By Marcello Cherchi, MD PhD
For patients
Lindsay-Hemenway syndrome (LHS) is a sequence of two other conditions that cause disequilibrium. It starts with vestibular neuritis (VN), which is then followed by benign paroxysmal positional vertigo (BPPV).
For clinicians
Overview
Lindsay-Hemenway syndrome (LHS) is currently thought to reflect a sequence of two pathologies, namely, vestibular neuritis (VN) followed by ipsilateral benign paroxysmal positional vertigo (BPPV). Physical examination findings and instrumented test results are compatible with those diagnoses. Patients with LHS tend to have a poorer prognosis in that symptoms are more prolonged, more vestibular rehabilitation therapy (VRT) is required, and the rate of recurrence of BPPV is higher.
Introduction
Lindsay-Hemenway syndrome (LHS) was originally described as a vascular insult of the labyrinth resulting in vestibular weakness, followed by positional vertigo. This hypothesized vascular mechanism has come into question, and most investigators now instead view this as vestibular neuritis (VN) followed by ipsilateral benign paroxysmal positional vertigo (BPPV). The physical examination findings, and results from audio-vestibular testing, correspond to those two pathologies; specifically, instrumented vestibular testing shows evidence of a unilateral vestibular weakness (either on caloric testing, or cervical vestibular evoked myogenic potentials, or ocular vestibular evoked myogenic potentials, or video head impulse testing, or some combination thereof), and ocular motor examination shows nystagmus compatible with benign paroxysmal positional vertigo (usually of the posterior canal).
Historical background
Dr. John Ralston Lindsay (1898-1981) was a Canadian otolaryngologist (Marion and Matz 1982; Mhoon et al. 1983; Schuknecht 1983) who served as the head of otolaryngology at the University of Chicago from 1930 through 1966 (Shambaugh 1967). Dr. William Garth Hemenway (1921 – 2007), also a Canadian, did residency in otolaryngology at the University of Chicago while Dr. Lindsay was head of that department.
|
Figure : Dr. John Ralston Lindsay (1898 – 1981). From Shambaugh (Shambaugh 1967). This photo was touched-up using Gemini AI. |
Figure : Dr. William Garth Hemenway (1921 – 2007). From https://media.gettyimages.com/id/837094244/photo/denver-post-archives.jpg?s=1024×1024&w=gi&k=20&c=AX3LgLNvo-PEVftQo0f7aV9UNmwaUY_v-gbyhXWPg0o= (accessed 12/29/2025). |

{kind=link}
In 1956 Dr. Lindsay and Dr. Hemenway reported the cases of 7 patients (Hemenway and Lindsay 1956), each of whom suffered the abrupt-onset of severe disequilibrium that left them bed-bound for days before improving, but was followed by briefer, milder bouts of “positional vertigo.” Of these seven cases, some (though not all) exhibited spontaneous nystagmus and some (though not all) exhibited unilateral caloric weakness; in those with both, the fast component of the spontaneous nystagmus beat away from the caloric weakness. Some (though not all) of the patients also had positional nystagmus.
Epidemiology
There is a paucity of literature on Lindsay-Hemenway syndrome (LHS). However, if (as will be discussed below) these are cases of vestibular neuritis (VN) followed by benign paroxysmal positional vertigo (BPPV), then the epidemiology should be some subset of patients with vestibular neuritis (which is one of the most common vestibular diagnoses).
Anghel and colleagues (Anghel et al. 2020) cite studies reporting that 16.3% of cases of BPPV are related to LHS. They further state that it is more common in patients over the age of 60 years, but with a range of 45 – 78 years.
Genetics
There are no published studies of genetics in patients with Lindsay-Hemenway syndrome.
Pathophysiological mechanism of disease
Of the seven cases originally reported by Lindsay and Hemenway (Hemenway and Lindsay 1956), only the first case came to autopsy, which reported that the right side (which was the side with caloric weakness, and spontaneous nystagmus contraversive to that caloric weakness) showed:
“Definite histopathologic changes. These consisted as follows: There was in the internal auditory meatus a mass of convoluted vessels varying in size from one relatively large vessel to many very small vascular channels many of which lay closely related to and within the vestibular nerve at the ganglion of Scarpa” (Hemenway and Lindsay 1956).
