By Marcello Cherchi, MD PhD
For patients
Auditory-evoked brainstem responses (ABRs) test some of the hearing pathways in the ear and brainstem. The test may be performed by an audiologist or technician. During this test you are seated or lying down; you will have an earbud insert placed in one ear at a time; you will hear a series of clicks over several minutes. The test is not uncomfortable. The test takes 30 – 60 minutes. If you have earwax in your ear, this should be removed before the test; there are otherwise no special preparations for the test. There are no specific instructions for what to do after the test.
For clinicians
Overview
Auditory-evoked brainstem responses (ABRs), also called brainstem auditory-evoked responses (BAER), are a far-field short-latency evoked potential test that assesses synaptic transmission at various points along the ascending auditory pathway from the cochlea through the medial geniculate nucleus, and the results are sensitive to lesions at any point along that pathway. It is sometimes helpful in the diagnosis of central auditory processing disorders and auditory neuropathy.
Introduction
In 1970 Don Jewett, Michael Romano and John Williston published, “Human auditory evoked potentials: possible brain stem components detected on the scalp” (Jewett et al. 1970). The next year Jewett and Williston more neutrally referred to these responses as, “Auditory-evoked far fields averaged from the scalp of humans” (Jewett and Williston 1971), yet designations confusingly including the word “brainstem” became entrenched in the literature, “even though they are not generated entirely within the brainstem” (Legatt 2015). Thus we are stuck with nomenclature such as “auditory-evoked brainstem responses” (ABRs), “brainstem auditory-evoked responses” (BAERs), and “brainstem auditory evoked potentials” (BAEPs). In this section we shall use “ABRs” for convenience.
ABRs are a far-field short-latency evoked potential test that assesses synaptic transmission at various points along the ascending auditory pathway.
Physiology and neuroanatomy
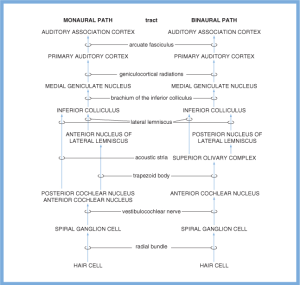
The points of synaptic transmission in the ascending auditory pathways are schematically depicted in the Figure below, from (Haines 2006).
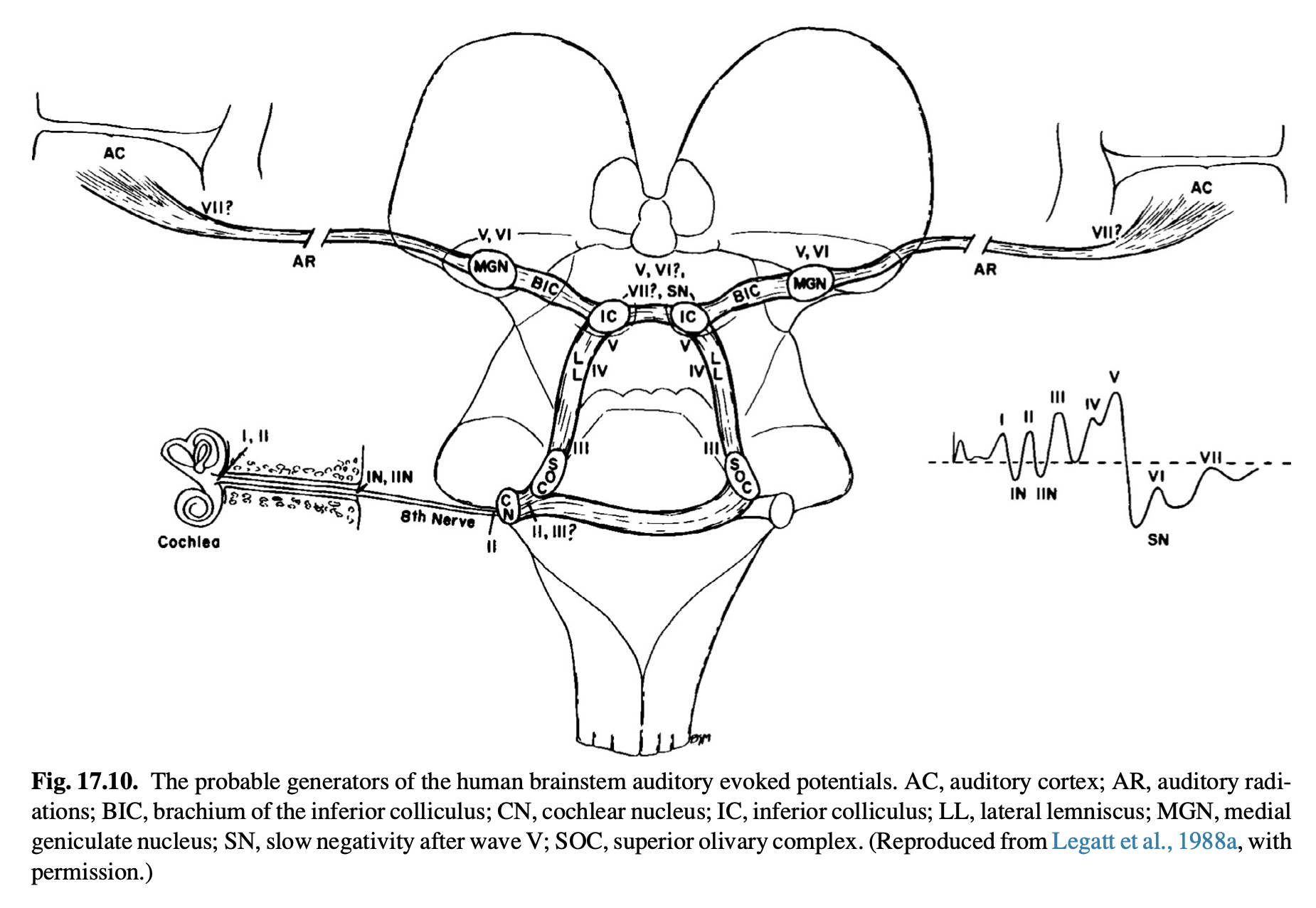
An anatomical depiction of these pathways is shown in the Figure below, from Legatt (Legatt 2015) after Legatt (Legatt et al. 1988).
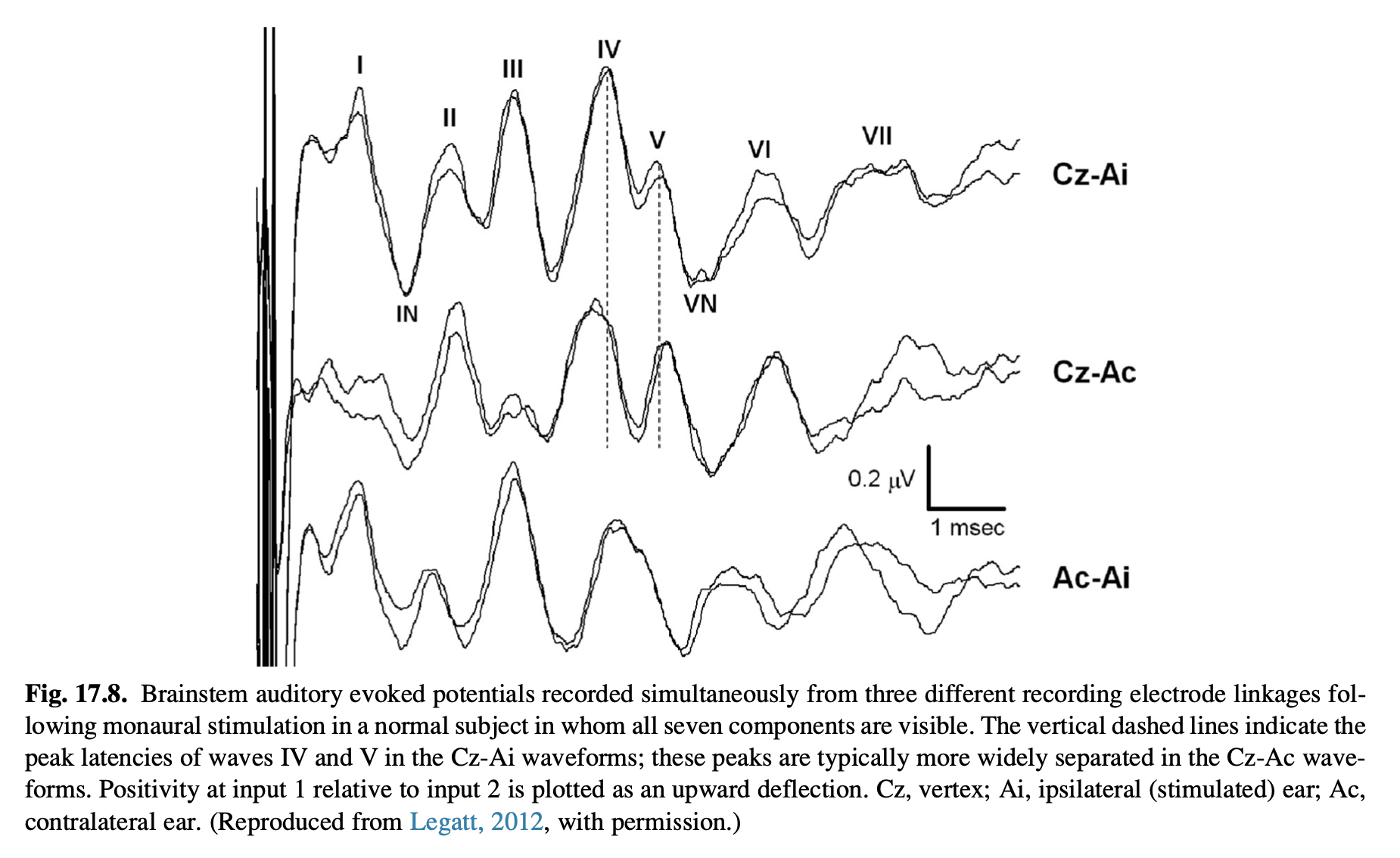
Sample ABR waveforms are shown in the Figure below, from Legatt (Legatt 2015) after Legatt (Legatt 2012).
Wave I is confidently known to arise in the cochlea; the anatomical origins of the remaining waves is less certain (Davies 2016). In summary, from Legatt (Legatt 2015):
