By Marcello Cherchi, MD PhD
For patients
Tympanometry is an ear test that helps in the diagnosis of several conditions of the middle ear. During this test the audiologist or technician will insert a special earbud first in one ear, and then in the other ear. You may or may not hear some sounds when the earbud is in place. The test is not uncomfortable. It takes less than a minute. If you have ear wax, this should be removed before the test; otherwise there are no special preparations for the test. There are no specific instructions for what to do after the test.
For clinicians
Overview
Tympanometry is an easy, brief otologic procedure that measures peak immittance and middle ear pressure, and indirectly calculates ear canal volume. These results are helpful in diagnosing a variety of middle ear problems.
Introduction
Tympanometry as used today is descended from impedance audiometry (Klockhoff 1961; Metz 1946). Contemporary practice uses the Liden-Jerger classification, developed by Gunnar Lidén (Liden 1969; Lidén et al. 1970) and James Jerger (Jerger 1970).
Physiology and anatomy
Davies lays out the terminology relevant for understanding tympanometry:
“Tympanometry, or measurement of the acoustic immittance of the ear, obtains information about the state of the middle ear as a function of ear canal pressure. Acoustic immittance represents the difficulty encountered by a sound wave (acoustic energy) as it is transmitted through the ear. ‘Stiffness’ of the ear is the characteristic that maintains its shape and brings about restoration after a force has been applied. Compliance is the reciprocal of stiffness and represents the mobility of the middle-ear system. Acoustic immittance identifies high-impedance middle-ear abnormalities, e.g., otitis media and otosclerosis, and low-impedance abnormalities such as ossicular interruption” (Davies 2016).
The mobility of the eardrum is affected by several factors, of which the pressure differential (between the external auditory canal and the middle ear) is one that can be experimentally manipulated. When the pressure differential is zero (i.e., pressures on each side of the tympanic membrane are equal), then the tympanic membrane should be at its most mobile. When the middle ear pressure is greater than the external auditory canal pressure the tympanic membrane “bulges out;” in contrast when the middle ear pressure is less than the external auditory canal pressure the tympanic membrane is “sucked in” (retracted); in these states the tympanic membrane is relatively less mobile (compared to when there is no pressure differential).
At the time tympanometry is performed the middle ear space has a specific pressure that is not (yet) known. A tympanometric probe is inserted into the external auditory canal and forms a hermetic seal, such that the external auditory canal is an air-tight space (assuming that the tympanic membrane is not perforated). The tympanometric probe has three orifices: (1) a channel through which a static pressure can be delivered and maintained; (2) a channel through which sound can be delivered (a “speaker”); (3) a channel through which sound can be received (a “microphone”). These are illustrated in the Figure below, from Jerger (Jerger 1970).

At a given level of static pressure, the “speaker” generates a tone at a specific frequency (most commercial devices use 226 Hz) and amplitude, which reflects off the eardrum and is received by the “microphone.” The difference between the amplitude of the original stimulus and the amplitude of the received signal helps calculate the compliance (mobility) of the eardrum, in the following manner.
If the tympanic membrane is extremely stiff (non-compliant), then the kinetic energy of the acoustic stimulus will not make it move; that energy will instead be reflected back to the microphone, and the amplitude of the received signal will be equal to the amplitude of the original acoustic stimulus.
In contrast, if the tympanic membrane is very “floppy,” then some of the kinetic energy of the acoustic stimulus will be “absorbed” by making the tympanic membrane move, and the signal that returns to the microphone will be of lower amplitude.
In tympanometry the level of static pressure is systematically varied; when that static pressure equals that of the middle ear, then the tympanic membrane should be at its most compliant (“floppiest”), whereas when the static pressure is different from middle ear pressure, the tympanic membrane should be less compliant.
Thus, tympanometry plots the degree of compliance as a function of external auditory canal pressure. The height (along the Y‑axis) of the resultant peak reveals the maximum tympanic membrane compliance. The location of that peak along the X‑axis shows the middle ear pressure (inferred from the external auditory canal pressure).
