By Marcello Cherchi, MD PhD
For patients
Benign paroxysmal positional vertigo (BPPV) is an inner ear problem that can cause the symptom of disequilibrium. BPPV can affect different parts of the inner ear. The lateral semicircular canal (also called the horizontal semicircular canal) is the second most commonly affected part of the ear in BPPV. It is sometimes difficult to figure out which side (which ear) is affected. Treatment is usually done by a physical therapist using a specific series of maneuvers.
For clinicians
Lateral (also called horizontal) semicircular canal benign paroxysmal positional vertigo (BPPV) is less common than posterior canal BPPV. Estimates in the literature suggest that it accounts for approximately 5% – 10% of cases of BPPV.
The diagnosis of lateral semicircular canal BPPV is secured by observing a specific pattern of eye movements when the patient is in several different positions. The series of positions is sometimes referred to as the “supine roll test,” while some examiners use eponymous designations (Bhattacharyya et al. 2017), after the various investigators who provided early descriptions of the phenomenon (e.g., McClure (McClure 1985), Pagnini (Pagnini et al. 1989)). Essentially, when the patient’s head is directly on its side (i.e., with the sagittal plane oriented horizontally, in parallel with the surface of the earth), nystagmus that is purely horizontal (with respect to the patient’s head) emerges; the nystagmus is either “geotropic” (meaning that the fast phase beats towards the ground) or “apogeotropic” (meaning that the fast phase beats away from the ground). These patterns are sometimes referred to as “direction changing positional nystagmus” (Baloh et al. 1993; McClure 1985), because the direction of the nystagmus depends on the position of the patient’s head with respect to gravity.
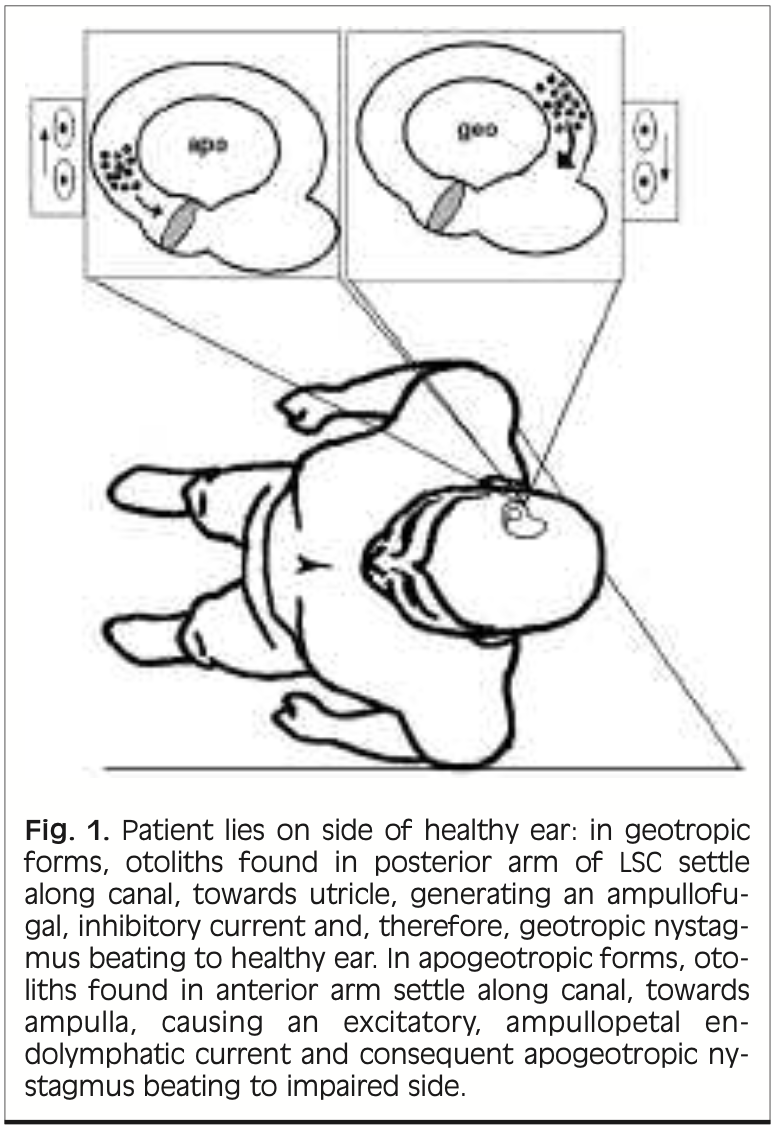
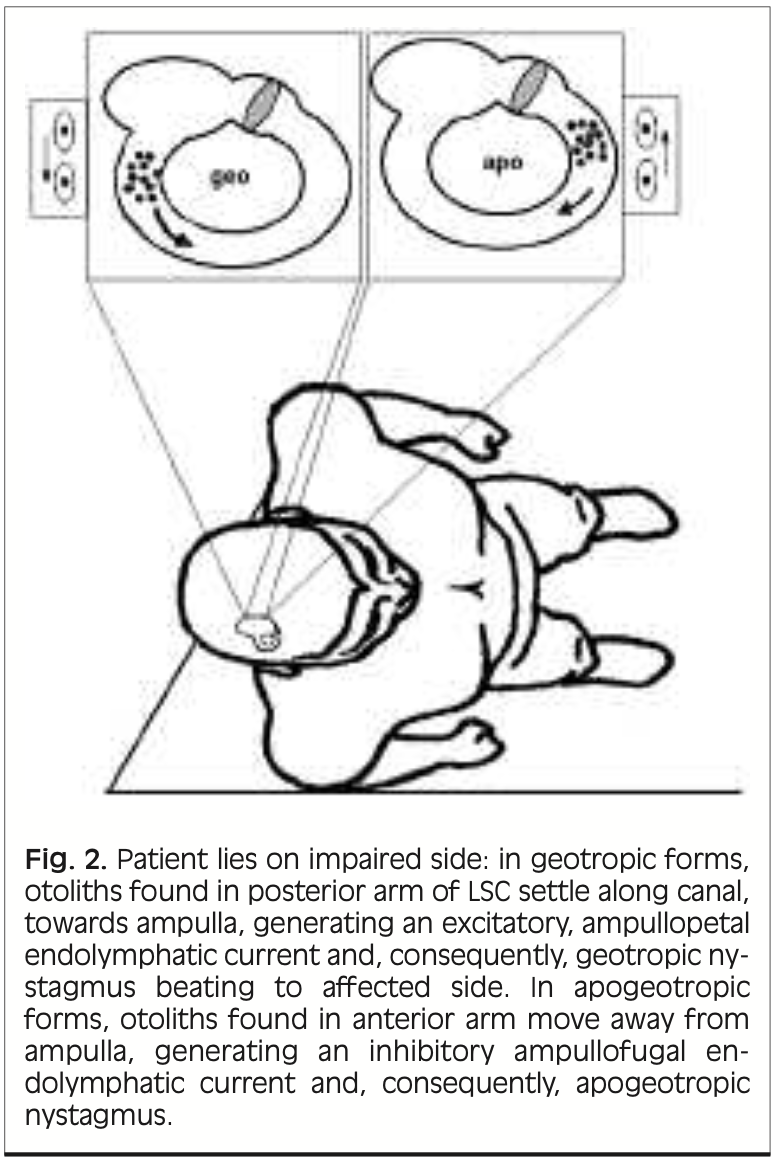
The Figures below, from Asprella Libonati (Asprella Libonati 2005), summarizes the anatomy and physiology of lateral canal BPPV canalolithiasis when the patient is lying on the affected or unaffected side, for geotropic and apogeotropic variants.