Lindsay and Hemenway summarized their seven cases as follows:
“Sudden or rapid partial destruction of one labyrinth has frequently been observed to cause postural vertigo. At the onset the vertigo is continuous but as the symptom decreases it becomes postural in character and may persist for periods of time varying from a few weeks to two or three years” (Hemenway and Lindsay 1956).
Lindsay and Hemenway concluded that these cases were due to “vascular accidents” (their term) and specifically either due to “hemorrhage” or “vascular occlusion” — in other words, they hypothesized a hemorrhagic or ischemic infarction of the labyrinth. Note that the histopathological evidence for this was based on a single case (their first patient in their series of seven).
Although some contemporary investigators continue to embrace this vascular hypothesis (Anghel et al. 2020; Gkoritsa 2016), work by Waissbluth and colleagues (Waissbluth et al. 2023) brought into question the hypothesized mechanism of infarction, as they found that patients with Lindsay-Hemenway syndrome did not have greater vascular risk factors compared to controls. Given that vascular labyrinthine insults are otherwise uncommon, we find it overall implausible that cases construed as Lindsay-Hemenway syndrome are of vascular etiology.
In view of these considerations (and despite Lindsay and Hemenway’s vascular hypothesis) when contemporary clinicians are presented with patient histories similar to those described by Lindsay and Hemenway, most would organize these as cases of acute vestibular syndrome (probably vestibular neuritis) followed by benign paroxysmal positional vertigo (BPPV), a sequence which is encountered rather commonly in routine clinical practice.
Moreover, given that the sequence of events is an acute vestibular syndrome followed by positional vertigo (rather than the reverse), it is plausible (though not proven) that the vestibular neuritis increases the risk for subsequent benign paroxysmal positional vertigo.
The modest literature on this topic includes observations of significant vestibular weakness (usually caloric weakness) in the affected ear yet posterior canal BPPV in that same ear (Casani et al. 2018). This is not a contradiction; most (though not all) cases of vestibular neuritis involve the superior division of the vestibular nerve, and disruption of this division may affect trophic function to other structures it innervates, including the utricle, which in turn may eventually make that utricle more vulnerable to loss of its otoliths. Those otoliths may eventually cause BPPV, of which the most common variant involves the posterior canal, which is innervated by the inferior division of the vestibular nerve (the division often unaffected by vestibular neuritis), and thus posterior canal BPPV can still manifest clinically (despite the caloric weakness of the superior division of the vestibular nerve).
Practically, it is well-established that vestibular neuritis (VN) can affect any combination of fibers in the vestibular nerve (Cherchi and Yacovino 2021), and our own experience is that BPPV occurring after VN can involve any canal. Thus, while LHS may reflect the statistics of vestibular neuritis (usually involving the superior division of the vestibular nerve) and BPPV (usually involving the posterior canal); these are only tendencies. In practice, any combination of vestibular weakness and ipsilateral BPPV can be encountered.
Clinical presentation
The presentation of Lindsay-Hemenway syndrome is an acute vestibular syndrome that is severe and protracted (clinically identical to vestibular neuritis) followed by positional vertigo (clinically identical to benign paroxysmal positional vertigo).
Physical examination
Patients with unilateral vestibular weakness, particularly closer to the onset of illness, will have corresponding physical examination findings, such as difficulty maintaining unsighted tandem Romberg stance.
Ocular motor examination
Infrared video oculography may identify:
- Findings compatible with benign paroxysmal positional vertigo (BPPV), usually (but not exclusively) the posterior canal.
- Findings compatible with unilateral vestibular weakness (ipsilateral to the BPPV), such as spontaneous unidirectional nystagmus (usually horizontal, sometimes with a modest torsional component), or unidirectional horizontal nystagmus that can be elicited by provocative maneuvers (e.g., neck vibration, head shaking).