Finally, tympanometry can calculate what is called the “equivalent canal volume.” Davies (Davies 2016) explains this as follows:
“When the EAM [external auditory meatus] pressure is at MEP [middle ear pressure], the measured compliance is primarily that of the air in the EAM plus that of the middle-ear structures. If the EAM pressure is increased significantly above MEP (e.g., MEP + 200 mmH2O), the measured compliance of the middle-ear structures becomes very small in comparison to the air in the EAM, and the measured compliance is approximately equal to that of the air in the EAM. If this value is subtracted from the maximum compliance obtained when MEP equals EAM pressure, this difference will be approximately equal to the compliance of the middle ear. Normal values range from 0.3 to 1.5 mL of equivalent volume” (Davies 2016).
In other words, the difference between the lowest obtainable impedance and the highest obtainable impedance enables an indirect calculation of ear canal volume, though this is approximate (Shanks and Lilly 1981).
Equipment needed
A tympanometer is needed for performing tympanometry. Many devices are commercially available.
How to perform the test
The audiologist or technician inserts the probe into the external auditory canal and attempts to form a hermetic seal. If a seal is achieved, then the tympanometer can be run, and it automatically collects data to generate a tympanogram. The test is usually performed once in each ear. In some (but not all) laboratories, tympanometry is a regular part of a standard audiometry evaluation.
What this test assesses
Tympanometry plots the degree of tympanic membrane compliance (along the Y‑axis) as a function of a specific pressure applied to the external auditory canal. As such, tympanometry reveals three important pieces of information: (1) the maximum compliance of the tympanic membrane; (2) middle ear pressure; and (3) information that permits indirect calculation of ear canal volume.
How to interpret the test results
The six main categories of tympanograms are shown in the composite plot in the Figure below, from Nakayama and Ramsey (Nakayama and Ramsey 2013).
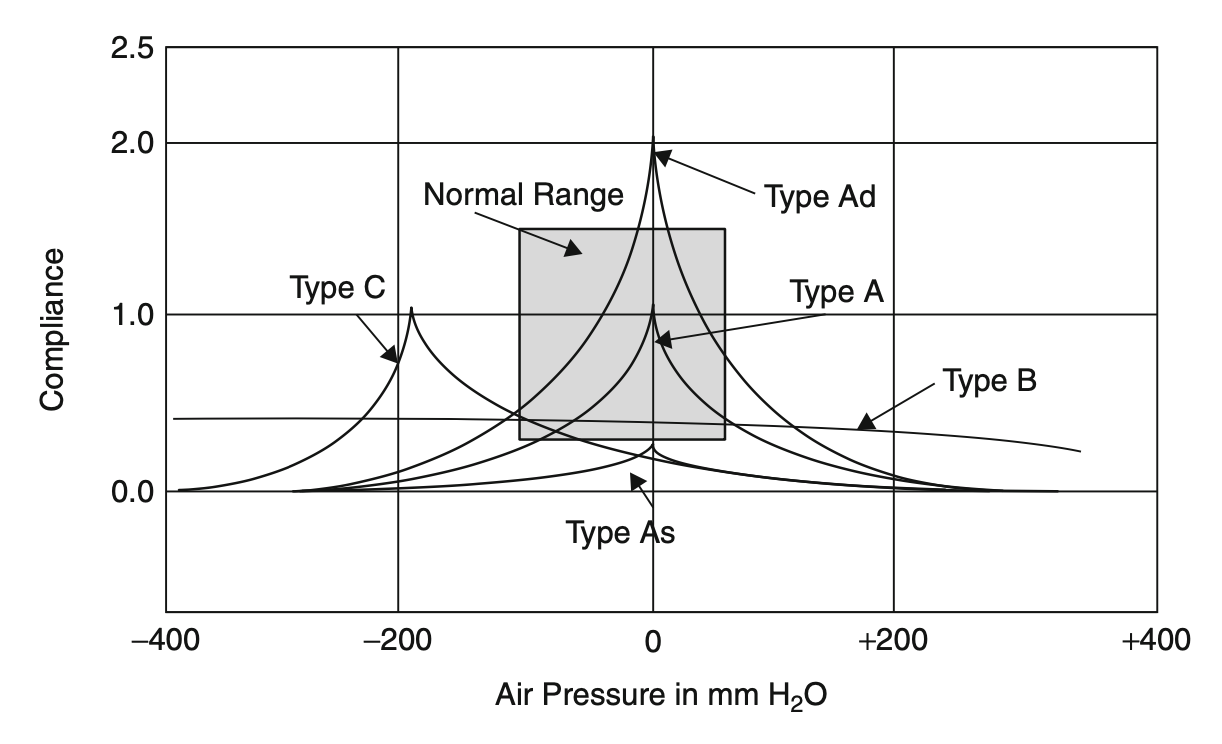
The Table below reviews the main categories of tympanograms.