 |
 |
To summarize this in tabular format:
|
Geotropic canalolithiasis BPPV. This variant is attributed to free floating particles in the posterior arm (closer to the utricle) of the lateral canal. |
Apogeotropic canalolithiasis BPPV. This variant is attributed to free floating particles in the anterior arm (closer to the ampulla) of the lateral canal. |
|||
|
Patient lying on affected ear |
When the patient is lying on the affected ear, the otoliths will move toward the ampulla (away from the utricle), resulting in an ampullopetal excitatory current and causing a nystagmus beating toward the (now undermost) affected ear (i.e., geotropic). |
|
|
When the patient is lying on the affected ear, the particles will move away from the ampulla (toward the utricle), resulting in an ampullofugal inhibitory endolymphatic current, causing a nystagmus beating toward the (now uppermost) unaffected ear (i.e., apogeotropic). |
|
Patient lying on unaffected ear |
When the patient is lying on the unaffected ear, the otoliths will move away from the ampulla (toward the utricle), resulting in an ampullofugal inhibitory endolymphatic current, causing a nystagmus beating to the (now undermost) unaffected ear (i.e., geotropic). |
|
|
When the patient is lying on the unaffected ear, the particles will move toward the ampulla (away from the utricle), resulting in an ampullopetal excitatory endolymphatic current, causing a nystagmus beating toward the (now uppermost) affected ear (i.e., apogeotropic). |
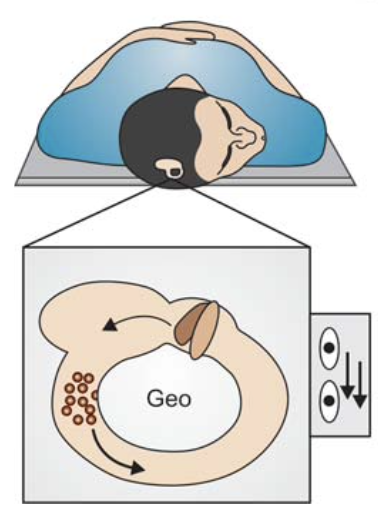
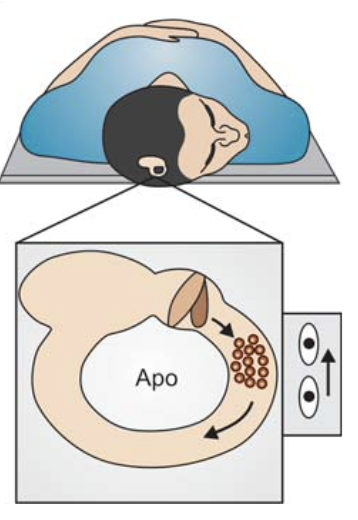
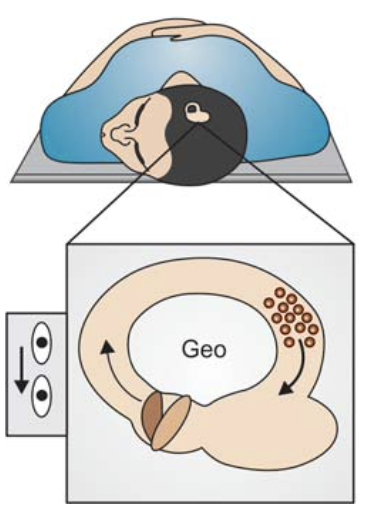
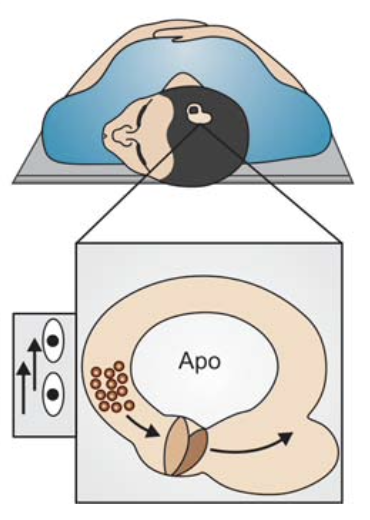
Table : Tabular summary of lateral canal BPPV canalolithiasis, geotropic and apogeotropic variants, with patient lying on affected or unaffected side. The figures are excerpted from Asprella Libonati (Asprella Libonati 2012).
Because both lateral semicircular canals lie in the same plane, either side can produce the same pattern of eye movement abnormalities on the supine roll test.
Several diagnostic maneuvers have been proposed for localizing (lateralizing) the affected side in lateral canal BPPV. One of the better studied techniques, originally proposed by Yon-Hoon Choung (Choung et al. 2006), is the “bow and lean test” (Choi et al. 2018; Kim et al. 2016; Kim et al. 2023; Koju et al. 2022; Lee et al. 2010; Marcelli 2016).
