By Marcello Cherchi, MD PhD
For patients
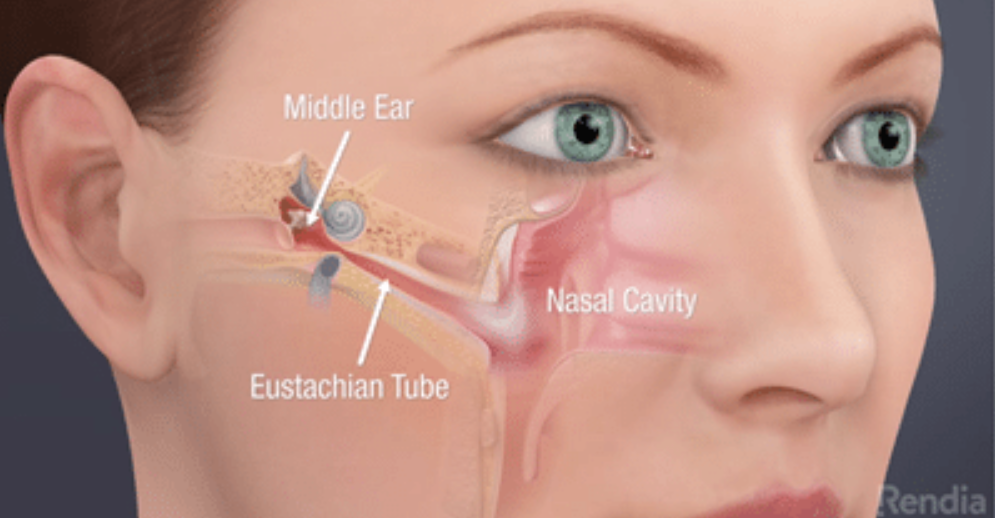
The Eustachian tube (ET) connects the middle ear (the space immediately behind the eardrum) with the back of the nose/throat. Its opening and closing serves to equalize pressure on both sides of the eardrum, and to protect the middle ear. ET dysfunction (ETD) can cause a variety of middle ear problems, including hearing loss. Diagnosis of ETD may be based on a combination of a patient’s history, physical examination, and sometimes tests or imaging. An otolaryngologist may offer a variety of treatments, from medical (oral or nasal decongestants) to surgical (balloon dilation, laser coagulation).
For clinicians
Overview
The pharyngotympanic tube, more commonly referred to as the Eustachian tube (ET), connects the middle ear with the nasopharynx. In the resting state the ET remains closed; it opens during co-contraction of the tensor veli palatini and the levator palatini muscles, which occurs during deglutition and yawning. Proper functioning of the ET serves to equalize pressure in the middle ear with the outside environment, to clear mucociliary secretions and pathogens from the middle ear, and to protect the middle ear and tympanic membrane. ET dysfunction (ETD) is sometimes classified into sub-types of (1) obstructive, (2) baro-challenge-induced, and (3) patulous. ETD can result from anatomical or functional abnormalities. Sequelae of ETD include middle ear effusions, infections, middle ear atelectasis, tympanic membrane retraction, development of cholesteatoma, and conductive hearing loss. There is no gold-standard test for ETD, so diagnosis usually relies on a combination of history, physical examination and testing (such as tympanometry), less commonly with procedures such as imaging or fiberoptic endoscopy. Treatments may include decongestants (oral or nasal), myringotomy/tympanostomy +/- placement of a grommet, Eustachian tuboplasty (with balloon dilatation or laser), and others, though none of these approaches is firmly supported by evidence-based studies, so prognosis is uncertain.
Introduction
The pharyngotympanic tube connecting the middle ear space with the nasopharynx is more commonly referred to as the Eustachian tube (ET), after Eustachio Bartolomeo who published a description of it in his anatomical treatise, Opuscula Anatomica in 1562 (Eustachio 1562).