Testing: auditory
Most literature reports that hearing is normal (or at least age-appropriate) in patients with Lindsay-Hemenway syndrome. Curiously, in Lindsay and Hemenway’s first patient (with right-sided pathology), they present an audiogram showing asymmetrical hearing loss (greater on the right side at 125 Hz – 4 kHz), as displayed in the Figure below.
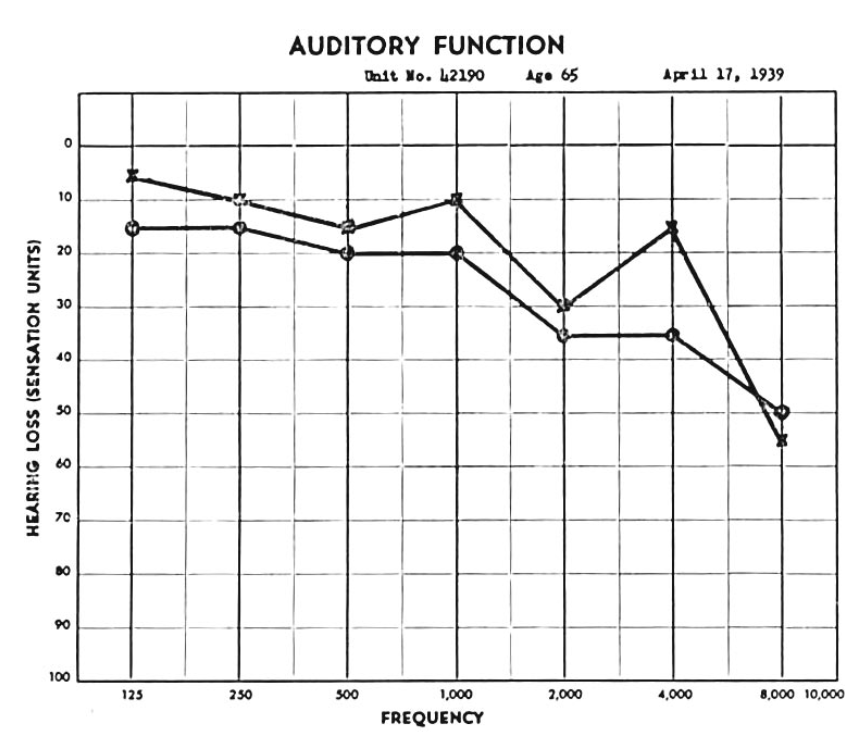
Figure: Audiogram from the first patient in the series reported by Lindsay and Hemenway (Hemenway and Lindsay 1956), showing that pure tone hearing was 5 – 20 dB weaker on the right (the side with vestibular weakness and benign paroxysmal positional vertigo) than on the left at 125 Hz – 4 kHz.
Testing: vestibular
Instrumented vestibular testing should show evidence of:
- Benign paroxysmal positional vertigo (BPPV).
- Unilateral vestibular weakness ipsilateral to the BPPV, such as:
- Caloric weakness (Anghel et al. 2020).
- Video head impulse testing (vHIT) will show low gain and compensatory saccades (Casani et al. 2018).
- Weakness on cervical vestibular evoked myogenic potentials (cVEMPs) and/or ocular vestibular evoked myogenic potentials (oVEMPs) (Casani et al. 2018).
The Figures below show examples of each finding.