The key insight underlying the “bow and lean test” is that for lateral canal canalolithiasis:
- Tilting the head forward (thereby orienting the lateral canals more vertically with respect to gravity, and with the ampullary end lower than the crural end of the canal), gravity will pull the otoliths on a given side toward the ampulla, and this ampullopetal movement comprises an excitatory stimulus that will drive the slow phase of the eyes away from the affected side, then the fast phase toward the affected side.
- Conversely, tilting the head backward (thereby orienting the lateral canals more vertically with respect to gravity, and with the ampullary end higher than the crural end of the canal), gravity will pull the otoiths on a given side away from the ampulla, and this ampullofugal movement comprises an inhibitory stimulus that will drive the slow phase of the eyes toward the affected side, then the fast phase away from the affected side.
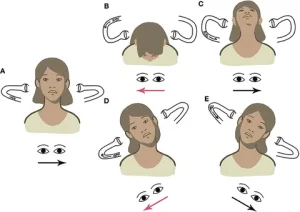
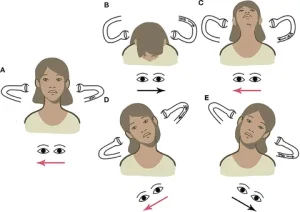
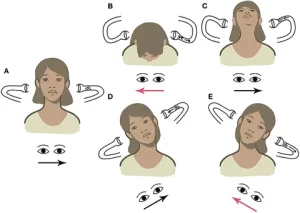
In short, for lateral canal canalolithiasis, tilting the head forward generates horizontal nystagmus whose fast phase beats toward the affected side, while tilting the head backward generates horizontal nystagmus whose fast phase beats away from the affected side. This is demonstrated in the Figure below from Choung and colleagues.
We summarize the underlying physiology for lateral canal canalolithiasis in the Figure below, which depicts the lateral semicircular canals as if viewed from above the patient’s head (nose down).

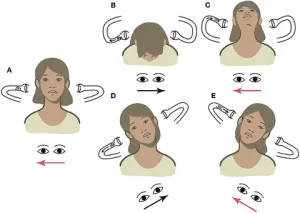
However, the situation is more complex due to the possibility of cupulolithiasis (as opposed to canalolithiasis), which may result in exactly the reverse pattern of nystagmus, as shown in the Figure below from Choung and colleagues.
One proposal for distinguishing between the canalolithiasis and cupulolithiasis variants of lateral canal benign paroxysmal positional vertigo (BPPV) is the finding of “pseudo-spontaneous nystagmus” when the patient is upright. The idea underlying this observation is that when a patient is seated upright, the plane of the lateral canal is actually not parallel with the earth’s surface; rather, it is tilted slightly (30˚) backward, such that the ampullary end is higher than the crural end; thus, in this position, if there are otoliths in the canal, they are more likely to move (slowly) away from the ampulla, and this ampullofugal movement is an inhibitory stimulus which should generate nystagmus in which the slow phase is toward the affected side, and the fast phase is directed away from the affected side.
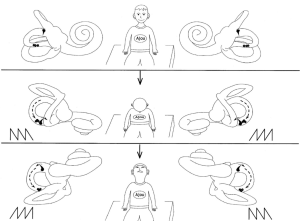
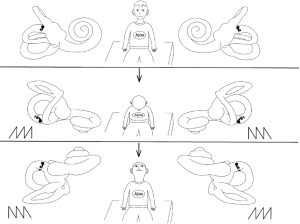
Some studies propose combining the observation of “pseudo-spontaneous nystagmus” with the results of the “bow-and-lean” test, as shown in the Table below, whose figures are drawn from Martellucci and colleagues (Martellucci et al. 2020).
|
Right side affected If geotropic (crural segment):
If apogeotropic (ampullary segment):
|
Left side affected If geotropic (crural segment):
If apogeotropic (ampullary segment):
|
|
|
Geotropic (otoliths at crural segment). Lateral lean causes geotropic nystagmus (by definition). |
 |
 |
|
Apogeotropic (otoliths at ampullary segment). Lateral lean causes apogeotropic nystagmus (by definition). |
 |
 |
A final diagnostic complication is posed by cases of bilateral lateral canal BPPV (Kumar et al. 2023). For the lateral semicircular canals Ewald’s second law states that an ampullopetal (excitatory) stimulus is stronger than an ampullofugal (inhibitory) stimulus, so by this principle, if one lateral canal is more affected (e.g., has a greater number of loose otoliths) than the other, then the influence of that side will predominante during the “bow” (forward tilt) part of the ”bow and lean” test, and the nystagmus resulting from that position should beat toward the affected side. However, if the lateral canals are symmetrically affected, then such determination would be impossible because forward tilting would generate equally strong but oppositely directed nystagmus — they would “cancel each other out.”