- Wave I: Arises from the first volley of action potentials in the distal portion auditory nerve (spiral ganglion).
- Wave II: Arises from synaptic transmission in the cochlear nucleus (pontomedullary junction).
- Wave III: Arises from synaptic transmission in the superior olivary complex (inferior pons).
- Wave IV: Probably arises from activity in the dorsal and rostral pons immediately caudal to the inferior colliculus, perhaps from synaptic transmission in the nuclei of the lateral lemniscus (mid-pons).
- Wave V: Arises from synaptic transmission in the inferior colliculus (tectal plate of the dorsal midbrain).
- Waves VI and VII: Probably reflect activity in the medial geniculate nucleus (thalamus).
Note that ABRs are a short-latency response, occurring within 8 msec of the acoustic stimulus. This is different from the middle-latency responses (8 – 50 msec) that probably reflect activity in the thalamus and perhaps the cerebral cortex, and the long-latency responses (50 – 300 msec) that reflect activity of the cerebral cortex (Picton et al. 1974).
Equipment needed
ABRs are recorded using commercially available evoked response equipment.
How to perform the test
The acoustic stimulus used for ABRs is as follows:
“BAEPs are most commonly elicited by brief acoustic click stimuli, produced by delivering monophasic square pulses of 100 ms duration to the electromechanical transducers at a rate of approximately 10 Hz” (Legatt 2015).