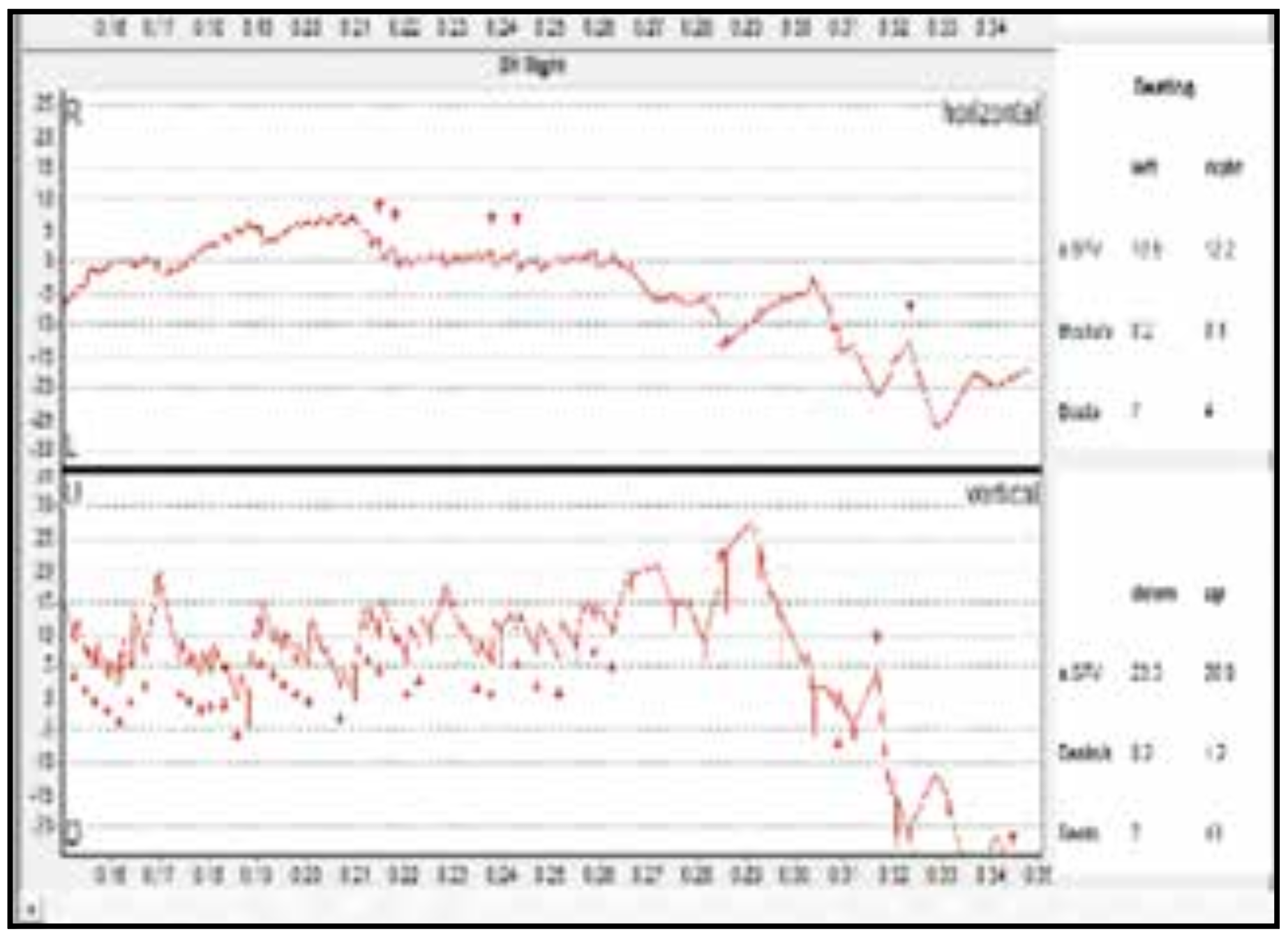
Figure: Results of videonystagmography (VNG) in the right-sided Dix-Hallpike position in a patient with right-sided Lindsay-Hemenway syndrome reported by Anghel and colleagues (Anghel et al. 2020). The figure in the original article is of poor quality; the authors of the paper interpret this as showing up beat and right torsional nystagmus, compatible with right-sided posterior canal benign paroxysmal positional vertigo (BPPV).