Anatomy
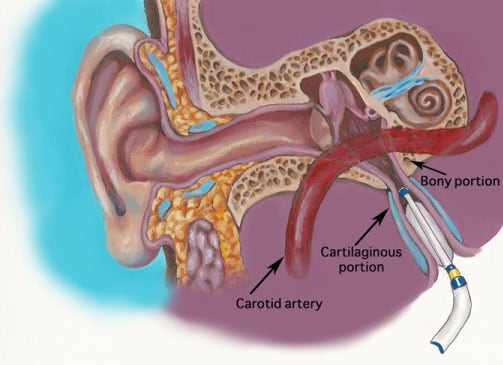
The Eustachian tube (ET) is situated in the para-pharyngeal region, proximal to the infratemporal fossa. It “acts as a void in fibroelastic cartilage” that “runs from the middle ear’s front wall to the sidewall of the nasopharynx” “along the pterygoid plate’s posterior edge” (Bal and Deshmukh 2022). The ET consists of a cartilaginous component (suspended from the skull base) that comprises about 2/3 of the length of the ET, and an osseous component that comprises about 1/3 of its length (Maddineni and Ahmad 2022).
The Figure below depicts the location and orientation of the right ET in an adult.
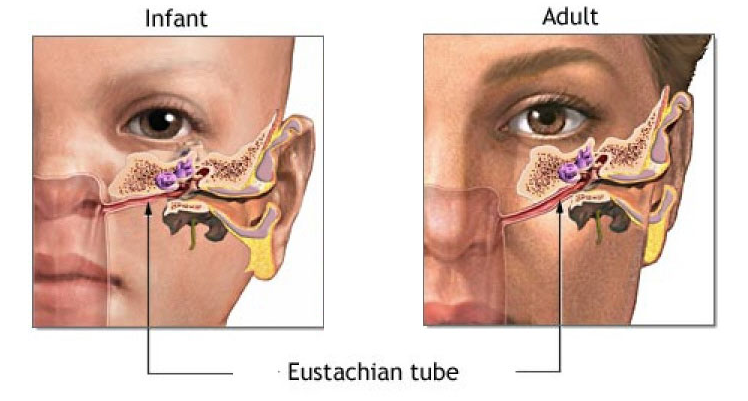
The Eustachian tube is oriented more horizontally in children than in adults, as shown in the Figure below.
Demographics
The prevalence of Eustachian tube dysfunction (ETD) is estimated at around 4 – 20% in the pediatric population. It is less common in adults; “there are an average of 0.77 adult visits for ETD for every pediatric visit” (Maddineni and Ahmad 2022). The higher prevalence of ETD in children is sometimes attributed to the relatively more horizontal orientation of the ET, one result of which is that gravity facilitates drainage less.
Factors in the pediatric population that can predispose to ETD include obstructive sleep apnea, and congenital malformations such as cleft palate (Maddineni and Ahmad 2022).
Physiology
The Eustachian tube “has two primary functions: balancing the pressure between the middle ear and the surroundings, and helping facilitate secretions from the middle ear, as well as protecting the ear from loud and potential sound hazards.” Other summaries regard the ET as serving three functions (Schilder, Bhutta et al. 2015, Bal and Deshmukh 2022):
- Pressure equalization and ventilation of the middle ear
- Mucociliary clearance of secretions from the middle ear
- Protection of the middle ear and eardrum from sounds, pathogens and secretions
The ET is lined by a “ciliated epithelium that enables mucociliary clearance of middle ear fluid while providing a barrier to the entry of pathogens from the nasopharynx” (Maddineni and Ahmad 2022).
The tensor veli palatini muscle, and the levator veli palatini muscle, when simultaneously contracted, dilate the Eustachian tube (Bal and Deshmukh 2022, Maddineni and Ahmad 2022). At rest the ET is collapsed; it “opens involuntarily during swallowing, but can also voluntarily open through swallowing or yawning” (Maddineni and Ahmad 2022).
Pathophysiology
A variety of processes can interfere with the function of the Eustachian tube, including (Bal and Deshmukh 2022):
- Anatomical abnormalities, such as:
- Reduced diameter (stenosis) due to inflammation or wall hypertrophy.
- Enlarged diameter (patulous Eustachian tube) due to slacking of the cartilage around the tube or the tissues.
- Elevated mucus production.
- Desquamation of the epithelium of the Eustachian tube.
