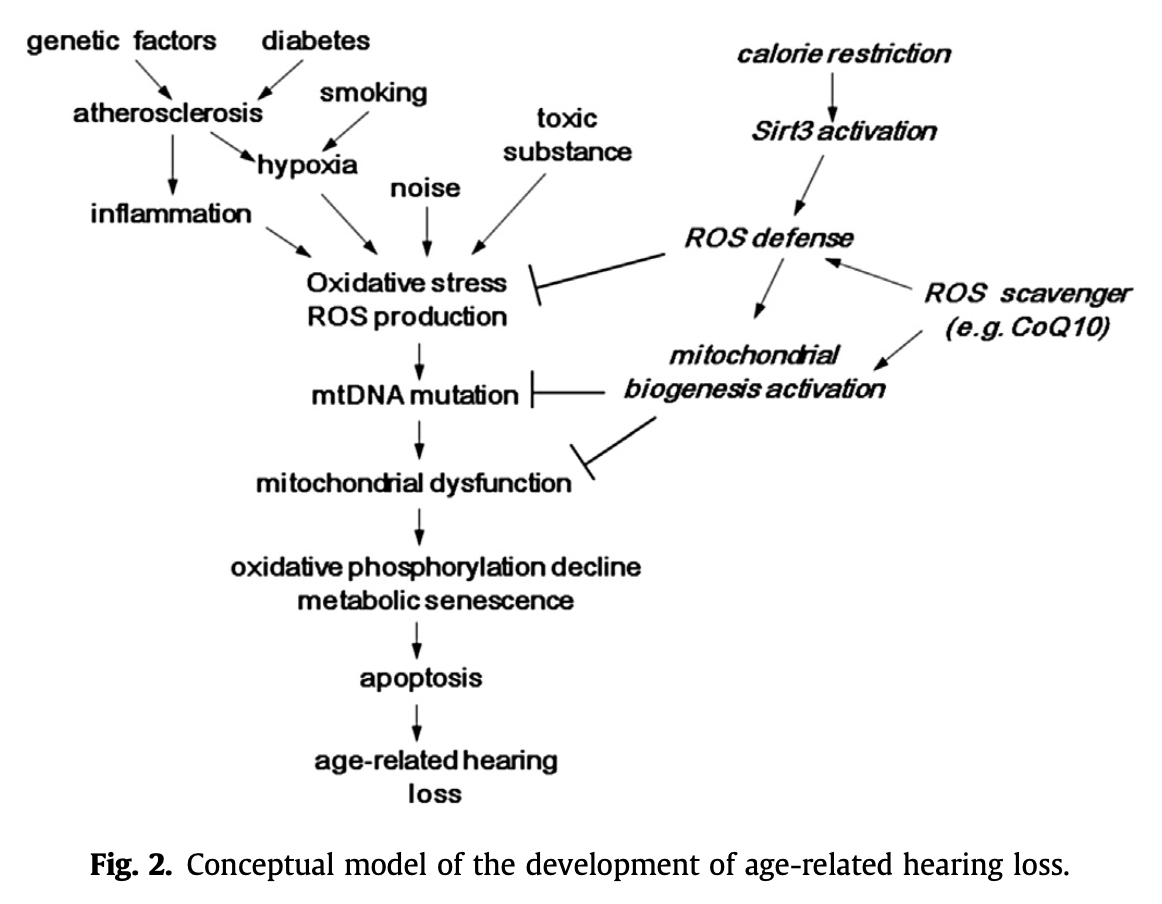
The Figure below, from Yamasoba and colleagues (Yamasoba et al. 2013), sketches out multiple factors that can contribute to presbycusis.
Clinical presentation
Presbycusis tends to present insidiously (Patel and McKinnon 2018), and patients often have difficulty pinpointing when they began noticing difficulty hearing.
Physical examination
Physical examination can include bedside screening tests for hearing loss (Michels et al. 2019), such as finger rub, Weber and Rinne tests, but ultimately formal audiometry is a superior method for characterizing the pattern of hearing loss.
Testing: auditory
Formal audiometry, including pure tone audiometry with word recognition and speech reception thresholds, remains the gold standard for evaluating hearing and corroborating a diagnosis of presbycusis.
Presbycusis initially affects predominantly high frequencies, but over time will eventually also involve the middle frequencies, and then the low frequencies.
Testing: other
As the genetic contributions to presbycusis become clarified, genetic testing may take on an increasing role in diagnosis and informing management decisions.
Imaging
Imaging is not required to secure a diagnosis of presbycusis. However, unexpected findings (such as significant asymmetry in hearing) during a workup for presbycusis may suggest that imaging is indicated.
Histopathology
As mentioned in the section above on the pathophysiologic mechanism of disease, studies (including histopathological works) have demonstrated changes at all levels of the auditory system.
Differential diagnosis
Not all hearing loss in elderly individuals is due to age alone. Clinicians should have a low threshold for suspecting other diagnoses if the history is atypical (such as abrupt onset, rapidly progressive symptoms, presence of significant disequilibrium, or use of ototoxic medications), or if audiometric findings are incompatible (such as a clear asymmetry in hearing, or hearing loss predominantly in the low frequencies).
Treatment
Patients who are receptive to amplification have several treatment options (Michels et al. 2019), including hearing aids, osseointegrated auditory implants and cochlear implants (Patel and McKinnon 2018), which we discuss elsewhere. By the point at which a patient may be considering these options, care should be supervised by an audiologist.
Other therapeutic modalities being investigated include gene therapy, and the use of stem cells. These remain experimental.
Prognosis
Presbycusis is generally slowly progressive. There is no curative or arrestive therapy.
References
Bowl MR, Dawson SJ (2019) Age-Related Hearing Loss. Cold Spring Harb Perspect Med 9. doi: 10.1101/cshperspect.a033217
Collins JG (1997) Prevalence of selected chronic conditions: United States, 1990-1992. Vital Health Stat 10: 1-89.
Elliott KL, Fritzsch B, Yamoah EN, Zine A (2022) Age-Related Hearing Loss: Sensory and Neural Etiology and Their Interdependence. Front Aging Neurosci 14: 814528. doi: 10.3389/fnagi.2022.814528
Michels TC, Duffy MT, Rogers DJ (2019) Hearing Loss in Adults: Differential Diagnosis and Treatment. Am Fam Physician 100: 98-108.
Patel R, McKinnon BJ (2018) Hearing Loss in the Elderly. Clin Geriatr Med 34: 163-174. doi: 10.1016/j.cger.2018.01.001
Wells HRR, Newman TA, Williams FMK (2020) Genetics of age-related hearing loss. J Neurosci Res 98: 1698-1704. doi: 10.1002/jnr.24549
Yamasoba T, Lin FR, Someya S, Kashio A, Sakamoto T, Kondo K (2013) Current concepts in age-related hearing loss: epidemiology and mechanistic pathways. Hear Res 303: 30-8. doi: 10.1016/j.heares.2013.01.021
![]()