Davies summarizes as follows:
“In the neuro-otology clinic, ABRs with stimulus intensity of 90 or 100 dB are recorded both ipsi- and contralaterally. Measurements are made of the absolute latencies of the waveforms and the inter- wave latencies, identifying any abnormalities. Interaural wave latencies and interwave intervals are compared.” (Davies 2016).
What this test assesses
In theory, ABRs assess the efficacy and timing of neural transmission along the ascending auditory pathways from the cochlea to the medial geniculate nucleus. Lesions along this pathway can manifest as absences (or reduced amplitudes) and/or delayed latencies of the various waveforms of the ABR.
How to interpret the test results
Davies summarizes as follows:
“Prolongation of the I–III interval can be seen in auditory nerve and cochlear nucleus pathology. Prolongation of the III–V interval is usually indicated when pathology is sited above the level of the cochlear nucleus, while absent IV and/or V waves are found in cases with involvement of the mid-upper pons” (Davies 2016).
Contraindications
Patients with injuries of the external ear, or who have otitis externa, may be unable to tolerate the earbud inserts required for performing ABRs.
Pitfalls
The acoustic stimulus generator can malfunction. The earbud inserts can burn out. As with other surface electrode evoked potential tests, inadequately cleaned skin can interfere with results. Electrical interference from nearby devices can also pose a problem.
When is the test indicated
It is reasonable to check ABRs in patients complaining of hearing loss, or who have evidence of sensorineural hearing loss on audiometry.
Diseases that may be diagnosed by this test
Disorders of the cochlea and auditory nerve can manifest as abnormalities of ABR waves I – III.
Brainstem lesions and central auditory processing disorders can manifest as abnormalities of ABR waves IV – VII.
Assessment of ABRs plays a role in cases of suspected auditory neuropathy. For patients in whom audiometry shows poor word recognition and speech perception thresholds out of proportion to performance on pure tone testing, a diagnosis of auditory neuropathy is supported if ABRs are abnormal yet otoacoustic emissions are preserved.
For years it was debated whether it was possible to diagnose a vestibular schwannoma on the basis of ABR abnormalities. In contemporary practice ABR, like audiometry, is viewed largely as a screening test for vestibular schwannoma; confirmation of the diagnosis comes from MRI of the internal auditory canals without and with contrast.
References
Davies RA (2016) Audiometry and other hearing tests. Handb Clin Neurol 137: 157-76. doi: 10.1016/B978-0-444-63437-5.00011-X
Haines DE (2006) Fundamental neuroscience, 3rd edn. Churchill Livingstone, Philadelphia
Jewett DL, Romano MN, Williston JS (1970) Human auditory evoked potentials: possible brain stem components detected on the scalp. Science 167: 1517-8. doi: 10.1126/science.167.3924.1517
Jewett DL, Williston JS (1971) Auditory-evoked far fields averaged from the scalp of humans. Brain 94: 681-96. doi: 10.1093/brain/94.4.681
Legatt AD (2012) Brainstem Auditory Evoked Potentials: Methodology, Interpretation, and Clinical Application. In: Aminoff MJ (ed) Aminoff’s Electrodiagnosis in Clinical Neurology, 6 edn. Churchil Livingstone, New York, pp 519-552
Legatt AD (2015) Electrophysiologic auditory tests. Handb Clin Neurol 129: 289-311. doi: 10.1016/B978-0-444-62630-1.00017-2
Legatt AD, Arezzo JC, Vaughan HG, Jr. (1988) The anatomic and physiologic bases of brain stem auditory evoked potentials. Neurol Clin 6: 681-704.
Picton TW, Hillyard SA, Krausz HI, Galambos R (1974) Human auditory evoked potentials. I. Evaluation of components. Electroencephalogr Clin Neurophysiol 36: 179-90. doi: 10.1016/0013-4694(74)90155-2
![]()