The mechanisms by which Eustachian tube dysfunction (ETD) might bring about otologic dysfunction have been debated. Kim critically reviews the data pertaining to several such mechanisms, including stiffness effects, mass effects, window mechanics and vascular stress (Kim 2025).
There have been various proposals for classifying ETD, such as (Bal and Deshmukh 2022; Maddineni and Ahmad 2022; Schilder et al. 2015):
- Obstructive ETD. Often this is because the ET is “unable to effectively dilate. The most common reason for the impairment of ET dilation is the inflammation of the mucosa of the cartilaginous ET” from upper respiratory tract infections, reflux, or allergy (Maddineni and Ahmad 2022). Some investigators postulate three sub-categories of obstructive ETD (Schilder, Bhutta et al. 2015):
- Functional obstruction.
- Dynamic dysfunction (muscular failure).
- Anatomical obstruction.
- Baro-challenge-induced ETD, “when there is an ambient pressure change in the environment” (Bal and Deshmukh 2022). Common scenarios include “deep-sea diving or descent from high altitudes” (Maddineni and Ahmad 2022).
- Patulous (dilatory) ETD, “characterized by an excessively patent ET that does not sufficiently constrict” (Maddineni and Ahmad 2022). This is less common than obstructive ETD, and “the majority of cases of patulous ETD do not have a clear etiology” (Maddineni and Ahmad 2022).
Some common pathophysiologic consequences of ETD include middle ear effusions and infections, atelectasis of the middle ear with tympanic membrane retraction, tympanic membrane damage, development of cholesteatoma, and conductive hearing loss (Bal and Deshmukh 2022, Maddineni and Ahmad 2022).
Clinical history
While each sub-type of ETD may have its own characteristics, in general symptoms suggesting ETD include, “pressure in the ear, aural fullness; popping, pain, or discomfort in the ear; muffled hearing; and autophony” (Maddineni and Ahmad 2022).
Regarding the characteristics of the various subtypes (Schilder, Bhutta et al. 2015, Maddineni and Ahmad 2022):
- Obstructive ETD: “Can present with aural fullness, pain, altered or muffled hearing, and tinnitus.”
- Baro-challenge-induced ETD: “Patients may only experience the aural symptoms [aural fullness, pain, muffled hearing] during situations of rapid pressure changes, especially with exposure to high pressures.”
- Patulous ETD: “can present with positional autophony, audible breathing, pulsatile tinnitus that synchronizes with breathing, a sense of pressure in the ear, and hearing loss.”
Diagnosis: by history
Questionnaire-based assessments, such as the Eustachian Tube Dysfunction Questionnaire 7 (ETDF‑7) have also been explored (McCoul, Anand et al. 2012). This questionnaire involves summation scoring of questions pertaining to seven parameters of “pressure in ears,” “pain in ears,” “clicking sound on swallowing,” “underwater/clogged sensation,” “ringing in ears,” “muffled hearing” and “pre-occurring cold/sinusitis,” all reported by the patient.
There have also been attempts at developing scoring systems that include both subjective categories and objective testing (from tubomanometry or tympanometry), such as the Eustachian Tube Scoring (ETS‑7) (Schroder, Lehmann et al. 2015).
Diagnosis: physical examination
Various physical examination maneuvers, such as the Valsalva maneuver and the Toynbee test, have been studied, but are not reliable. The Valsalva maneuver involves attempting to exhale against a closed mouth and nose in order to drive air distally through the ET into the middle ear; if during this maneuver the examiner observes movement of the tympanic membrane then the test is considered “positive.” The Toynbee test has the patient swallow while the nostrils are pinched closed; if during this maneuver the examiner observes movement of the tympanic membrane then the test is considered “positive.” Unfortunately these are, “non-dependable confirmatory diagnostic test[s]” (McCoul, Anand et al. 2012).
Diagnosis: otologic testing
There is a long history of intermittent enthusiasm for tympanometry in the diagnosis of ETD (Givens and Seidemann 1984), but this has not been universally accepted, as some studies show it to have very limited diagnostic utility (Virtanen and Marttila 1982).
More technologically elaborate diagnostic methods have included video nasopharyngoscopy (Chauhan and Chauhan 2013).