With such considerations in mind, while these theoretical diagnostic frameworks have merit, in clinical practice it is often not possible to determine confidently the side affected side in lateral canal BPPV. Physical examination alone can generally diagnose lateral semicircular canal BPPV (because it is usually straightforward to distinguish geotropic and apogeotropic patterns), but may not be able to determine the affected side. Consequently, when a physical therapist is confronted with this ambiguity, he or she may simply choose one side and provisionally start treating it; if after a few sessions the patient improves then it is assumed that the originally selected side was correct; in contrast, if after a few sessions a patient fails to improve, then the therapist may switch to the other side, at which point the patient should begin to improve. One should not “alternate” treatment sides, because treating a given side will “undo” whatever had been accomplished by treating the opposite side.
The first maneuver shown to treat lateral semicircular canal BPPV was described by Thomas Lempert (Lempert 1994) as the “barbecue roll;” some clinicians also refer to this as the “log roll.” Other maneuvers that have been less thoroughly studied include the Gufoni maneuver (Gufoni et al. 1998) and the Appiani maneuver (Ciniglio Appiani et al. 2005).
As noted earlier, lateral semicircular canal BPPV can cause either geotropic or apogeotropic direction changing positional nystagmus. Some studies report that both variants respond similarly to the Lempert maneuver and the Gufoni maneuver (Fu et al. 2020a, b). In contrast, some studies suggest that the geotropic and apogeotropic variants of lateral semicircular canal BPPV respond differently to different maneuvers; for instance, one randomized trial reported the Lempert maneuver and Gufoni maneuver to be effective specifically for geotropic lateral semicircular canal BPPV (Kim et al. 2012), while the original paper about the Appiani maneuver described it as efficacious specifically for apogeotropic lateral semicircular canal BPPV (Ciniglio Appiani et al. 2005).
References
Asprella Libonati G (2005) Diagnostic and treatment strategy of lateral semicircular canal canalolithiasis. Acta Otorhinolaryngol Ital 25: 277-83.
Asprella Libonati G (2012) Benign Paroxysmal Positional Vertigo and Positional Vertigo Variants. Otorhinolaryngology Clinics – An International Journal 4: 25-40. doi: 10.5005/jp-journals-10003-1085
Baloh RW, Jacobson K, Honrubia V (1993) Horizontal semicircular canal variant of benign positional vertigo. Neurology 43: 2542-9. doi: 10.1212/wnl.43.12.2542
Bhattacharyya N, Gubbels SP, Schwartz SR, Edlow JA, El-Kashlan H, Fife T, Holmberg JM, Mahoney K, Hollingsworth DB, Roberts R, Seidman MD, Steiner RW, Do BT, Voelker CC, Waguespack RW, Corrigan MD (2017) Clinical Practice Guideline: Benign Paroxysmal Positional Vertigo (Update). Otolaryngol Head Neck Surg 156: S1-S47. doi: 10.1177/0194599816689667
Choi S, Choi HR, Nahm H, Han K, Shin JE, Kim CH (2018) Utility of the bow and lean test in predicting subtype of benign paroxysmal positional vertigo. Laryngoscope 128: 2600-2604. doi: 10.1002/lary.27142
Choung YH, Shin YR, Kahng H, Park K, Choi SJ (2006) ‘Bow and lean test’ to determine the affected ear of horizontal canal benign paroxysmal positional vertigo. Laryngoscope 116: 1776-81. doi: 10.1097/01.mlg.0000231291.44818.be
Ciniglio Appiani G, Catania G, Gagliardi M, Cuiuli G (2005) Repositioning maneuver for the treatment of the apogeotropic variant of horizontal canal benign paroxysmal positional vertigo. Otol Neurotol 26: 257-60. doi: 10.1097/00129492-200503000-00022
Fu W, Han J, Chang N, Wei D, Bai Y, Wang Y, He F, Wang X (2020a) Corrigendum to “Immediate efficacy of Gufoni maneuver for horizontal canal benign paroxysmal positional vertigo (HC-BPPV): A meta-analysis” [Auris Nasus Larynx (2020) 48-54]. Auris Nasus Larynx 47: 171-172. doi: 10.1016/j.anl.2019.07.001
Fu W, Han J, Chang N, Wei D, Bai Y, Wang Y, He F, Wang X (2020b) Immediate efficacy of Gufoni maneuver for horizontal canal benign paroxysmal positional vertigo (HC-BPPV): a meta-analysis. Auris Nasus Larynx 47: 48-54. doi: 10.1016/j.anl.2019.05.002
Gufoni M, Mastrosimone L, Di Nasso F (1998) [Repositioning maneuver in benign paroxysmal vertigo of horizontal semicircular canal]. Acta Otorhinolaryngol Ital 18: 363-7.
