By Marcello Cherchi, MD PhD
For patients
Basilar invagination is an abnormality in the shape of the bones at the bottom of the skull. This can cause disequilibrium and eye movement abnormalities. Treatment is surgical.
For clinicians
Overview
The phrase “basilar invagination” usually refers to a craniocervical junction abnormality in which the odontoid process ascends excessively. This anatomical configuration can impinge on the medulla and cause a variety of symptoms that localize to the brainstem (usually the medulla) or craniocervical junction.
Basilar invagination sometimes presents with nystagmus (Ridder, Anderson et al. 2015, de Oliveira Filho, Romero et al. 2019), and specifically down beat nystagmus (Yeow and Tjia 1989, Pratiparnawatr, Tiamkao et al. 2000).
Management is surgical decompression.
Case
A patient who carried a diagnosis of basilar invagination was referred to us to be evaluated for chronic, gradually progressive unsteadiness when upright.
On general neurological examination station was characterized by a wide base; gait appeared mildly ataxic; myotatic reflexes were diffusely brisk, with positive Hoffman’s and Troemner’s signs bilaterally, though plantar responses were flexor.
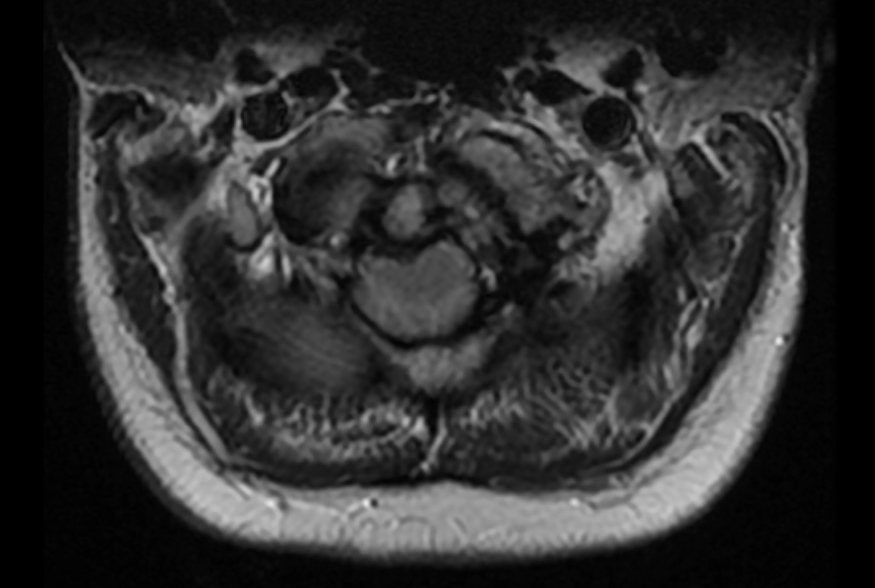
Cervical spine MRI showed that the inferior clivus protruded posteriorly, impinging on the medulla. The cerebellar tonsils descended slightly through the foramen magnum, resulting in crowding at the foramen magnum with no visible cerebrospinal fluid around the cord.
 |
 |
Videonystagmography showed spontaneous down beat nystagmus that dramatically augmented on lateral gaze, as displayed below.
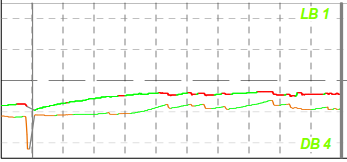
Spontaneous down beat nystagmus on primary position of gaze. |
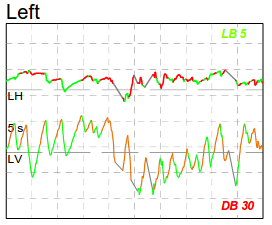
Left gaze significantly augmented the baseline down beat nystagmus. |
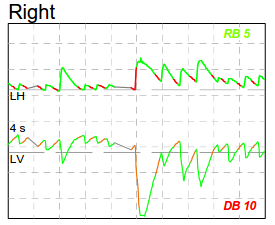
Right gaze significantly augmented the baseline down beat nystagmus. |
A video of this nystagmus is shown below and here.
References
de Oliveira Filho IT, Romero PC, Fontoura EAF, Botelho RV (2019) Chiari malformation and types of basilar invagination with/without syringomyelia. Surg Neurol Int 10: 206. doi: 10.25259/SNI_469_2019
Pratiparnawatr P, Tiamkao S, Tanapaisal C, Kanpittaya J, Jitpimolmard S (2000) Downbeating nystagmus and postural hypotension due to basilar invagination. J Med Assoc Thai 83: 1530-4.
Ridder T, Anderson RC, Hankinson TC (2015) Ventral Decompression in Chiari Malformation, Basilar Invagination, and Related Disorders. Neurosurg Clin N Am 26: 571-8. doi: 10.1016/j.nec.2015.06.011
Yeow YK, Tjia TL (1989) The localizing value of downbeat nystagmus. Singapore Med J 30: 273-6.
![]()