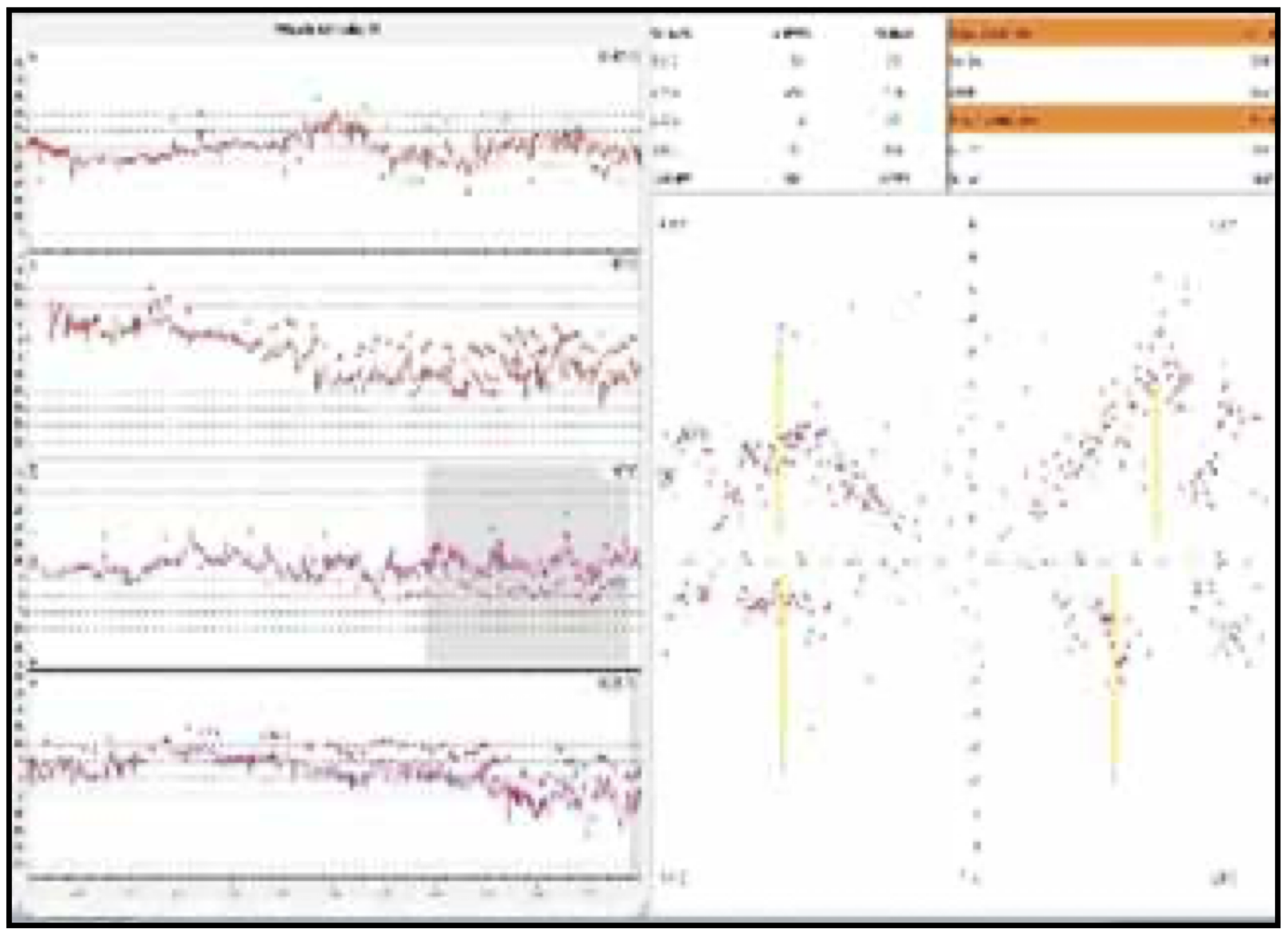
Figure: Results of caloric testing in a patient with right-sided Lindsay-Hemenway syndrome reported by Anghel and colleagues (Anghel et al. 2020). The figure in the original article is of poor quality, but shows right-sided caloric weakness.