Kim CH, Kim YG, Shin JE, Yang YS, Im D (2016) Lateralization of horizontal semicircular canal canalolithiasis and cupulopathy using bow and lean test and head-roll test. Eur Arch Otorhinolaryngol 273: 3003-9. doi: 10.1007/s00405-016-3894-8
Kim JS, Oh SY, Lee SH, Kang JH, Kim DU, Jeong SH, Choi KD, Moon IS, Kim BK, Kim HJ (2012) Randomized clinical trial for geotropic horizontal canal benign paroxysmal positional vertigo. Neurology 79: 700-7. doi: 10.1212/WNL.0b013e3182648b8b
Kim MW, Jin MH, Kim JK, Kwak MY (2023) Efficacy of the Head Rotation Test With Bowing for the Lateral Canal Benign Paroxysmal Positional vertigo. Otol Neurotol 44: 918-924. doi: 10.1097/MAO.0000000000003982
Koju G, Bing D, Zhou LQ, Mao ZY, Tao YL, Chen QG, Chen J, Liu Y, Tong T, Chu HQ (2022) Comparisons of Supine Roll Test and Alternative Positional Tests in HC-BPPV Lateralization. Curr Med Sci 42: 613-619. doi: 10.1007/s11596-022-2562-z
Kumar S, Gupta N, Dorasala S, Madaan P (2023) Bilateral Apogeotropic Lateral Canal BPPV: Role of Secondary Signs of Lateralization in Diagnosis. Indian J Otolaryngol Head Neck Surg 75: 3967-3970. doi: 10.1007/s12070-023-03976-y
Lee JB, Han DH, Choi SJ, Park K, Park HY, Sohn IK, Choung YH (2010) Efficacy of the “bow and lean test” for the management of horizontal canal benign paroxysmal positional vertigo. Laryngoscope 120: 2339-46. doi: 10.1002/lary.21117
Lempert T (1994) Horizontal benign positional vertigo. Neurology 44: 2213-4. doi: 10.1212/wnl.44.11.2213-a
Marcelli V (2016) Nystagmus intensity and direction in bow and lean test: an aid to diagnosis of lateral semicircular canal benign paroxysmal positional vertigo. Acta Otorhinolaryngol Ital 36: 520-526. doi: 10.14639/0392-100X-795
Martellucci S, Malara P, Castellucci A, Pecci R, Giannoni B, Marcelli V, Scarpa A, Cassandro E, Quaglieri S, Manfrin ML, Rebecchi E, Armato E, Comacchio F, Mion M, Attanasio G, Ralli M, Greco A, de Vincentiis M, Botti C, Savoldi L, Califano L, Ghidini A, Pagliuca G, Clemenzi V, Stolfa A, Gallo A, Asprella Libonati G (2020) Upright BPPV Protocol: Feasibility of a New Diagnostic Paradigm for Lateral Semicircular Canal Benign Paroxysmal Positional Vertigo Compared to Standard Diagnostic Maneuvers. Front Neurol 11: 578305. doi: 10.3389/fneur.2020.578305
McClure JA (1985) Horizontal canal BPV. J Otolaryngol 14: 30-5.
Pagnini P, Nuti D, Vannucchi P (1989) Benign paroxysmal vertigo of the horizontal canal. ORL J Otorhinolaryngol Relat Spec 51: 161-70. doi: 10.1159/000276052
![]()