Diagnosis: imaging
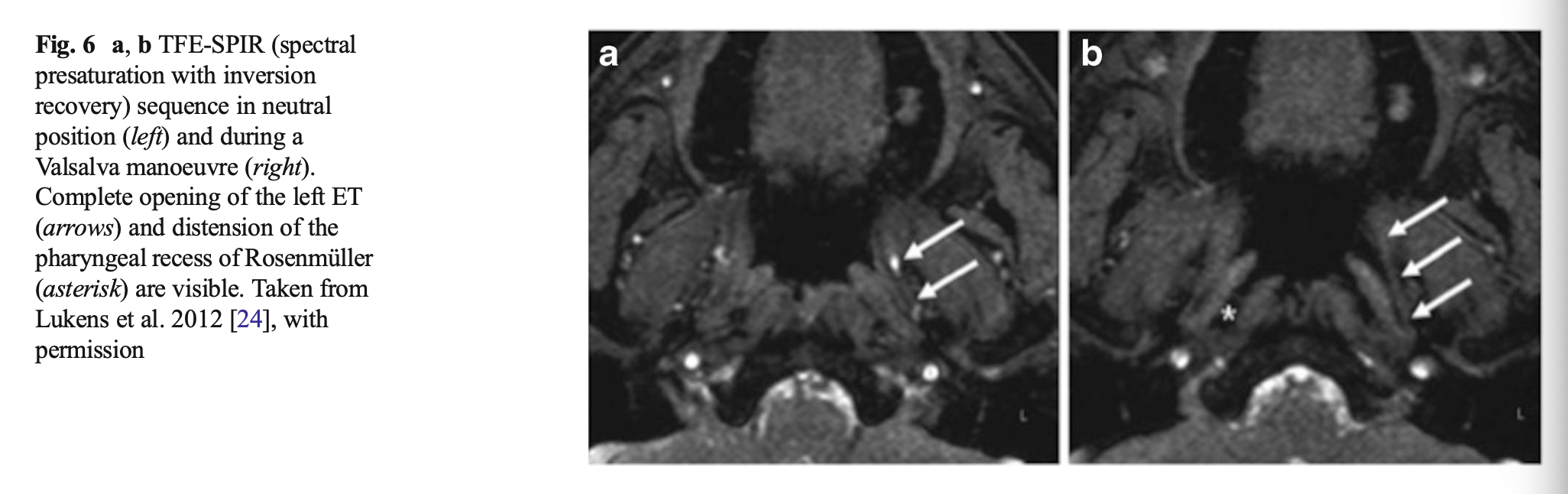
Imaging modalities of CT and MRI have been explored for diagnosing ETD (Smith, Scoffings et al. 2016), but none has proven reliably diagnostic (Maddineni and Ahmad 2022).
The Figure below from Smith and colleagues (Smith, Scoffings et al. 2016) shows an MRI from a healthy volunteer at rest (panel a) and during Valsalva (panel b), demonstrating that Valsalva opens the Eustachian tube.
The Figure below from Smith and colleagues (Smith, Scoffings et al. 2016) shows a CT of a patulous Eustachian tube.

Diagnosis: Fiberoptic endoscopy
One study reported videonasopharyngoscopy as a, “highly accurate and reliable test for Eustachian tube function as compared to tympanometry” (Chauhan and Chauhan 2013).
Diagnosis: overall
Multiple authors have noted that there does not yet exist a “gold standard” test for proof-positive diagnosis of ETD (Smith and Tysome 2015, Bal and Deshmukh 2022, Maddineni and Ahmad 2022), and that “more work is required to validate… Eustachian tube function tests” (Smith, Bance et al. 2019).
Absent a definitive test, diagnosis has traditionally relied upon a combination of history, physical examination, otoscopy, and sometimes tympanometry (Bal and Deshmukh 2022).
Treatment
Despite diagnostic uncertainty, a range of treatments have been attempted.
The most common initial approach usually involves oral decongestants or nasal spray decongestants. Evidence of efficacy is weak or lacking (Llewellyn, Norman et al. 2014, Norman, Llewellyn et al. 2014), but the risk is low, so this is a first approach for many clinicians.