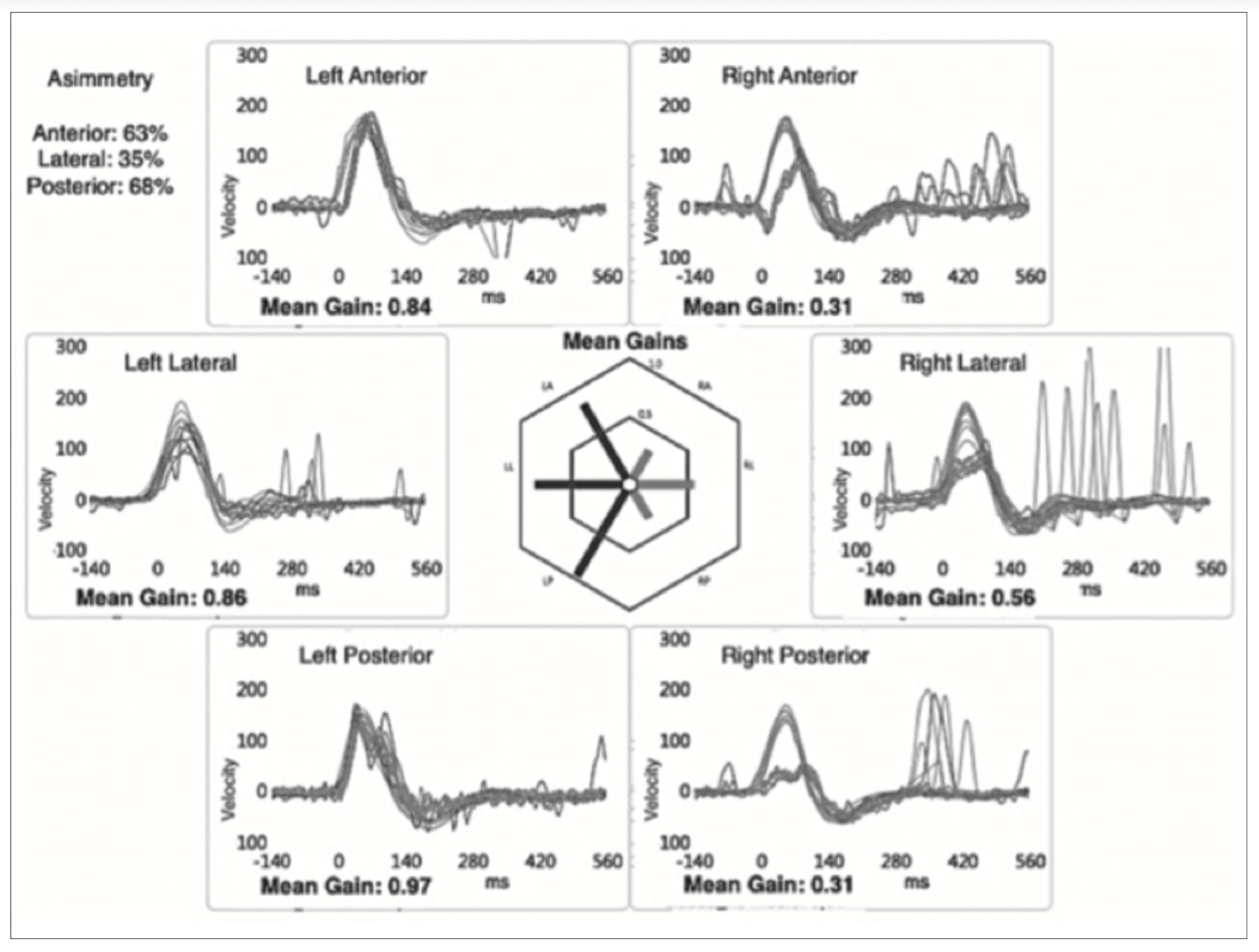
Figure: Video head impulse testing (vHIT) from a case of right-sided Lindsay-Hemenway syndrome reported by Casani and colleagues (Casani et al. 2018), showing low gain with overt compensatory saccades in all canals on the right side.