|
Type |
Description of plot |
Parameters |
Differential diagnosis |
|
A |
Normal. |
Peak immittance is at or near zero middle ear pressure. |
|
|
AD |
“Deep” (the plots in original studies of Liden and Jerger were inverted). |
Unusually high peak of maximum compliance. |
|
|
AS |
“Shallow” (the plots in original studies of Liden and Jerger were inverted). |
Unusually low peak of maximum compliance. |
|
|
B |
“Flat,” i.e., no clear compliance peak. |
Absent, or nearly absent, peak of maximum compliance. Reflects little or no mobility of tympanic membrane. |
|
|
C |
Negative peak pressure. |
Peak of compliance occurs at negative middle ear pressure. |
|
|
D |
“Notched.” |
Hypermobile tympanic membrane. |
|
|
E |
Broad, smooth notch. |
|
Table: Liden-Jerger classification of tympanograms.
The equivalent canal volume (ECV), though only approximate (Shanks and Lilly 1981), can still be helpful. An abnormally large ECV suggests a tympanic membrane perforation (because the result actually reflects the combined volume of the external auditory canal and the middle ear). An abnormally small ECV may be compatible with a total cerumen impaction.
Limitations
If a patient’s external auditory canal is shaped in such a way that a tympanometric probe cannot form a hermetic seal, then the test results will be uninterpretable.
Contraindications
Nakayama and Ramsey (Nakayama and Ramsey 2013) list several contraindications to tympanometry, including the presence of a foreign body in the external auditory canal, discomfort of the ear, otitis externa, and recent otologic surgery.
Pitfalls
If the tympanometric probe cannot achieve a hermetic seal with the walls of the external auditory canal, then the test will yield uninterpretable results.
When is the test indicated
Nakayama and Ramsey (Nakayama and Ramsey 2013) list several indications for tympanometry, including suspected or known disorders of the tympanic membrane, and hearing disorders.
When a standard audiogram shows a significant air-bone gap, this suggests conductive or mixed hearing loss. In this circumstance, tympanometry is useful in confirming the conductive component of the hearing loss.
Our practice is to check tympanometry prior to invasive audiologic procedures in order to assess integrity of the tympanic membrane.
Diseases that may be diagnosed by this test
Tympanometry is helpful in confirming the conductive component of hearing loss, and in identifying tympanic membrane perforations. Decreased peak immittance alerts the clinician to certain middle ear conditions (e.g., middle ear effusions, ossicular chain fixation), while increased peak immittance suggests other middle ear conditions (e.g., ossicular chain discontinuity).
Additional notes
Tympanometry is also part of other assessments, such as checking acoustic (stapedial) reflexes.
References
Davies RA (2016) Audiometry and other hearing tests. Handb Clin Neurol 137: 157-76. doi: 10.1016/B978-0-444-63437-5.00011-X
Jerger J (1970) Clinical experience with impedance audiometry. Arch Otolaryngol 92: 311-24. doi: 10.1001/archotol.1970.04310040005002
Klockhoff IHs (1961) Middle ear muscle reflexes in man: a clinical and experimental study with special reference to diagnostic problems in hearing impairment, Stockholm
Liden G (1969) The scope and application of current audiometric tests. J Laryngol Otol 83: 507-20. doi: 10.1017/s0022215100070651
Lidén G, Peterson JL, Björkman G (1970) Tympanometry. Arch Otolaryngol 92: 248-57. doi: 10.1001/archotol.1970.04310030038009
Metz O (1946) The acoustic impedance measured on normal and pathological ears: orientating studies on the applicability of impedance measurement in otological diagnosis. E. Munksgaard, Copenhagen
Nakayama JR, Ramsey MJ (2013) Tympanometry. In: Kountakis SE (ed) Encyclopedia of Otolaryngology, Head and Neck Surgery. Springer Berlin Heidelberg, Berlin, Heidelberg, pp 2905-2909
Shanks JE, Lilly DJ (1981) An evaluation of tympanometric estimates of ear canal volume. J Speech Hear Res 24: 557-66. doi: 10.1044/jshr.2404.557
![]()