Myringotomy/tympanostomy involves making a small incision in the tympanic membrane. Because such incisions usually heal shut relatively rapidly, the otolaryngologist may place a grommet, also called a “tympanostomy tube” or “ventilation tube.” A meta-analysis reported favorable outcomes (Llewellyn, Norman et al. 2014), though some find the effect to be minimal (Lous, Burton et al. 2005) or zero (Knight and Hilger 1993).
Eustachian tuboplasty, which may involve “point laser coagulation of superior and posterior margin of ET nasopharyngeal opening.” A meta-analysis of 7 case series (192 patients) of Eustachian laser tuboplasty reported, “Eustachian tuboplasty using various techniques (seven case series, 182 patients) was associated with improvement in symptoms in 36-92% of patients. Improvements in hearing (four studies) were small with limited clinical significance. Three studies documented low rates (13-36%) of conversion to type A tympanogram” (Norman, Llewellyn et al. 2014).
Balloon Eustachian tuboplasty. This involves passing a catheter with a balloon at its end which, when inflated, dilates the ET. A meta-analysis reported favorable outcomes (Llewellyn, Norman et al. 2014).
 |
 |
Microwave ablation. Preliminary studies have explored microwave ablation Eustachian tuboplasty (Lou, Lou et al. 2021), which targets “the ET orifice’s hypertrophic tissue” (Bal and Deshmukh 2022).
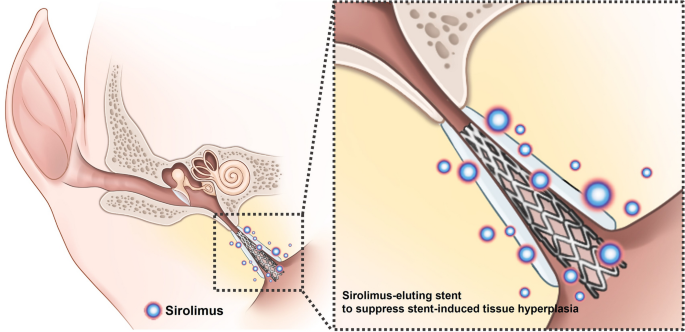
Research on Eustachian tube stenting is conducted in animal models, but the risk of a stent is that it can convert an obstructive dysfunction ET into a patulous dysfunction ET. The Figure below depicts placement of a sirolimus-eluting stent in the ET of a pig (Kang, Kim et al. 2022).
For the most part, meta-analyses of interventions for ETD reach disappointing conclusions such as, “It is not possible to draw conclusions regarding the effectiveness of any of the interventions for the treatment of adults with an ETD diagnosis, and there is insufficient evidence to recommend a trial of any particular intervention” (Llewellyn, Norman et al. 2014), and “Eustachian tube dysfunction is a poorly defined condition. Due to the limited and poor-quality evidence, it is inappropriate to make conclusions on the effectiveness of any intervention; the evidence base is insufficient to guide recommendations for a trial of any particular intervention” (Norman, Llewellyn et al. 2014).
Prognosis
A meta-analysis of outcomes from treatment techniques (Llewellyn, Norman et al. 2014) noted that the overall quality of evidence was “limited in quantity and overall was of poor quality,” but suggested that:
- “Based on a single RCT, nasal steroids showed no improvement.”
- “Single trials fount two pressure equalization devices were each associated with significant short-term improvements in symptoms, middle ear function and/or hearing.”
- Eustachian tubpoplasty (seven case series) and balloon dilatation (three case series) were associated with improved outcomes.”
- “Positive results were also reported for myringotomy (two case series).”