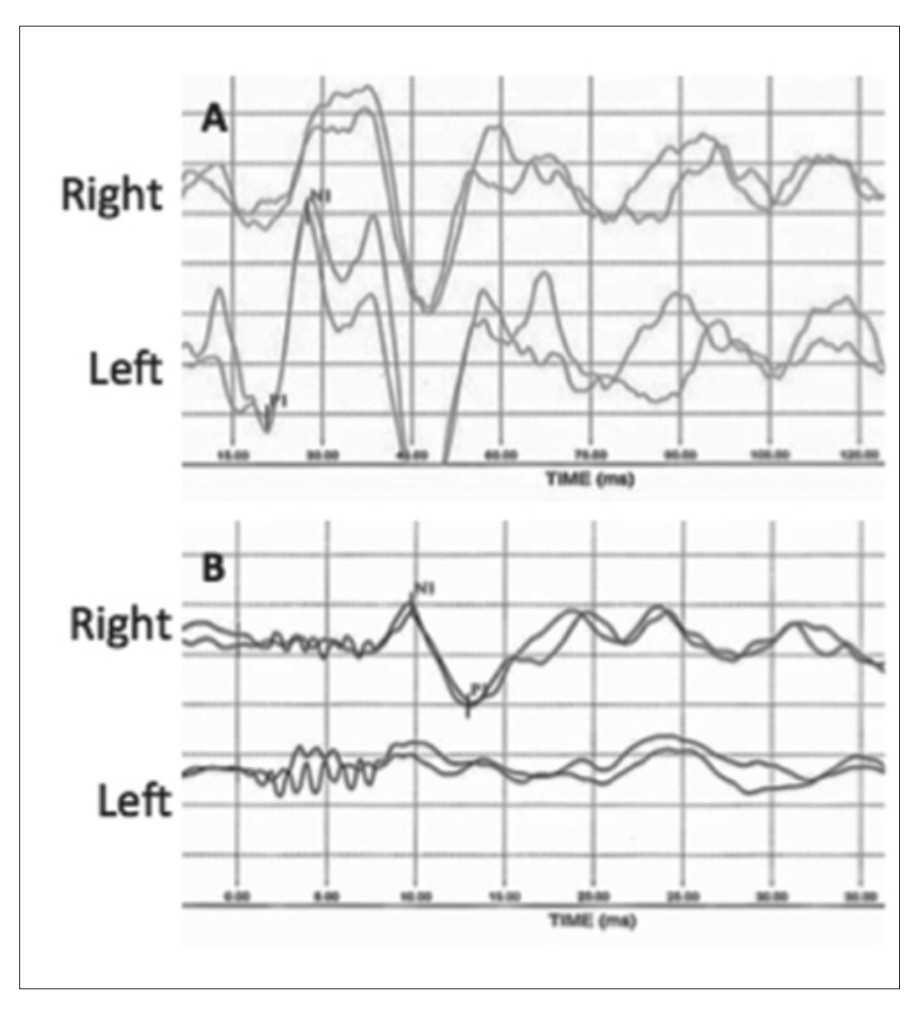
Figure: Air-conducted cervical vestibular evoked myogenic potentials (cVEMPs) and bone-conducted ocular vestibular evoked myogenic potentials (oVEMPs) in a case of right-sided Lindsay-Hemenway syndrome reported by Casani and colleagues (Casani et al. 2018). The cVEMP responses were absent on the right side (reflecting a right-sided vestibular weakness). The oVEMP responses were absent on the left side (reflecting a right-sided vestibular weakness).
Imaging
Imaging is usually not contributory in establishing a diagnosis of Lindsay-Hemenway syndrome, except insofar as it may help exclude competing diagnoses.
Histopathology
The only case with published histopathology is the first patient reported by Lindsay and Hemenway (Hemenway and Lindsay 1956).
Differential diagnosis
The differential diagnosis is the combined differential of vestibular neuritis (VN) and benign paroxysmal positional vertigo (BPPV).
Management
The standard of care for vestibular neuritis (VN) and benign paroxysmal positional vertigo (BPPV) is appropriately targeted vestibular rehabilitation therapy (VRT).
Prognosis
Chacchi and colleagues (Chacchi et al. 2025) longitudinally studied 98 patients, including 36 with Lindsay-Hemenway syndrome (LHS), 30 with isolated AUVP (acute unilateral vestibulopathy), and 32 with isolated posterior canal BPPV. They reported that patients with LHS experienced “more severe vestibular dysfunction, slower recovery, and more persistent BPPV than [unilateral] isolated AUVP or idiopathic PSC [posterior semicircular canal] BPPV” (Chacchi et al. 2025). Balatsouras and colleagues (Balatsouras et al. 2014) compared (1) 22 patients whose BPPV occurred within 12 weeks of vestibular neuritis (although they did not specifically designate such cases as Lindsay-Hemenway syndrome), and (2) 284 patients with idiopathic BPPV, and reported that the rate of recurrence of BPPV in the former group was higher. Whether the poorer prognosis in LHS is simply the additive result of two separate pathologies, or whether the acute vestibular syndrome and BPPV are synergistic, is unclear.
References
Anghel A, Badea C, Musat G (2020) Lindsay-Hemenway Syndrome: Review of the literature and case report. Romanian Journal of Rhinology 10: 13-18. doi: 10.2478/rjr-2020-0003
Balatsouras DG, Koukoutsis G, Ganelis P, Economou NC, Moukos A, Aspris A, Katotomichelakis M (2014) Benign paroxysmal positional vertigo secondary to vestibular neuritis. Eur Arch Otorhinolaryngol 271: 919-24. doi: 10.1007/s00405-013-2484-2
Casani AP, Cerchiai N, Navari E (2018) Paroxysmal positional vertigo despite complete vestibular impairment: the role of instrumental assessment. Acta Otorhinolaryngol Ital 38: 563-568. doi: 10.14639/0392-100X-1549
Chacchi PM, Touma GC, Perez LC, Batuecas-Caletrio A, Sanz EM (2025) Lindsay-Hemenway Syndrome, Acute Vertigo Followed by BPPV: A Prospective Comparative Study. Laryngoscope. doi: 10.1002/lary.70324
Cherchi M, Yacovino DA (2021) Histology and neuroanatomy suggest a unified mechanism to explain the distribution of lesion patterns in acute vestibular neuropathy. Experimental Brain Research 239: 1395–1399. doi: 10.1007/s00221-021-06094-9
Gkoritsa EZ (2016) The Lyndsay-Hemenway syndrome: two case reports, review and comments. J Ear Nose Throat Disord 1: 1014.
Hemenway WG, Lindsay JR (1956) Postural vertigo due to unilateral sudden partial loss of vestibular function. Ann Otol Rhinol Laryngol 65: 692-706. doi: 10.1177/000348945606500311
Marion MS, Matz GJ (1982) In memoriam. John R. Lindsay, M.D. 1898-1981. Laryngoscope 92: 462. doi: 10.1288/00005537-198204000-00020
Mhoon EE, Jr., Marion M, Matz GJ (1983) John R. Lindsay, 1898-1981. Ann Otol Rhinol Laryngol Suppl 102: 7.
Schuknecht HF (1983) John R. Lindsay: clinician, teacher, otopathologist. Ann Otol Rhinol Laryngol Suppl 102: 12-6. doi: 10.1177/00034894830921s204
Shambaugh GEJ (1967) Dr. John Lindsay Retires, but Remains Active. Archives of Otolaryngology 85: 237-237. doi: 10.1001/archotol.1967.00760040239001
Waissbluth S, Becker J, Sepúlveda V, Iribarren J, García-Huidobro F (2023) Benign Paroxysmal Positional Vertigo Secondary to Acute Unilateral Peripheral Vestibulopathy: Evaluation of Cardiovascular Risk Factors. The Journal of International Advanced Otology: 28-32. doi: 10.5152/iao.2023.22703
![]()