References
Bal R, Deshmukh P (2022) Management of Eustachian Tube Dysfunction: A Review. Cureus 14: e31432. doi: 10.7759/cureus.31432
Chauhan B, Chauhan K (2013) A comparative study of eustachian tube functions in normal and diseased ears with tympanometry and videonasopharyngoscopy. Indian J Otolaryngol Head Neck Surg 65: 468-76. doi: 10.1007/s12070-011-0312-9
Eustachio B (1562) Epistola de auditus organis [Letter concerning the hearing organ]. Opuscula Anatomica. Lugduni Batavorum, Apud Johannem vander Linden, pp 125-142
Givens GD, Seidemann MF (1984) Acoustic immittance testing of the Eustachian tube. Ear Hear 5: 297-9. doi: 10.1097/00003446-198409000-00006
Kang JM, Kim SH, Choi YJ, Park Y, Ryu DS, Kang WS, Park JH, Park HJ (2022) Sirolimus-eluting cobalt-chrome alloy stent suppresses stent-induced tissue hyperplasia in a porcine Eustachian tube model. Sci Rep 12: 3436. doi: 10.1038/s41598-022-07471-2
Kim HY (2025) Eustachian Tube Dysfunction in Hearing Loss: Mechanistic Pathways to Targeted Interventions. Biomedicines 13. doi: 10.3390/biomedicines13112686
Knight LC, Hilger A (1993) The effects of grommet insertion on Eustachian tube function. Clin Otolaryngol Allied Sci 18: 459-61. doi: 10.1111/j.1365-2273.1993.tb00613.x
Llewellyn A, Norman G, Harden M, Coatesworth A, Kimberling D, Schilder A, McDaid C (2014) Interventions for adult Eustachian tube dysfunction: a systematic review. Health Technol Assess 18: 1-180, v-vi. doi: 10.3310/hta18460
Lou Z, Lou Z, Sun J, Chen Z, Yin S (2021) Microwave ablation eustachian tuboplasty: a preliminary investigation with long-term follow-up. J Otolaryngol Head Neck Surg 50: 39. doi: 10.1186/s40463-021-00520-2
Lous J, Burton MJ, Felding JU, Ovesen T, Rovers MM, Williamson I (2005) Grommets (ventilation tubes) for hearing loss associated with otitis media with effusion in children. Cochrane Database Syst Rev: CD001801. doi: 10.1002/14651858.CD001801.pub2
Maddineni S, Ahmad I (2022) Updates in Eustachian Tube Dysfunction. Otolaryngol Clin North Am 55: 1151-1164. doi: 10.1016/j.otc.2022.07.010
McCoul ED, Anand VK, Christos PJ (2012) Validating the clinical assessment of eustachian tube dysfunction: The Eustachian Tube Dysfunction Questionnaire (ETDQ-7). Laryngoscope 122: 1137-41. doi: 10.1002/lary.23223
Norman G, Llewellyn A, Harden M, Coatesworth A, Kimberling D, Schilder A, McDaid C (2014) Systematic review of the limited evidence base for treatments of Eustachian tube dysfunction: a health technology assessment. Clin Otolaryngol 39: 6-21. doi: 10.1111/coa.12220
Schilder AG, Bhutta MF, Butler CC, Holy C, Levine LH, Kvaerner KJ, Norman G, Pennings RJ, Poe D, Silvola JT, Sudhoff H, Lund VJ (2015) Eustachian tube dysfunction: consensus statement on definition, types, clinical presentation and diagnosis. Clin Otolaryngol 40: 407-11. doi: 10.1111/coa.12475
Schroder S, Lehmann M, Sauzet O, Ebmeyer J, Sudhoff H (2015) A novel diagnostic tool for chronic obstructive eustachian tube dysfunction-the eustachian tube score. Laryngoscope 125: 703-8. doi: 10.1002/lary.24922
Smith ME, Bance ML, Tysome JR (2019) Advances in Eustachian tube function testing. World J Otorhinolaryngol Head Neck Surg 5: 131-136. doi: 10.1016/j.wjorl.2019.08.002
Smith ME, Scoffings DJ, Tysome JR (2016) Imaging of the Eustachian tube and its function: a systematic review. Neuroradiology 58: 543-556. doi: 10.1007/s00234-016-1663-4
Smith ME, Tysome JR (2015) Tests of Eustachian tube function: a review. Clin Otolaryngol 40: 300-11. doi: 10.1111/coa.12428
Virtanen H, Marttila T (1982) Middle-ear pressure and eustachian tube function. Arch Otolaryngol 108: 766-8. doi: 10.1001/archotol.1982.00790600010003
![]()